,%20bone%20defect.jpg)
,%20trimmed,%20bone%20graft.jpg)


|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Narrow Long Implant Placed Deep
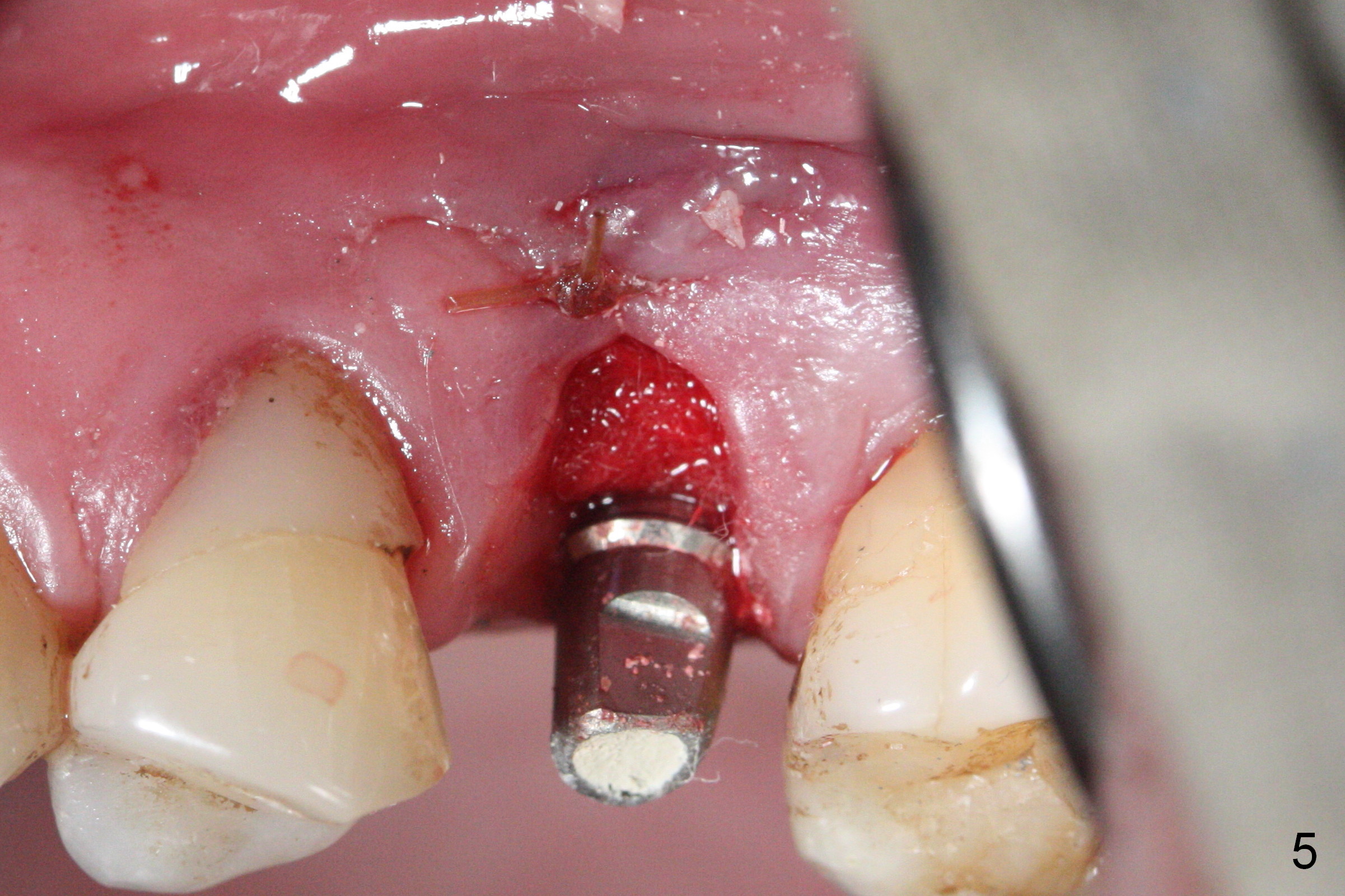
When the fractured root from the smoke-reducing patient is being removed by a root tip pick, the buccal gingiva is lacerated, partially due to loss of the buccal plate. Later suturing is required (Fig.5).
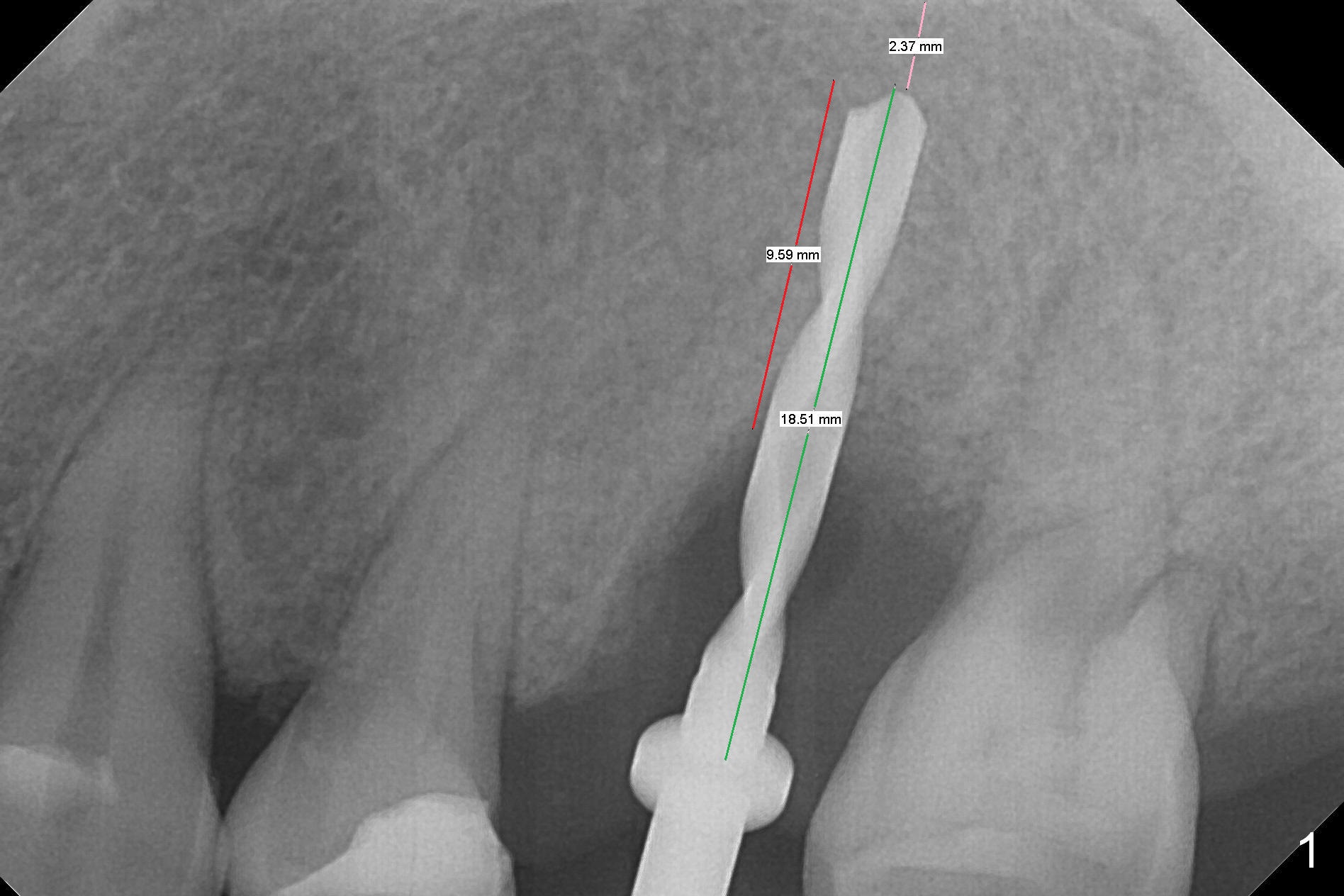
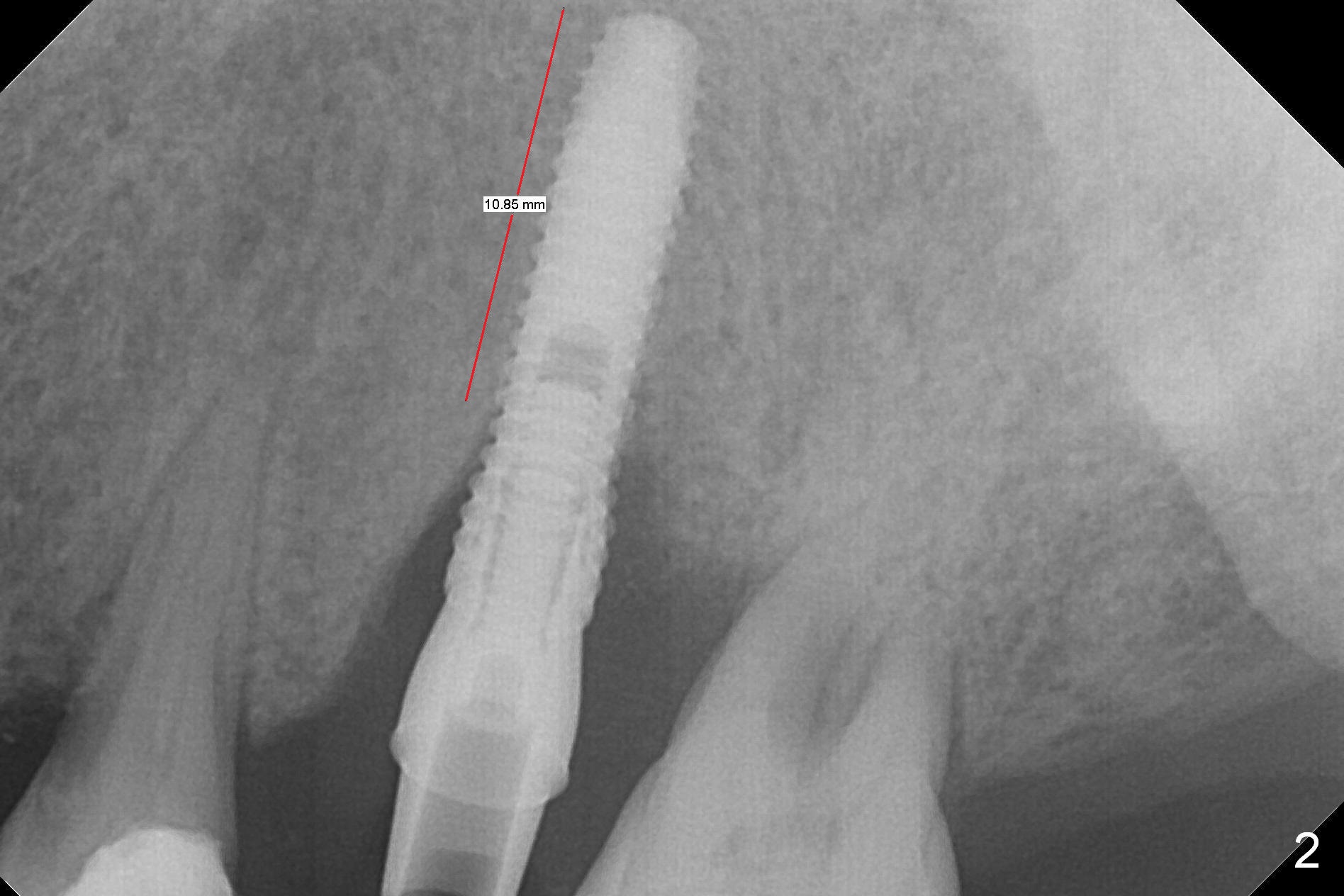
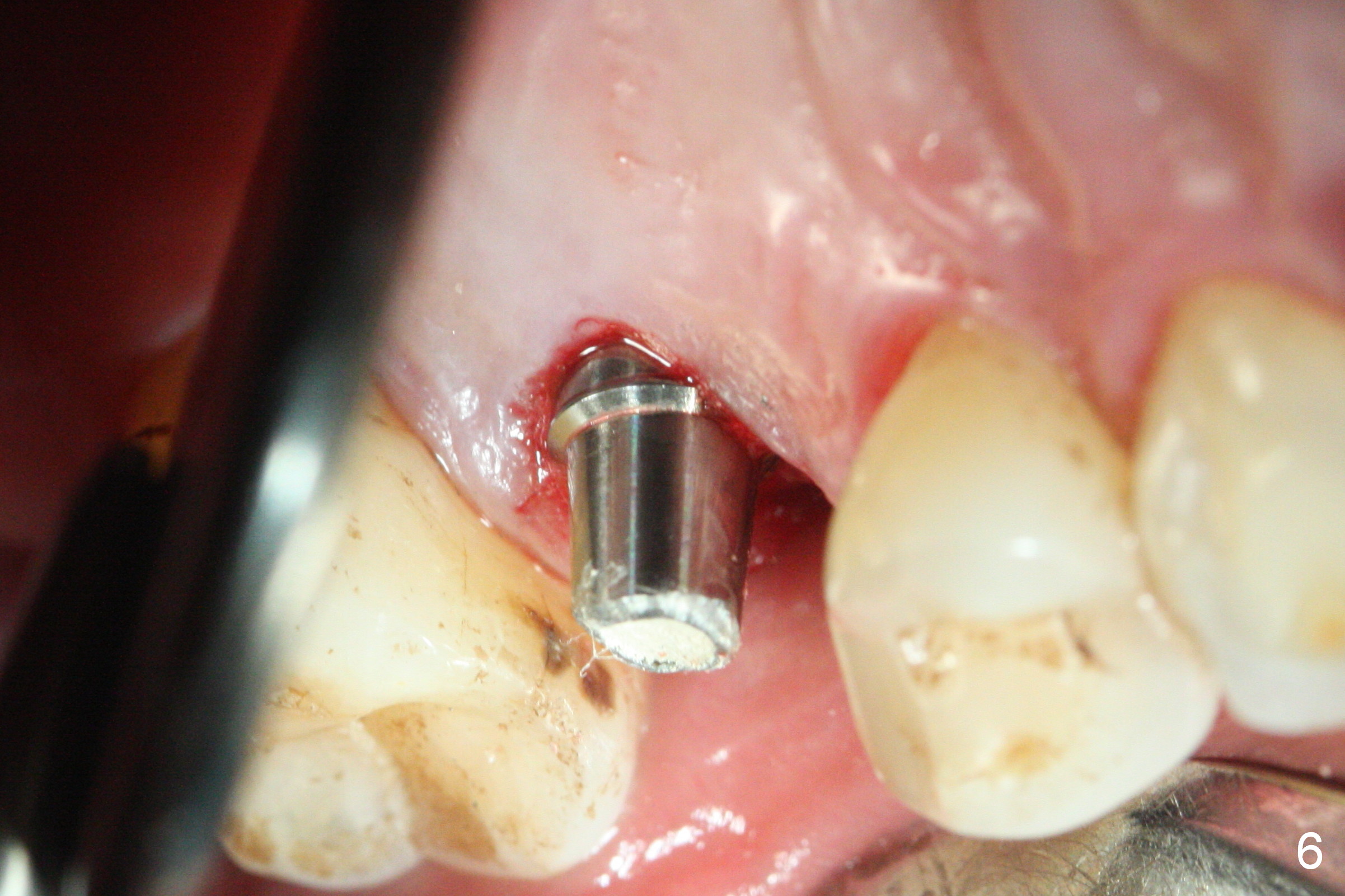
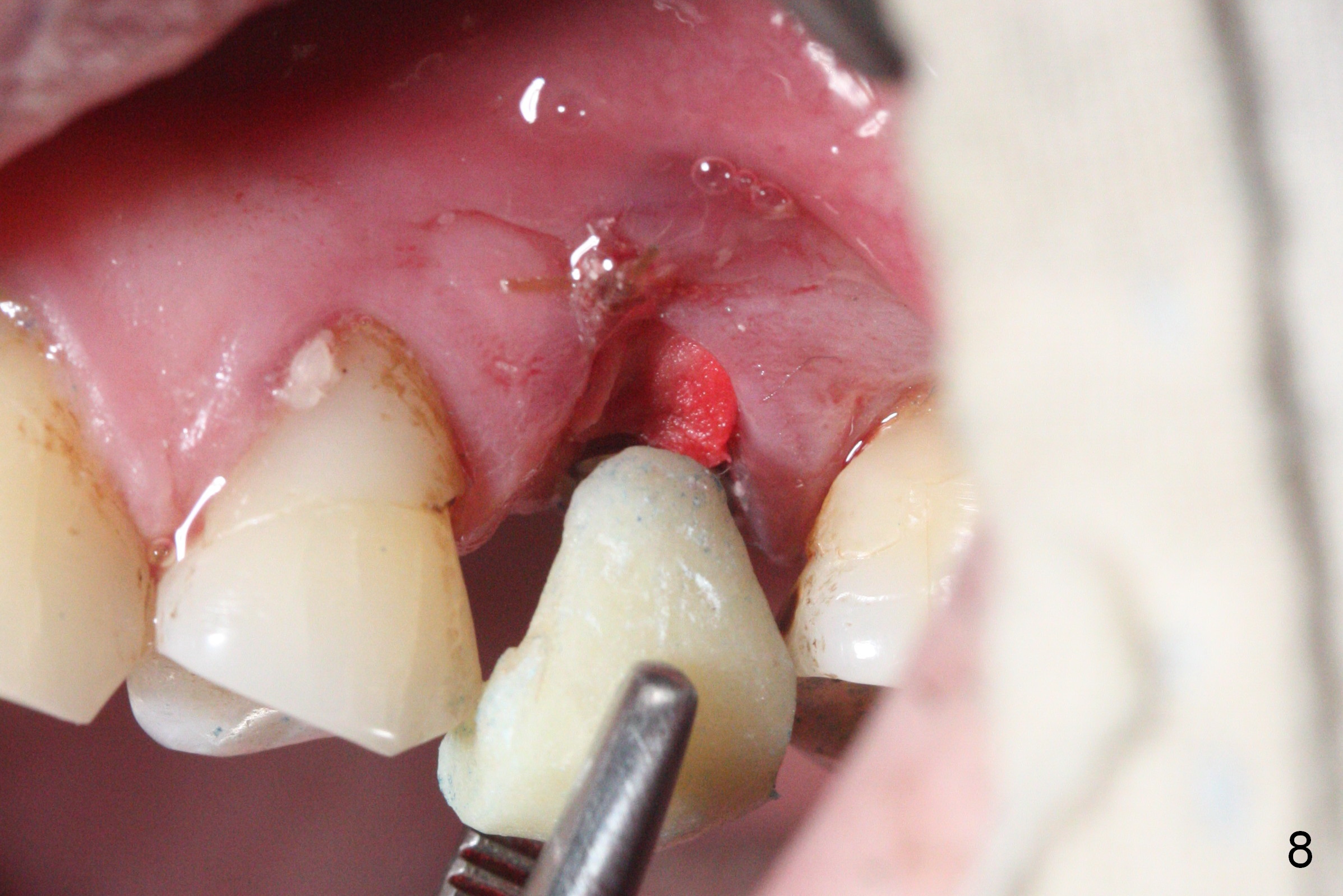
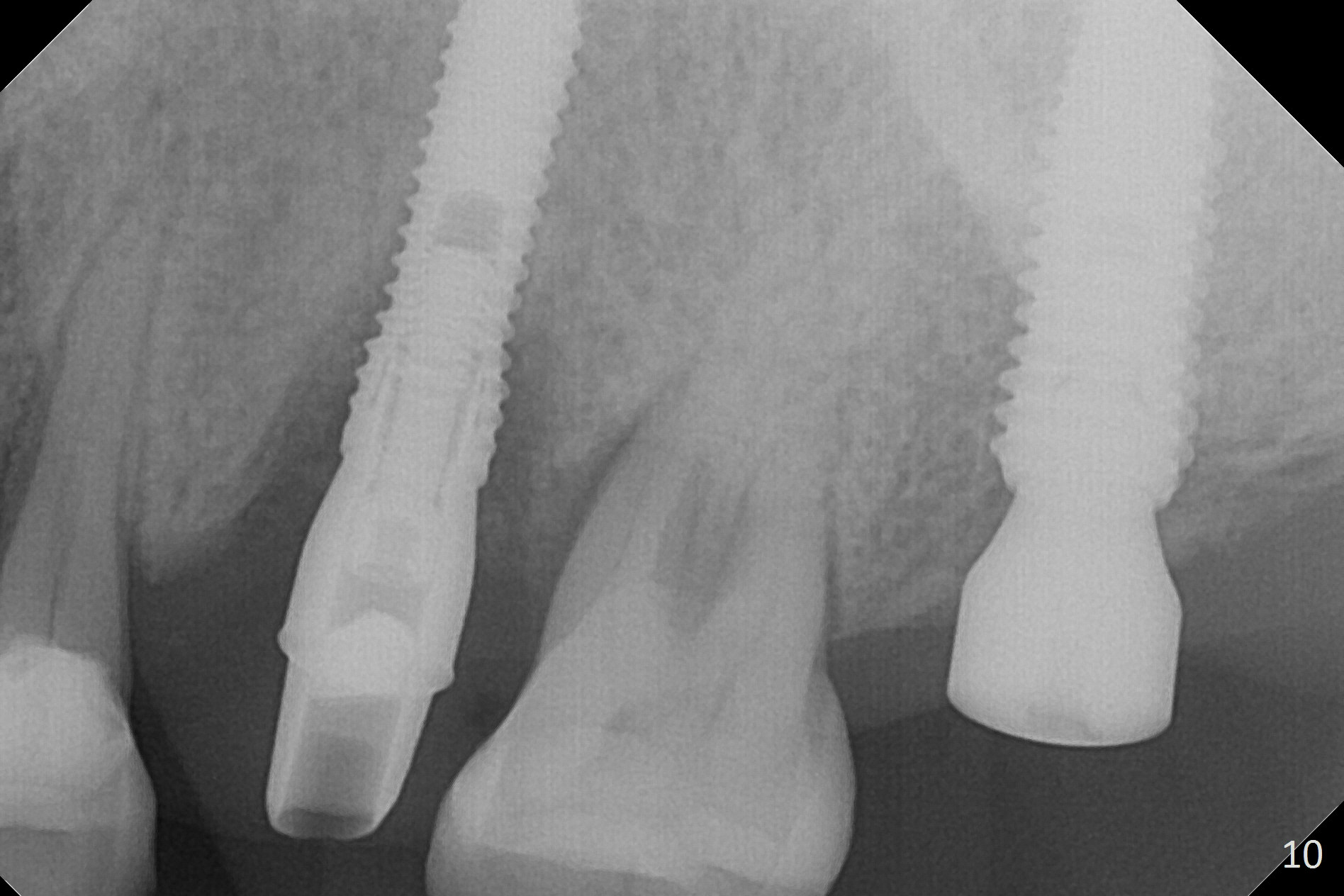
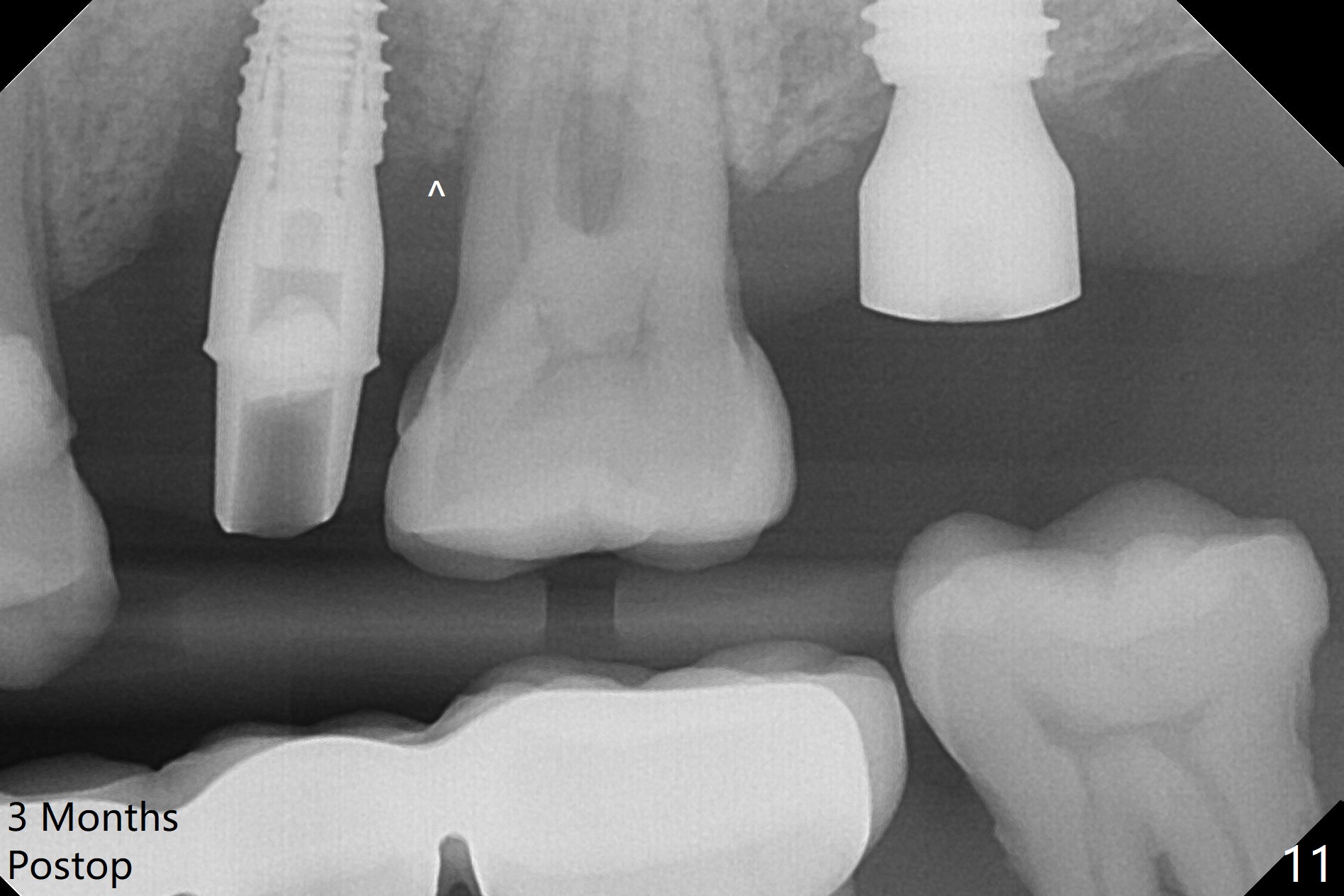
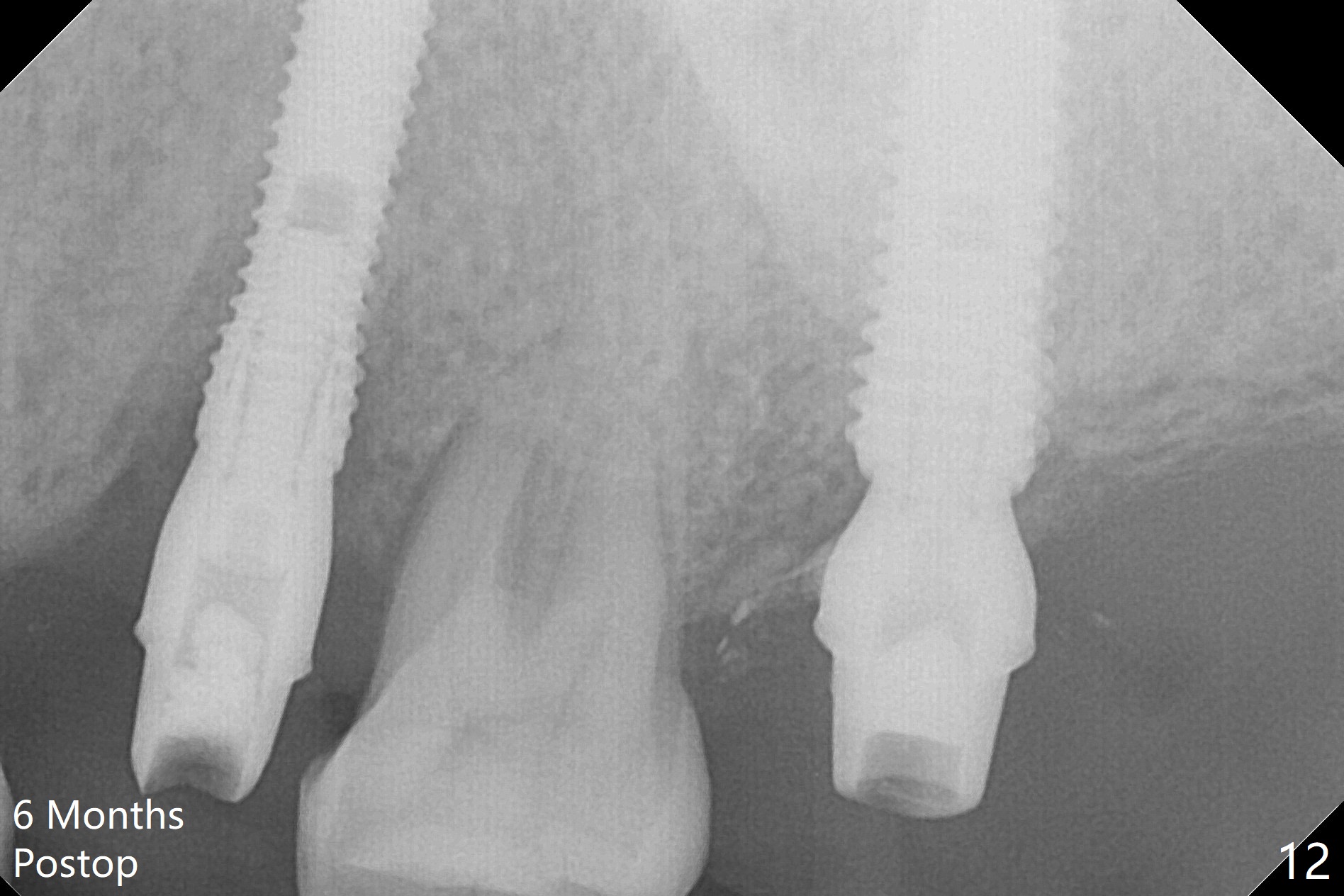
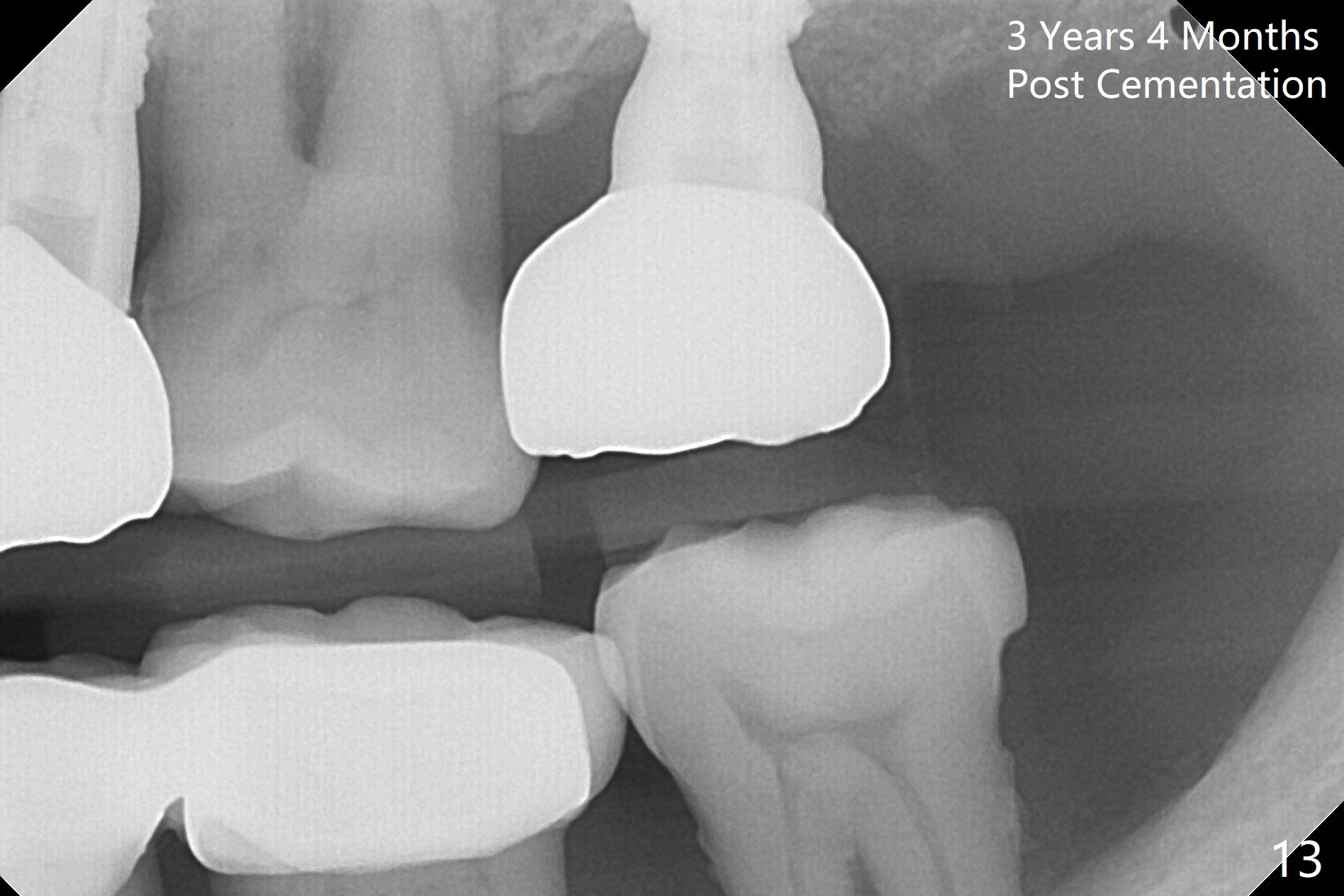
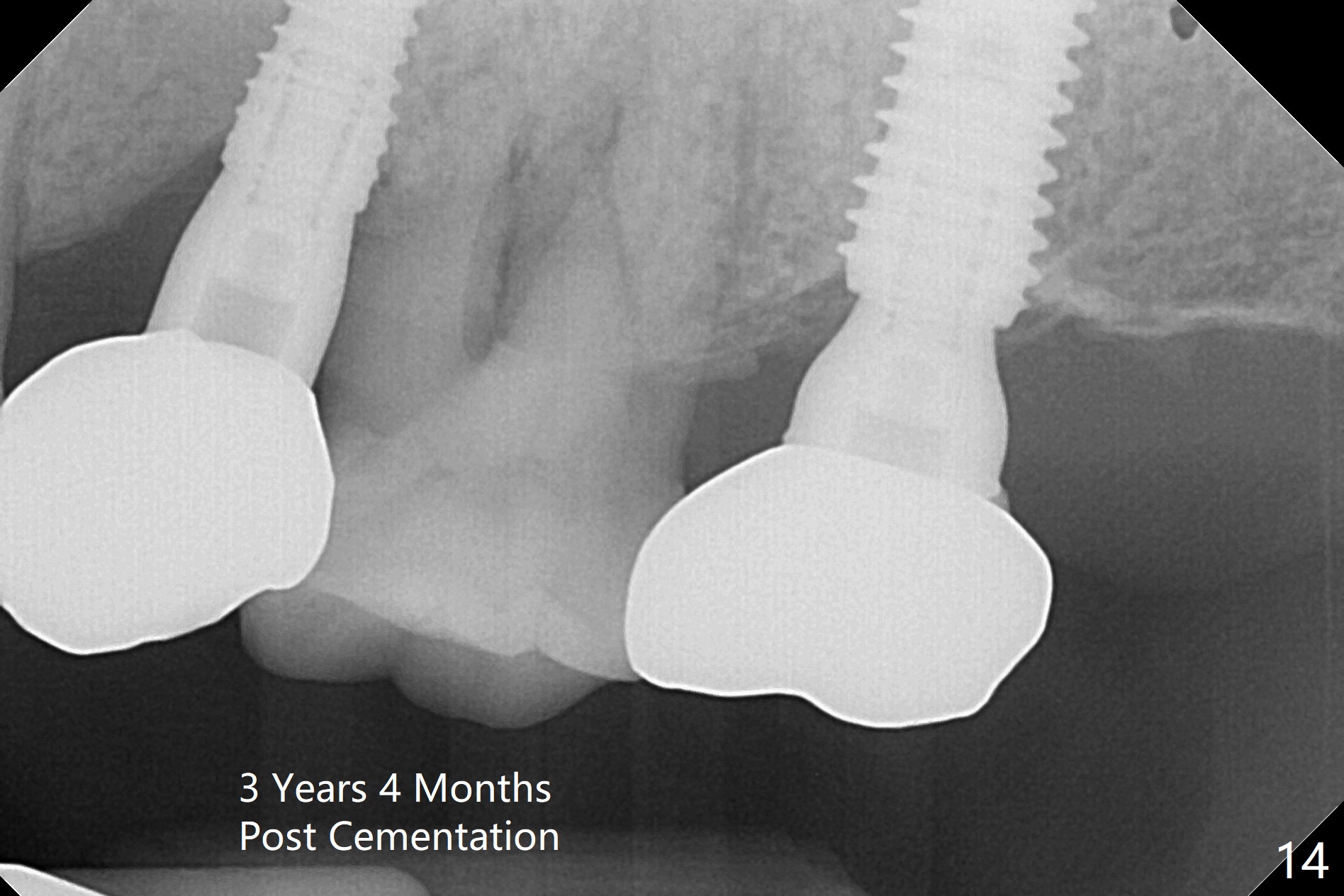
Initial osteotomy depth is 18 mm (Fig.1 green line) with 9 mm in the native bone (red line). The bone density feels to be low. There is at least 2 more mm bone apically (pink line). The depth is increased by 2 mm so that when a 3.8x15 mm implant is placed, there is 10-11 mm implant/bone contact (Fig.2 red line). There is large bony defect (Fig.3 *), which is bone grafted (Fig.4 *). Finally a longer abutment is placed (4.5x5.5(5) in Fig.4 vs. 4.5x4(5) in Fig.2,3). The 5 mm cuff does not look too long buccally (Fig.5) or palatally (Fig.6). To prevent postop buccal gingival overgrowth (2), the buccal margin of an immediate provisional is subgingival (Fig.7-9 *). Bone density between #13 and 14 appears to increase 3 months postop (Fig.10). The implant seems to be equi-crestal (Fig.11 ^). There seems to be more bone growth (i.e., decreasing gap) 6 months postop (Fig.12). Impression is taken. A crown is delivered nearly 7 months postop (08/07/2017). While there is minimal bone loss at #13 and 15 three years and 4 months post cementation, the tooth #14 and 18 are mobile (Fig.13,14).
Return to
Upper
Premolar Immediate Implant, IBS,
#15 (surgery),
31 (surgery)
Xin Wei, DDS, PhD, MS 1st edition 02/03/2017, last revision 12/01/2020