
,%20VeraGraft.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|||
Short or Long Implant?
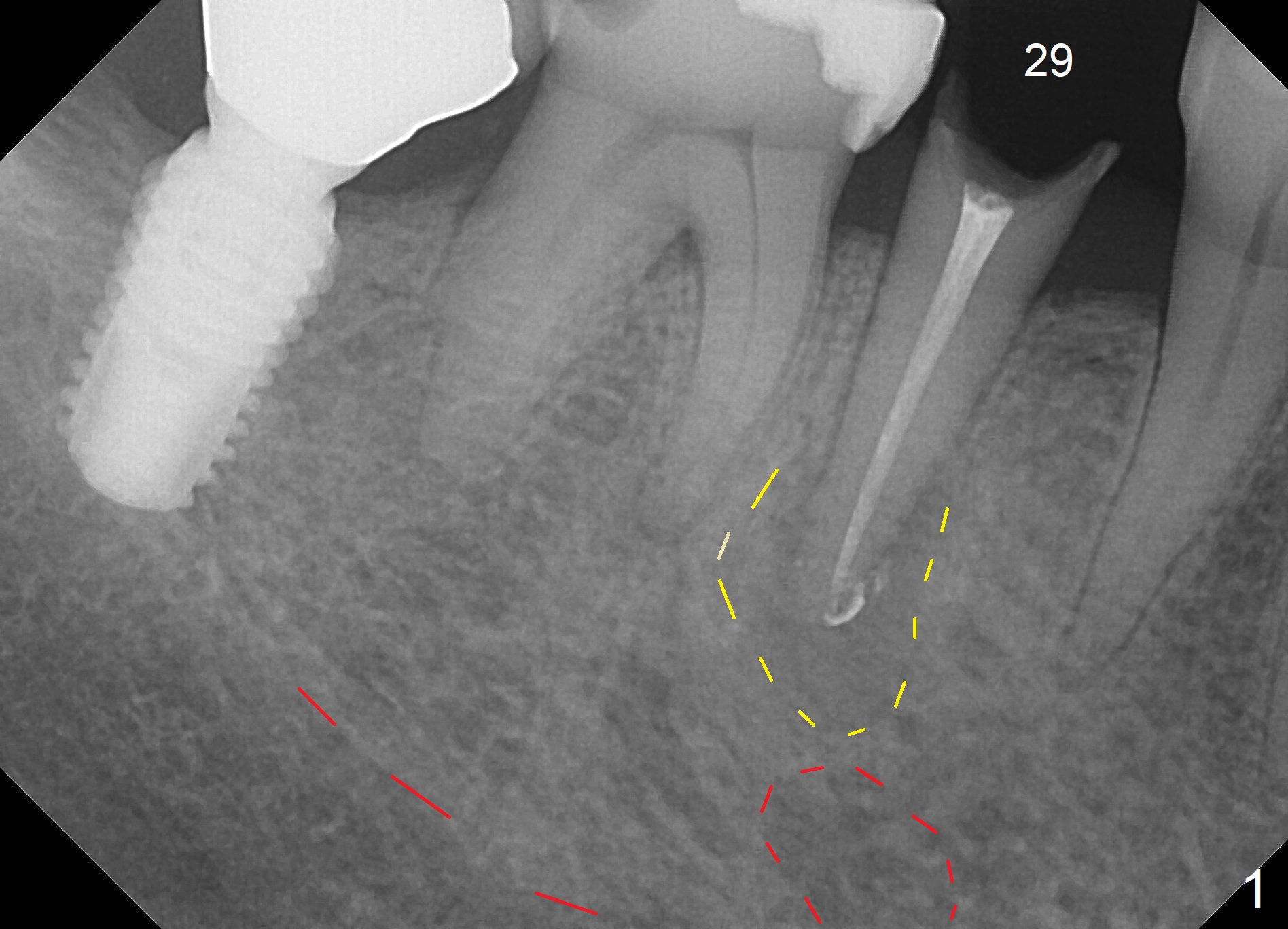
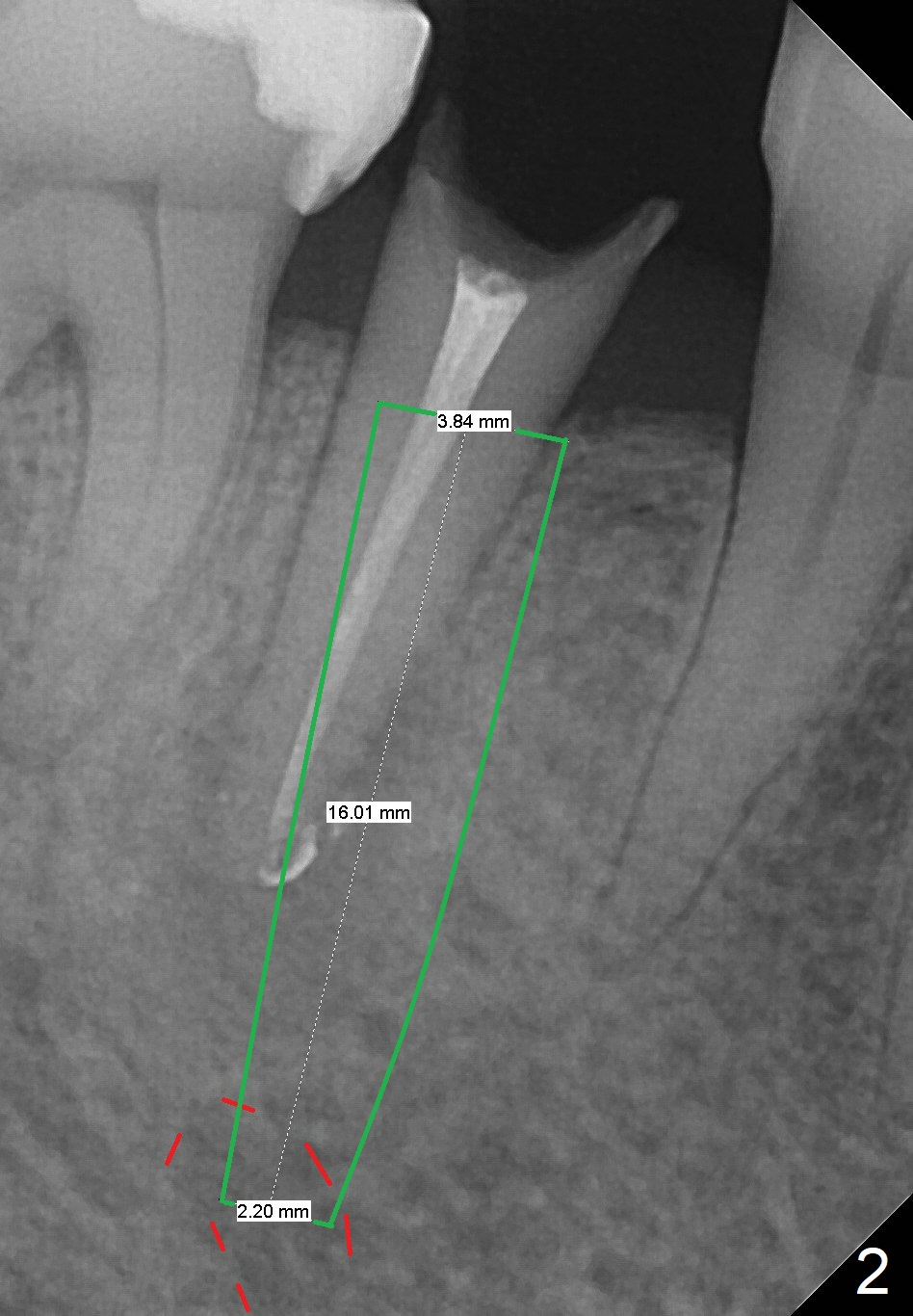
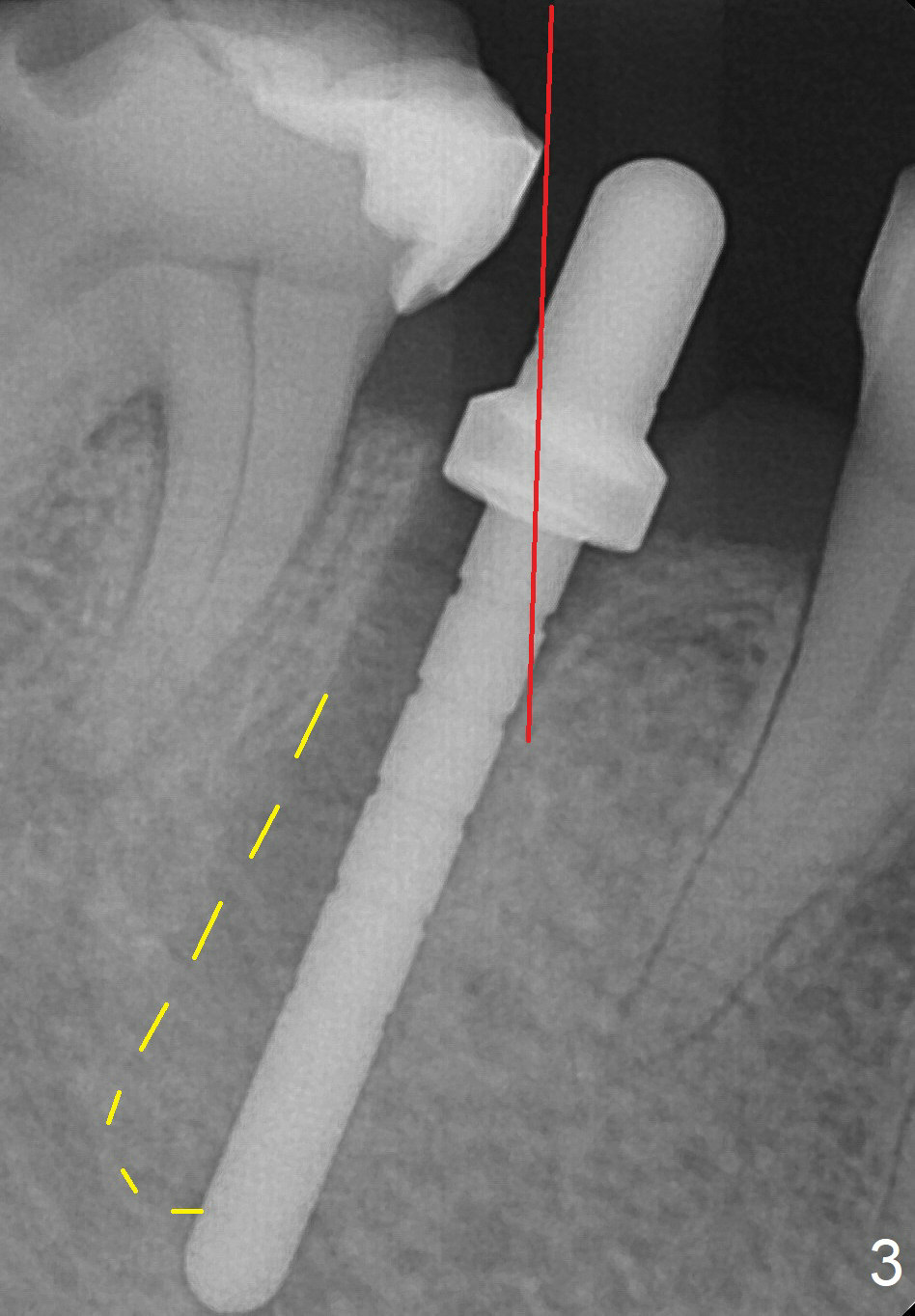
A 67-year-old woman fractures the tooth #29 three months post RCT. There is persistent periapical radio-lucency (Fig.1 yellow dashed line), which is close to the Mental Loop (red dashed line). Since the root of the affected tooth deviates distal, osteotomy will be established mesial (Fig.2). In fact it is not so easily accomplished; the osteotomy is initiated as mesial as possible (Fig.3 (yellow dashed line: original socket)). When a 3.8x16 mm implant is being placed, it is distal (Fig.4). The MO composite of the tooth #30 has to be trimmed for fabrication of an immediate provisional (Fig.5 <).
To place the implant mesially, the initial osteotomy should be established higher in the mesial slope of the socket (Fig.3 red line). Once the drill penetrates the lamina dura (Fig.5 short black line), change the trajectory (Fig.5 red line). A potential drawback may be loss of primary stability when osteotomy increases.
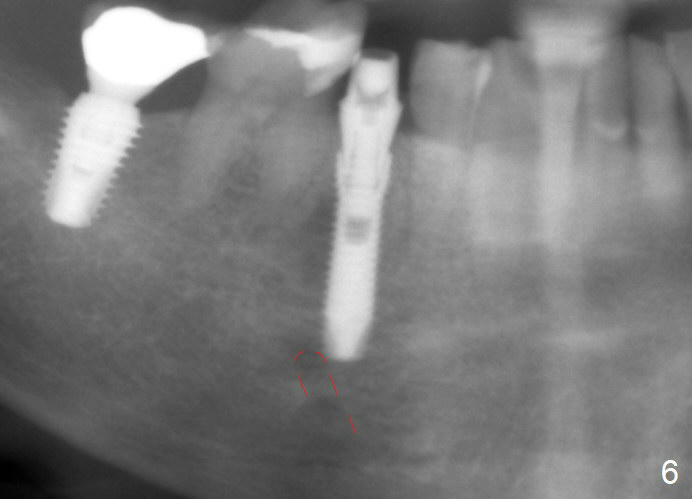
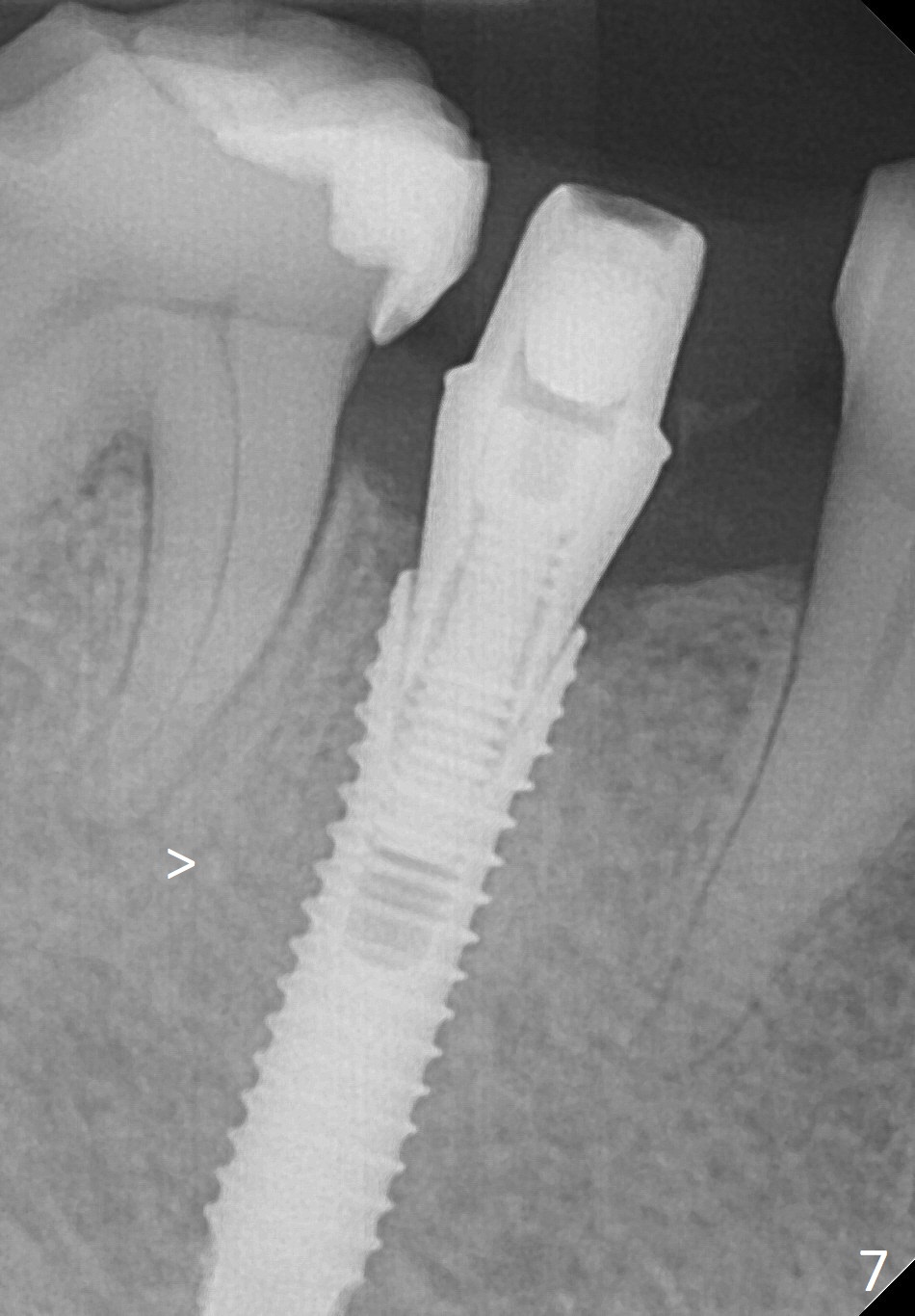
To reduce the chance to injury the buccally located loop, the osteotomy should be as lingual as possible. Initial depth is 19 mm (gingival level, Fig.3). In fact all of the three intraop PAs (Fig.3-5) do not show the Mental Loop until panoramic X-ray is taken immediately postop (Fig.6). There is no postop paresthesia. There appears no gap around the implant 3.5 months postop (Fig.7 >).
Return to
Lower Premolar Immediate
Implant, IBS
Xin Wei, DDS, PhD, MS 1st edition 07/25/2017, last revision 11/29/2017