
.jpg)


|
|
|
|
||
|
|
|
|
|
|
|
|
||||
Dense Bone
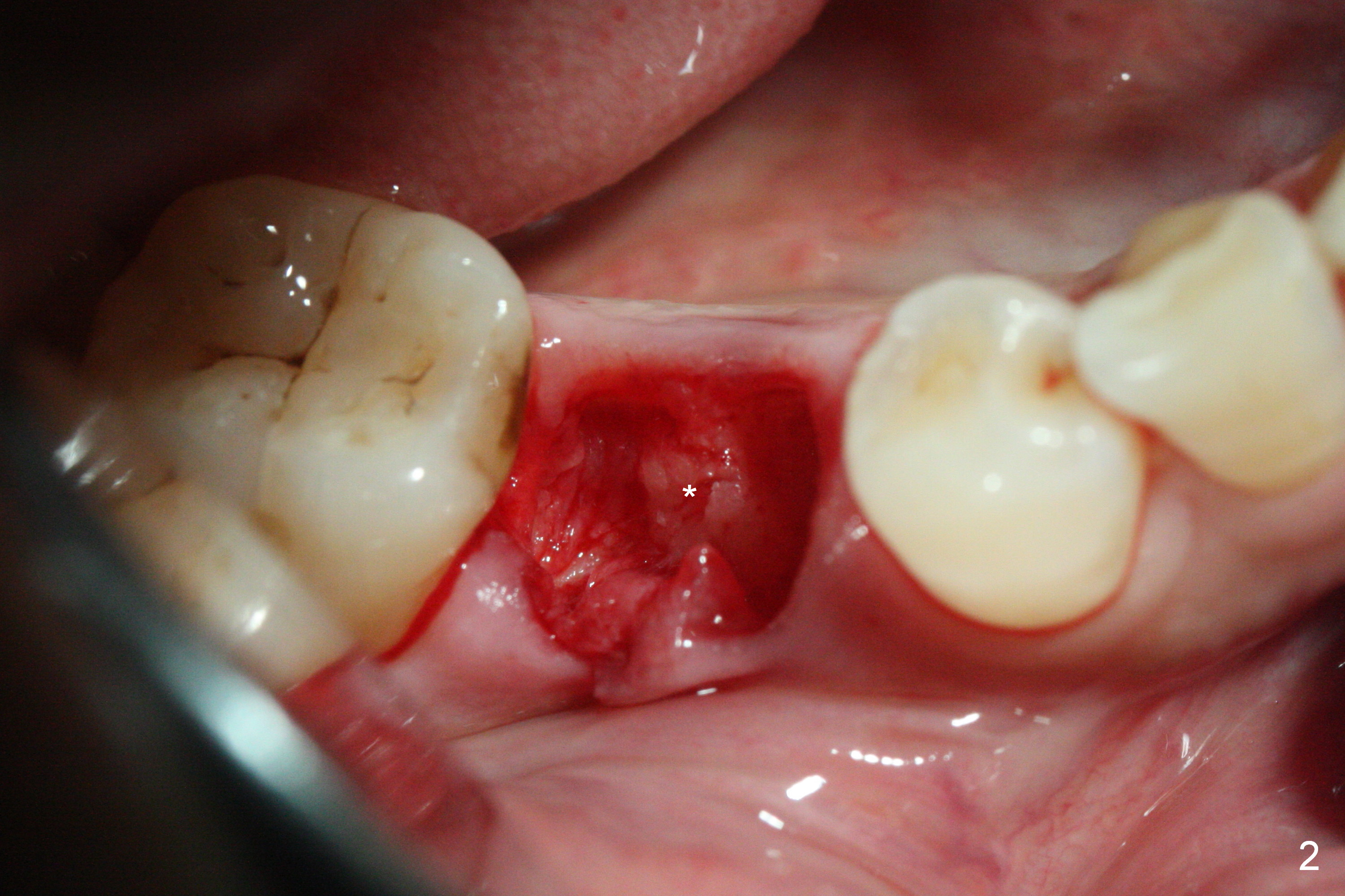
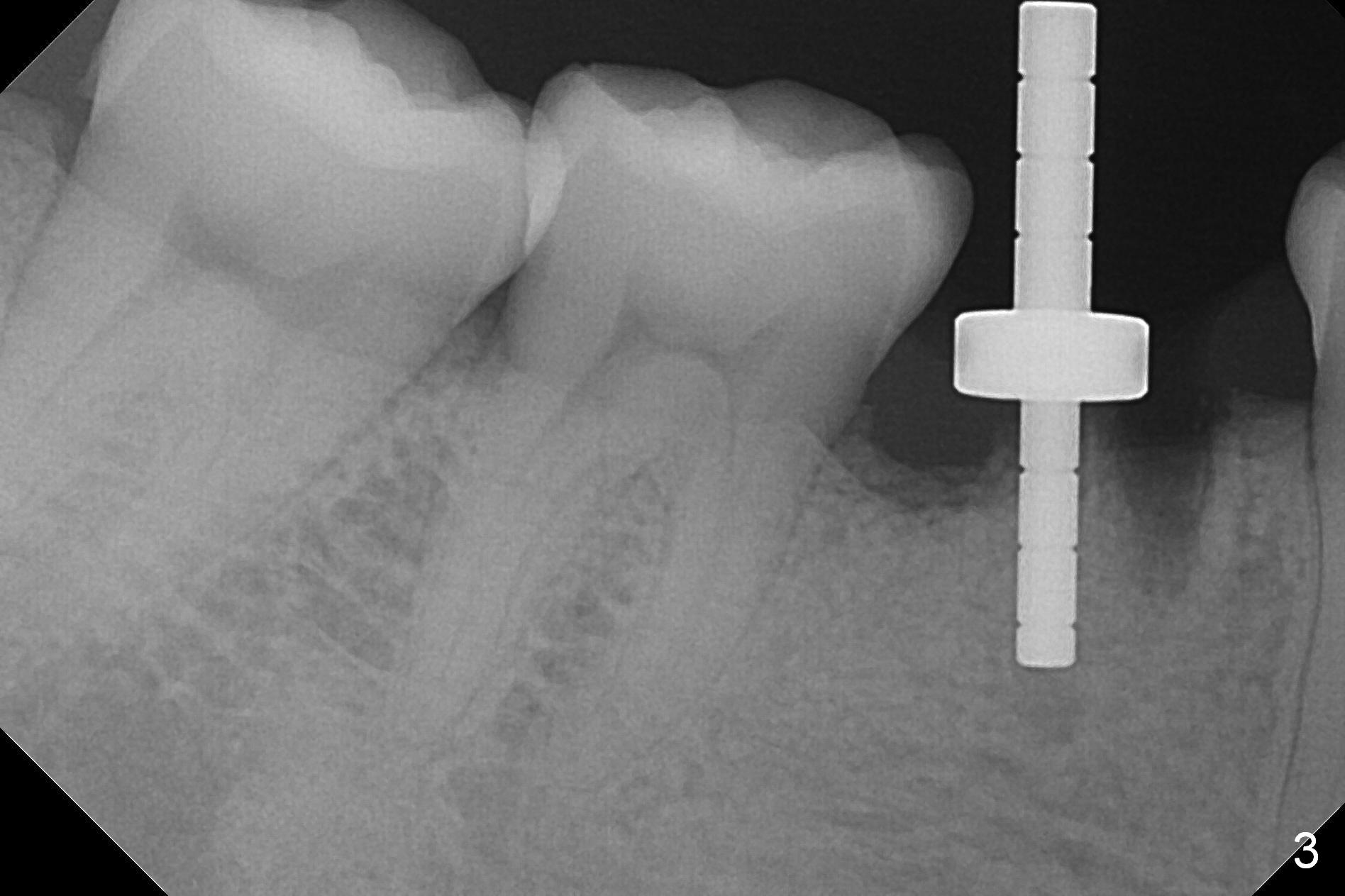
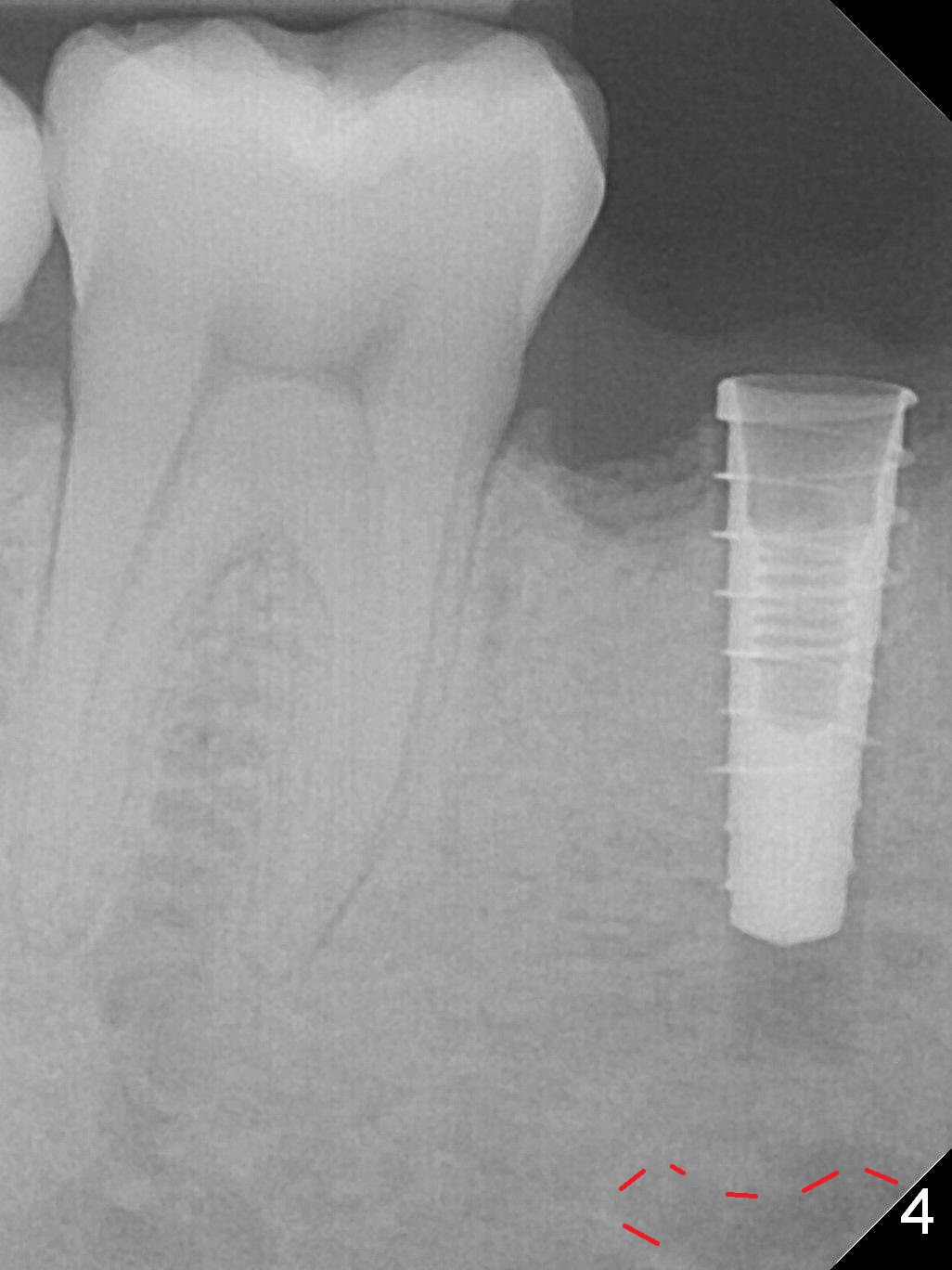
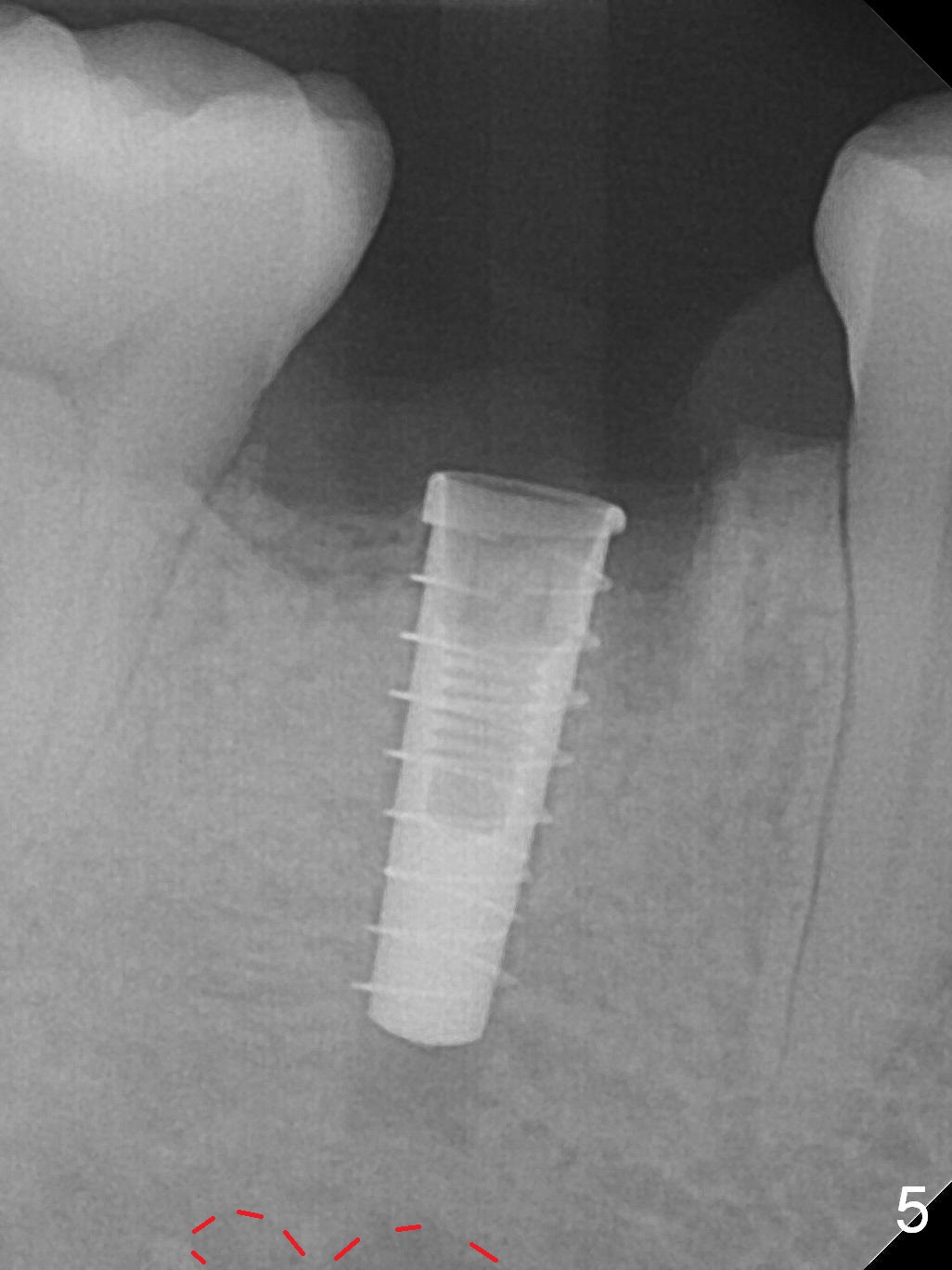
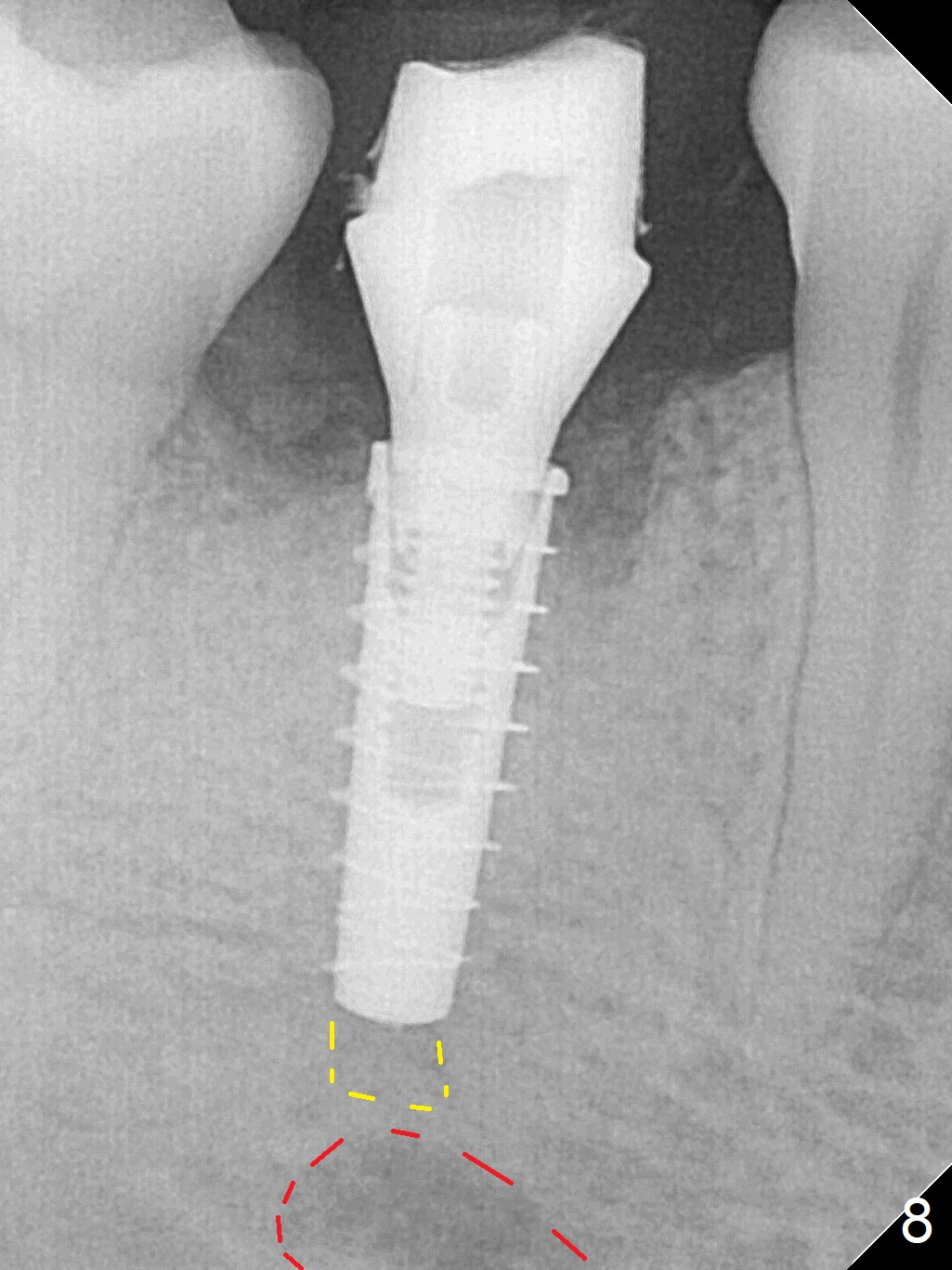
The lower 2nd primary molar has buccal furca lesion (Fig.1 *) with the thin buccal plate (Fig.2). Osteotomy is initiated in the sloped septum (Fig.3). After use of Magic Drill (MD) 3.3 mm for 13 mm and MD 3.8 mm for 11 mm, placement of a 4x11 mm IBS implant meets resistance because of the dense bone (Fig.4-6, red dashed line: Mental Loop) with final insertion torque >50 Ncm. After placement of a 6x4(3) mm abutment and autogenous bone in the remaining shallow sockets (Fig.6), a provisional is fabricated (Fig.7). Finally periodontal dressing is applied. Impression is taken 3 months postop (Fig.8). Buccal infection develops 2 weeks post cementation (Fig.9). When the crown/abutment is removed, there is no residual cement. The implant threads can be felt through the fistula. After soft tissue debridement and copious irrigation, Arestin is placed in the fistula. The latter disappears 15 days post debridement. The patient feels better and moves out of state. It appears that early periimplantitis develops because of the preexisting buccal furca lesion and failure to place the implant deep. The implant will be placed deep after loosening a little (since there is apical space (Fig.8 white line)) or removed, truncated at the apex and placed lower than the buccal crest.
Return to
Lower Premolar Immediate
Implant Course 1
2
Next Deciduous Case
Xin Wei, DDS, PhD, MS 1st edition 03/09/2017, last revision 02/25/2018