|
|
|
|
|
|
|
|
|
|
Avoid Mental Loop
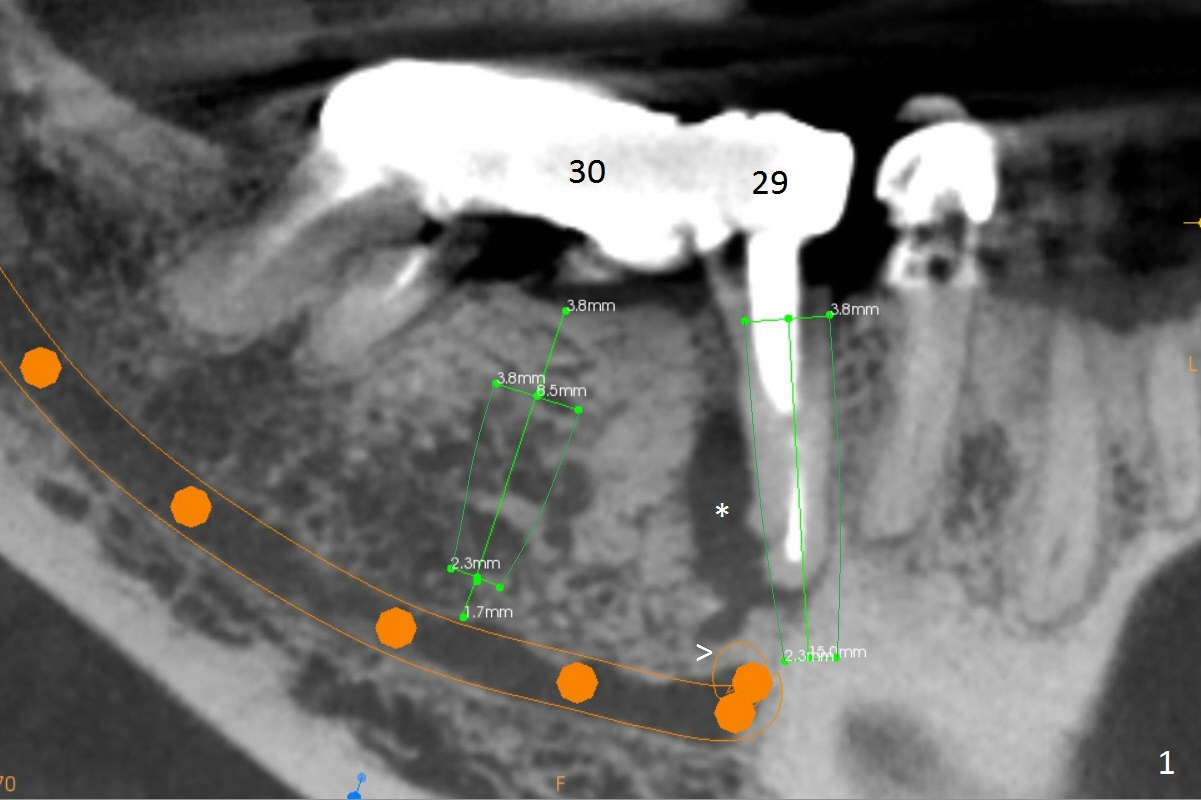
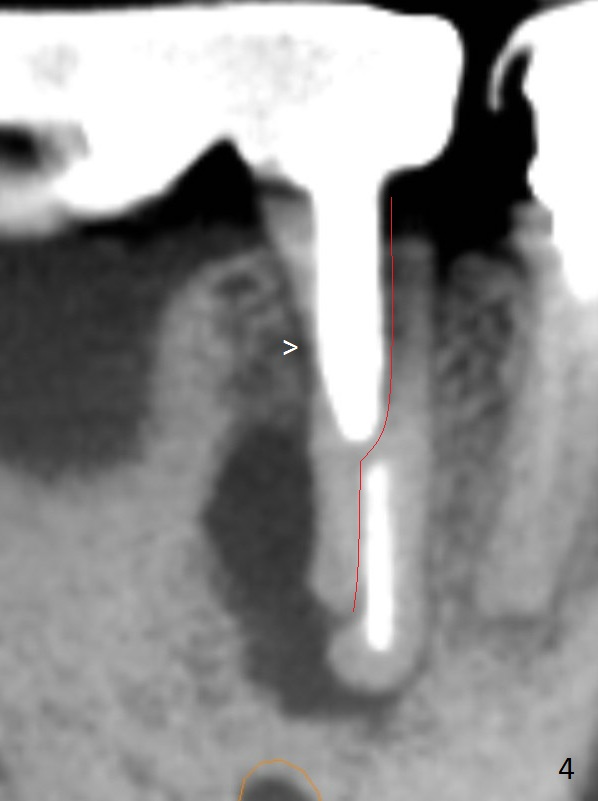
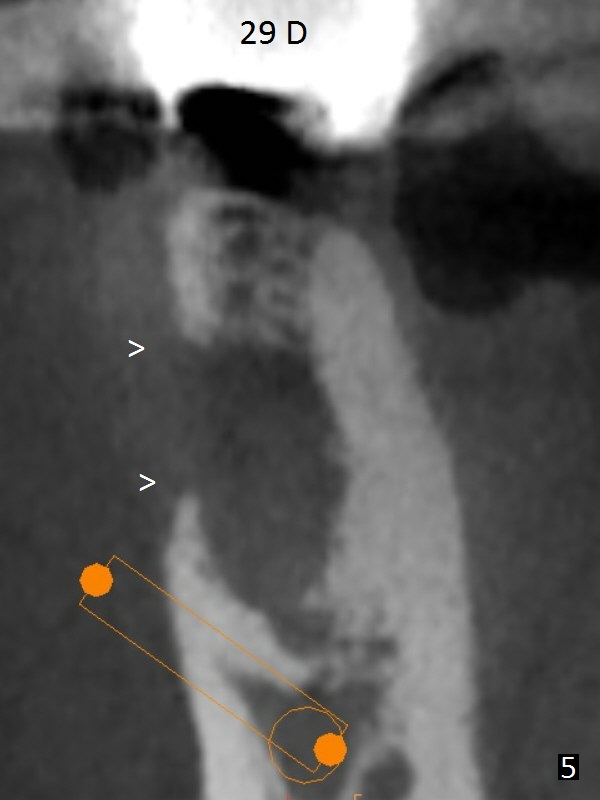
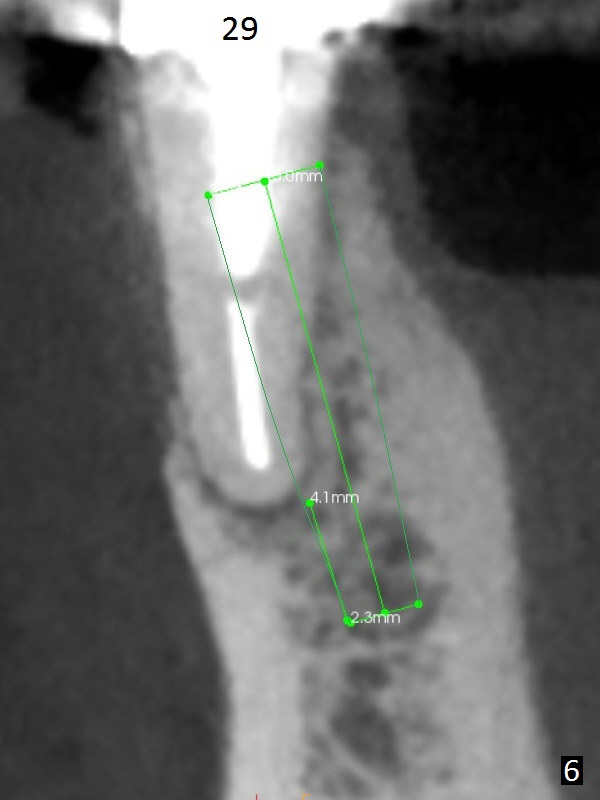
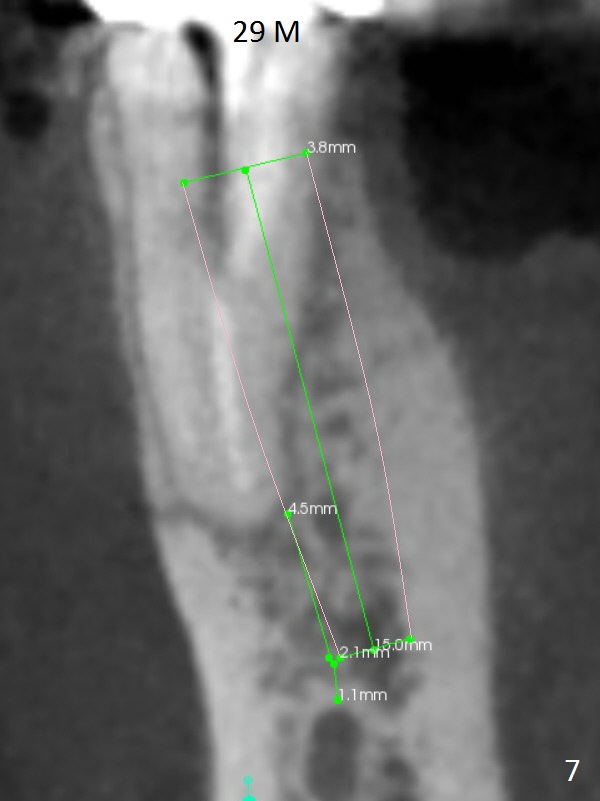
A 50-year-old man has pain and swelling buccal to the tooth #29 with large distal radiolucency (Fig.1 *). The bridge will be sectioned between #30 and 31. The mesial segment of the bridge is expected to separate from #29 post space; the mesial abutment is presumed to have vertical fracture (Fig.4 red line or root perforation due to oversized post (>)). After intraligamental injection, extraction and no Antibiotic treatment, a narrow long implant (Fig.6,7: 3.8x15 or 13 mm) will be placed as mesial and lingual as possible to avoid the buccal bony defect (Fig.5 >; repaired with Osteotape or PRF membrane) and the Mental Loop (Fig.1 >).
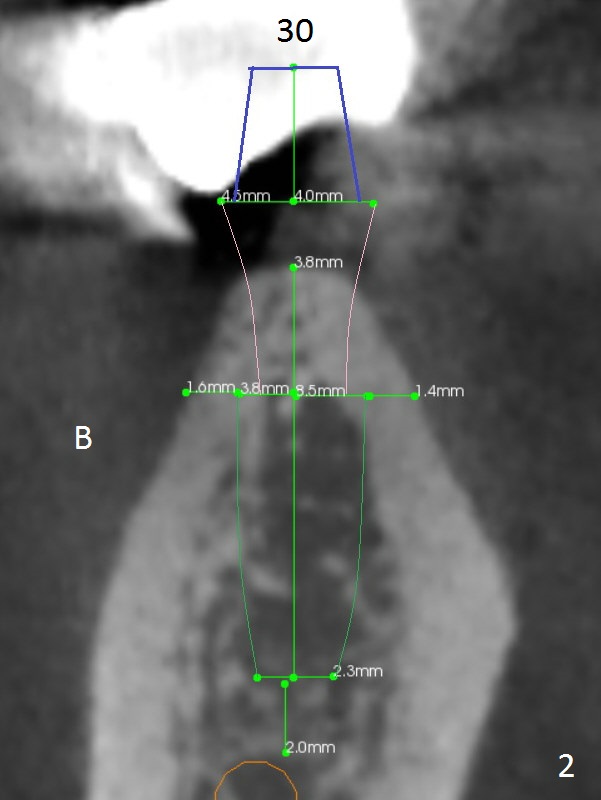
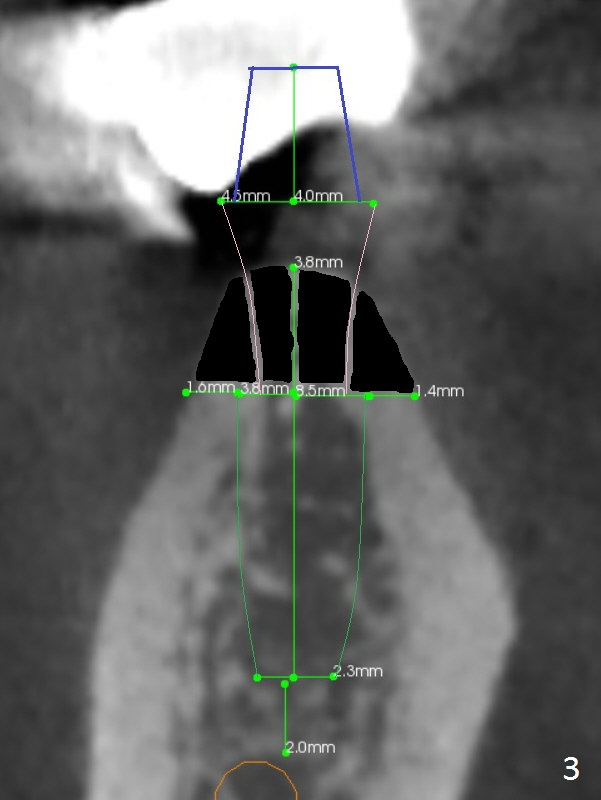
The ridge at #30 is pointed (Fig.2) and going to be resected (Fig.3 black area) to receive a narrow, short implant (3.8x8.5 mm). A splinted immediate provisional will be fabricated following placement of a 4.5x4(5) mm abutment at #30 (Fig.2,3). Take Alginate impression when the patient arrives in case the tooth #31 is also non-salvageable.
Return to
Lower Premolar Immediate
Implant, IBS 下齿槽神经
Xin Wei, DDS, PhD, MS 1st edition 06/03/2017, last revision 08/08/2021