
,%203.8x16.jpg)
,%203.8x16.jpg)
,%20laser%20gingivectomy.jpg)

|
|
|
|
|
|
|
|
|
|
|
|
|
|
Too Close to Mental Loop
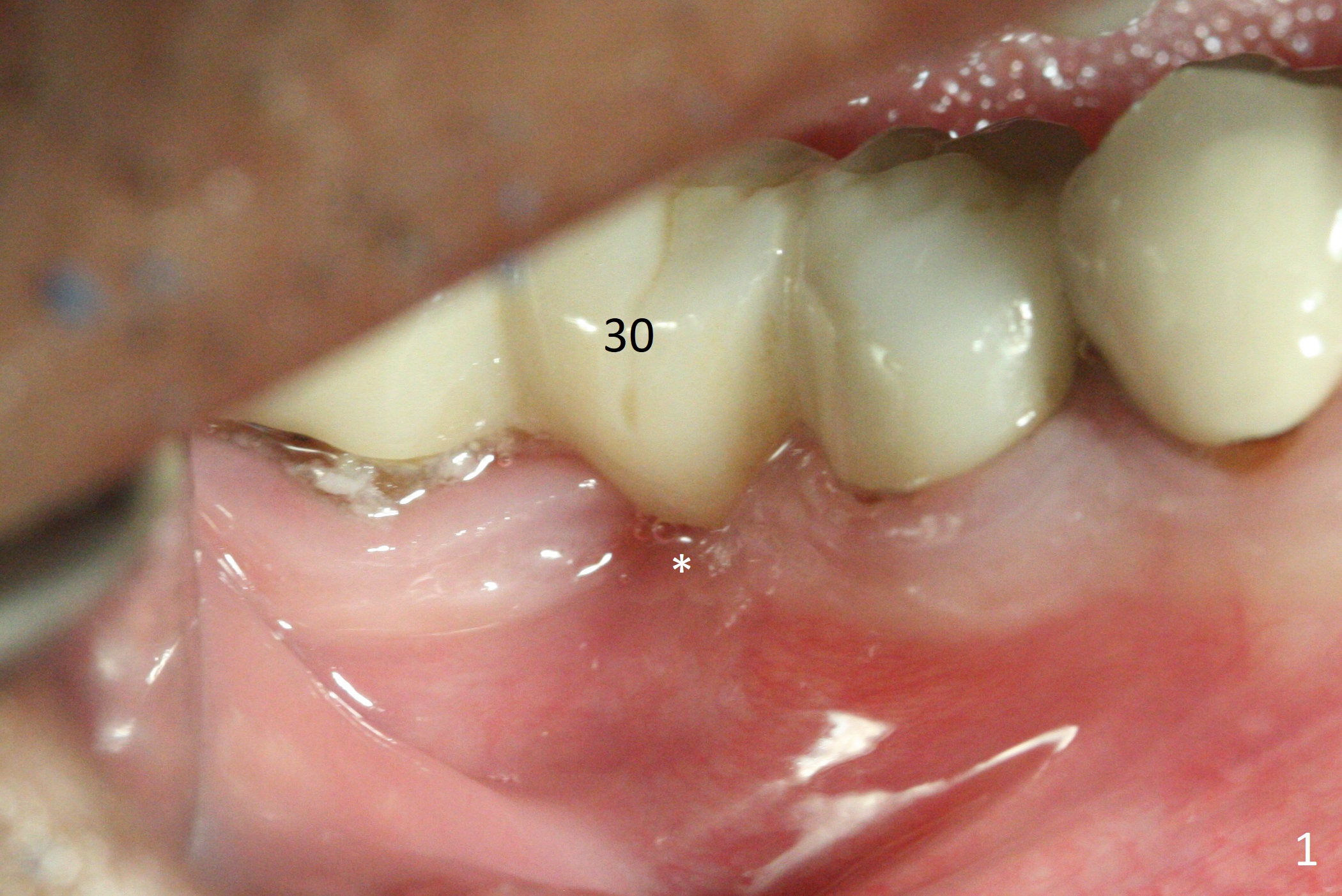
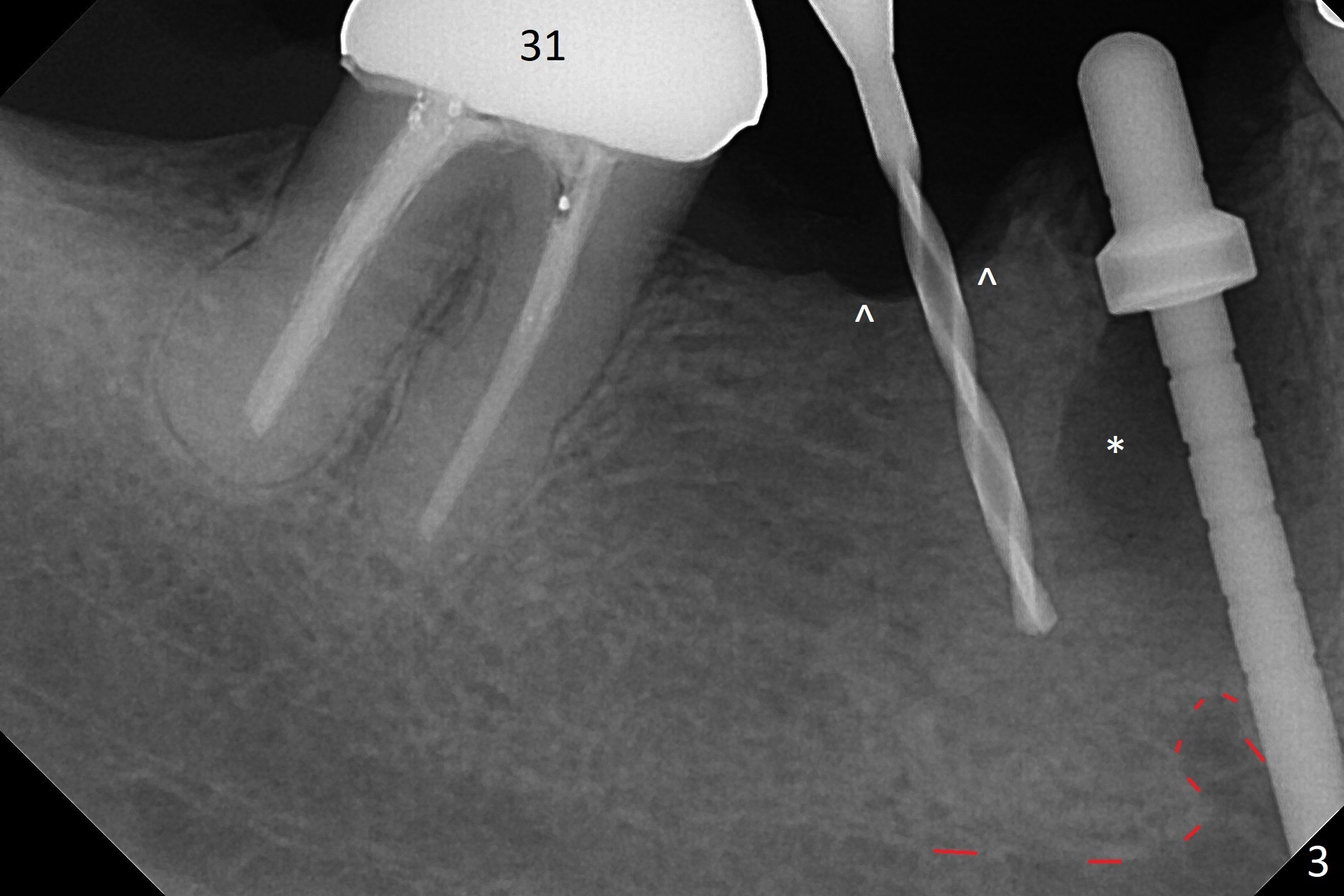
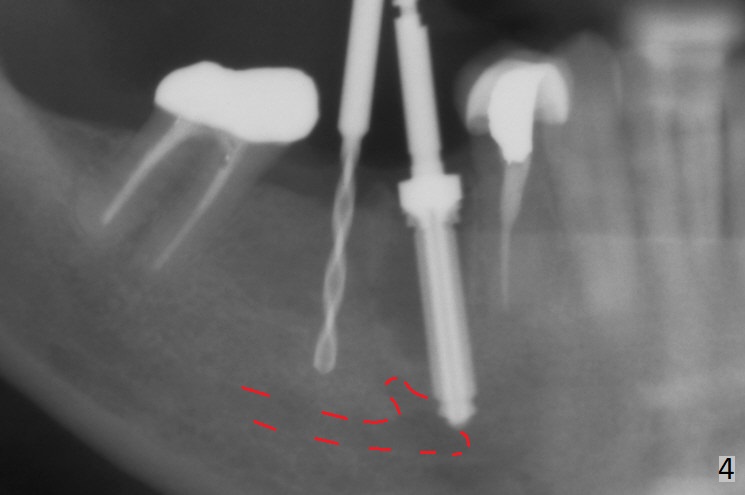
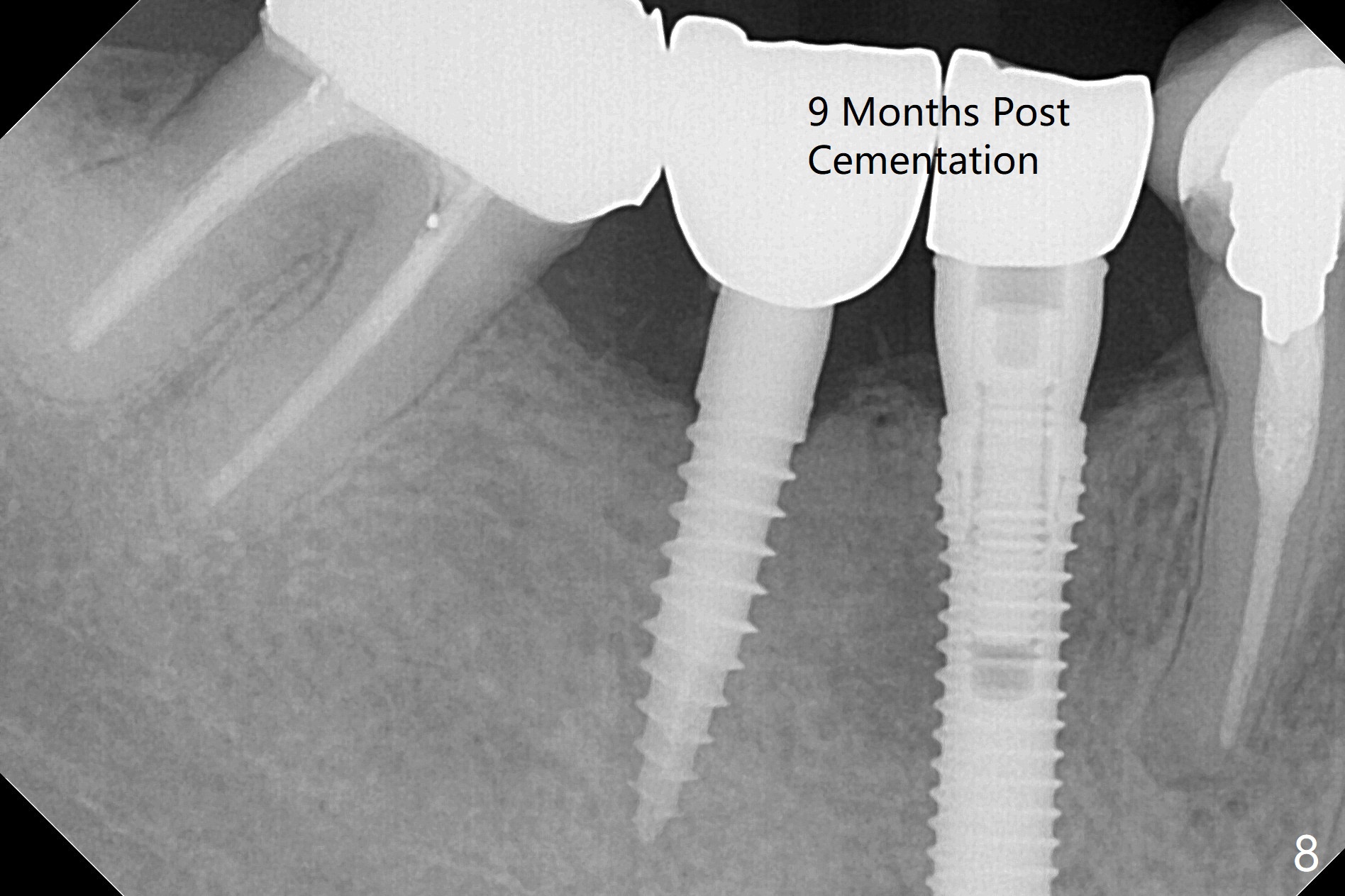
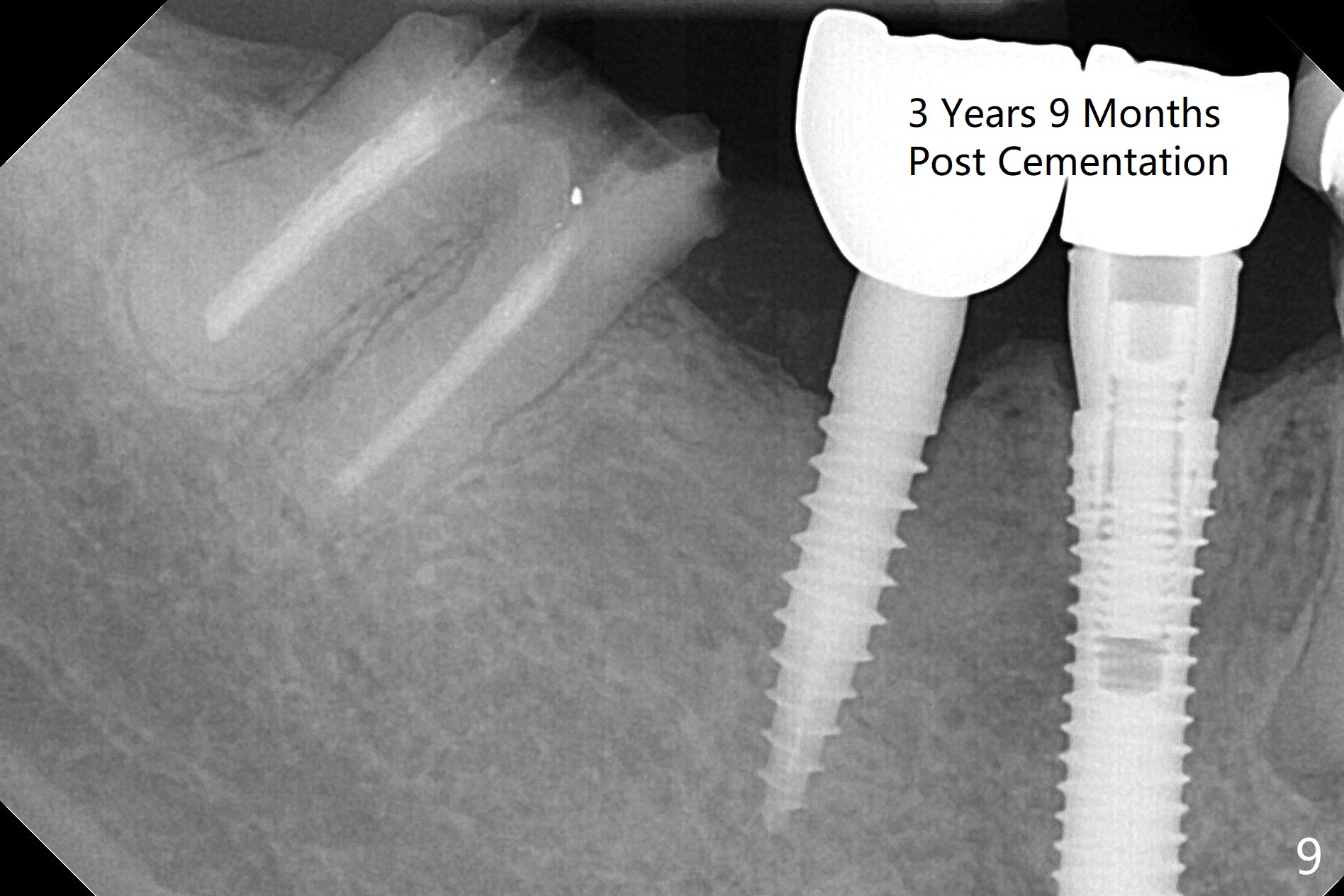
Preop examination shows that the buccal plate at #30 is atrophic (Fig.1 *). The mesiodistal width of the pontic is narrow as compared to the retainer at #31 (Fig.2). It appears that a narrow implant should be placed at #30 and should be able to sustain functional loading. After ridge reduction at #30 (Fig.3 ^) and extraction and debridement at #29, osteotomies at these sites are initiated with 1.2 mm and 2 mm drills, respectively. Probably due to low bone density, the osteotomy at #29 drops deep and close the Mental Loop (red dashed line). While the trajectory at #30 improves, the osteotomy at #29 remains close to the Mental Loop (Fig.4), asymptomatic with infiltration anesthesia. A 3x12(2) mm 1-piece implant is placed at #30 and 3.8x16 mm 2-piece implant at #29 (Fig.5,6 with insertion torque >50 and <50 Ncm, respectively). The large distal defect at #29 (Fig.3,5 *, most likely due to post-related perforation) is later filled with bone graft (data not shown). After placing an abutment at #29 and suturing, periodontal dressing is applied. Three months later, the meisal gap of #29 disappears while the distal one reduces (Fig.7 *). The abutment is changed to 4.5x4(4) mm one before reprep for impression. There is no bone loss 9 months post cementation (Fig.8) or 3 years 9 months post cementation (Fig.9). In fact the crown is lost at #31. At repeated request from the patient, a prefabricated post and crown will be fabricated for short term purpose while an implant is going to be placed at #19. The new crown at #31 has no occlusal contact (Fig.10), which may change over time.
Return to
Lower Premolar Immediate
Implant,
IBS
下齿槽神经
Xin Wei, DDS, PhD, MS 1st edition 06/19/2017, last revision 08/10/2021