|
|
|
|
|
|
|
|
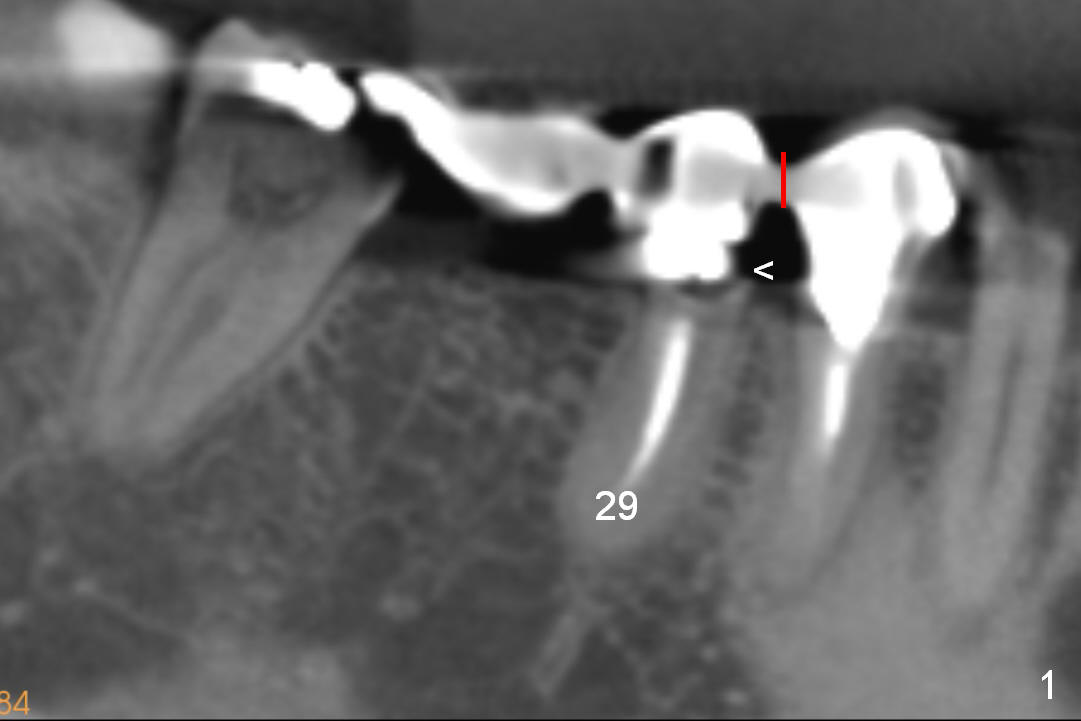
From Bridge to Implants: Immediate Restoration
A 52-year-old lady complains of food impaction underneath #29 retainer (Fig.1). The retainer is most likely separated/fractured from its abutment (<). A section is to be made between #28 and 29 retainers (red line).
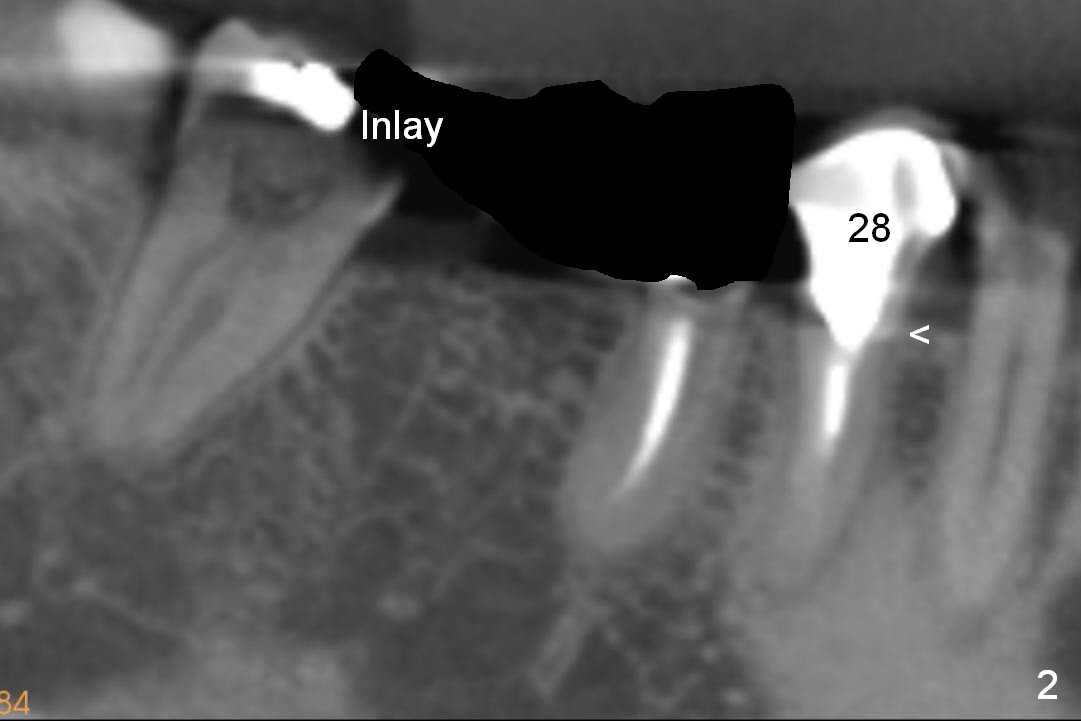
The posterior 3-unit should be able to dislodge (Fig.2). Check whether there is the similar lesion associated with #28 (<). The tooth #31 should be afforded not to be restored, since there is a small inlay prep mesially.
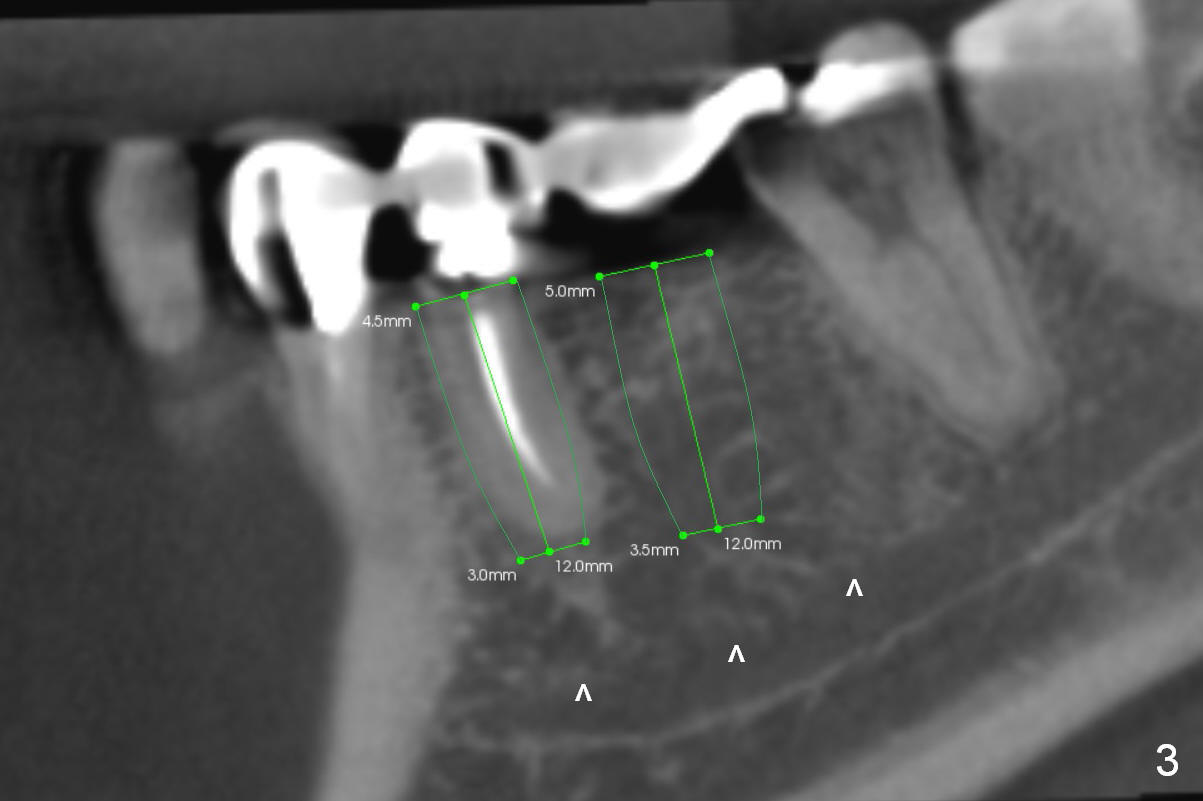
If it is the case, two implants will be placed at the sites of #29 and 30 (4.5x12 and 5x12 mm, respectively, Fig.3).
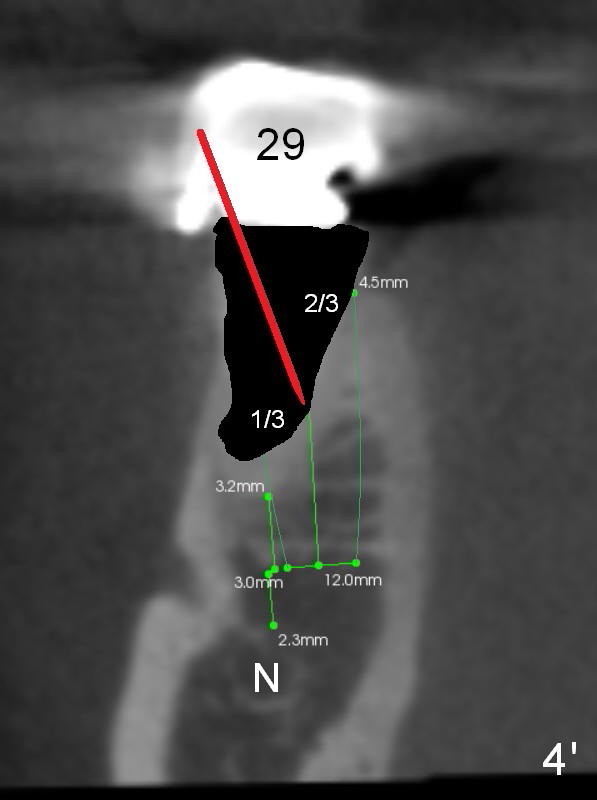
After #29 root extraction, osteotomy starts in the lower 1/3 of the lingual socket wall (Fig.4' red arrow). Once the pilot drill enters the lamina dura, the trajectory will change to the axis of the tooth (Fig.4).
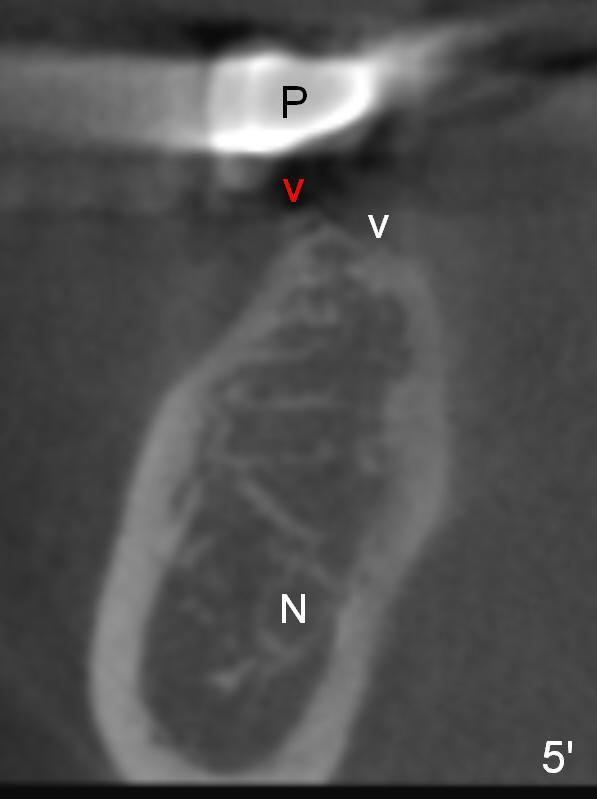
As to #30 osteotomy entry point, it tends to start in the middle of a flat surface (Fig.5' white arrowhead), but it is directly underneath the pontic (P). The trajectory will be not correct. Ideally the entrance point should be at the crest. To avoid slippage, a sharp starter drill will be used. A second advantage is that the osteotomy will be as deep as the previous entry point. There is less likelihood of nerve (N) injury (Fig.5).
Immediate provisionals will be splinted if insertion torque is high for each implant (use latch adapt).
Return to Lower Bicuspid
Immediate Implant,
Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 03/15/2015, last revision 03/15/2015