

,%20bone%20graft.jpg)

|
|
|
|
|
|
|
|
|
|
|
|
|
||
Where is Implant Placed?
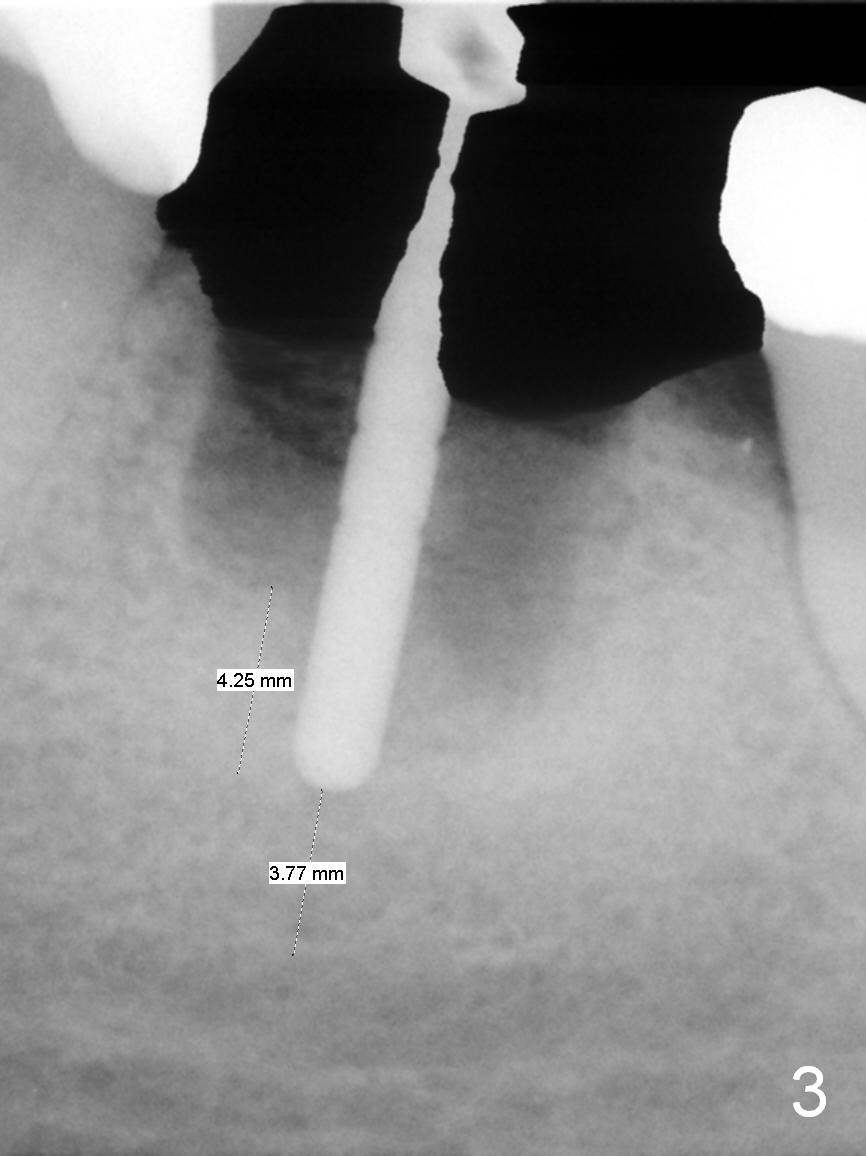
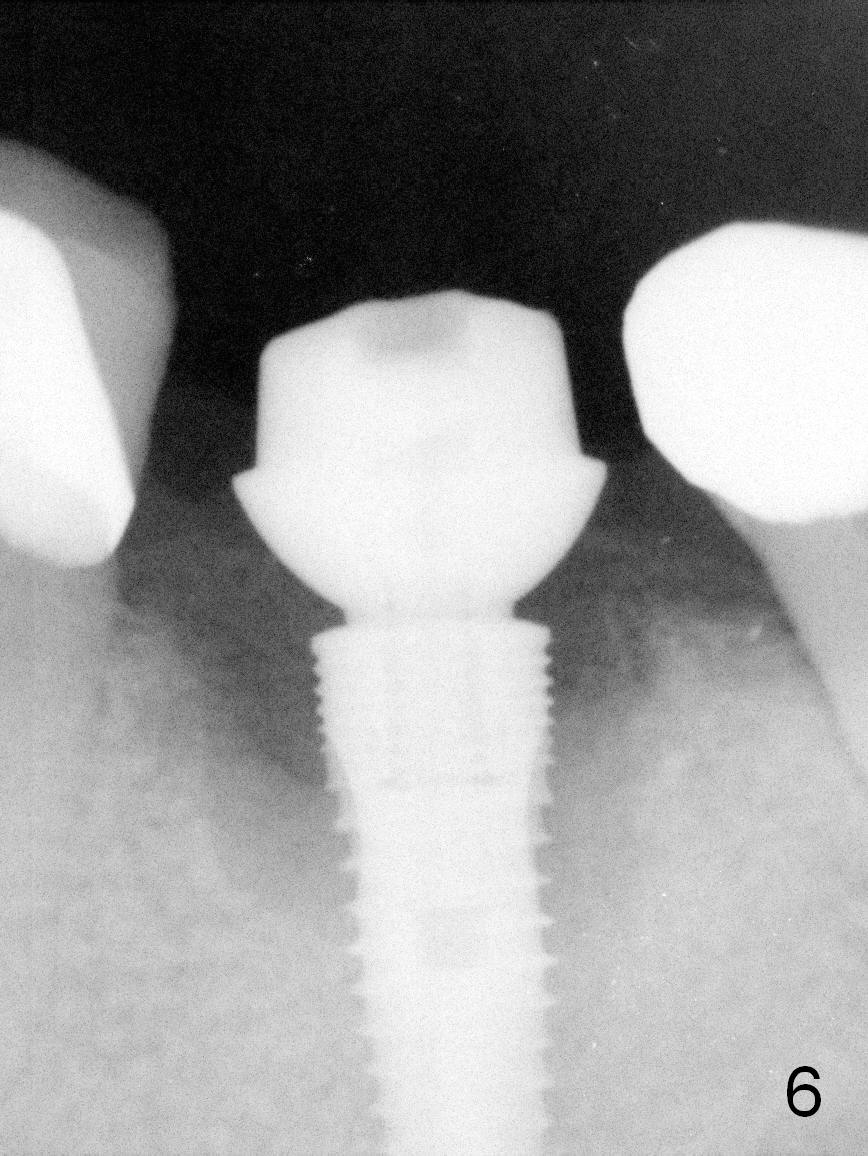
A 56-year-old lady (YW) has diabetes II, fairly well controlled. Although there is radiologic evidence of mesial root fracture of the tooth #19 (Fig.1 (panoramus)), she is asymptomatic. The buccal gingiva is slightly erythematous and edematous. There is no deep pocket. According to Fig.1, either the buccal or lingual wall is lost. This is not evident from Fig.2 (PA). Osteotomy is established in the septum or the distal socket (treated with Clindamycin), away from the lost plate (Fig.6,7). It is estimated that there is 4-5 mm apical bone. Measure the depth of the socket. Osteotomy should be 3 mm beyond the socket.
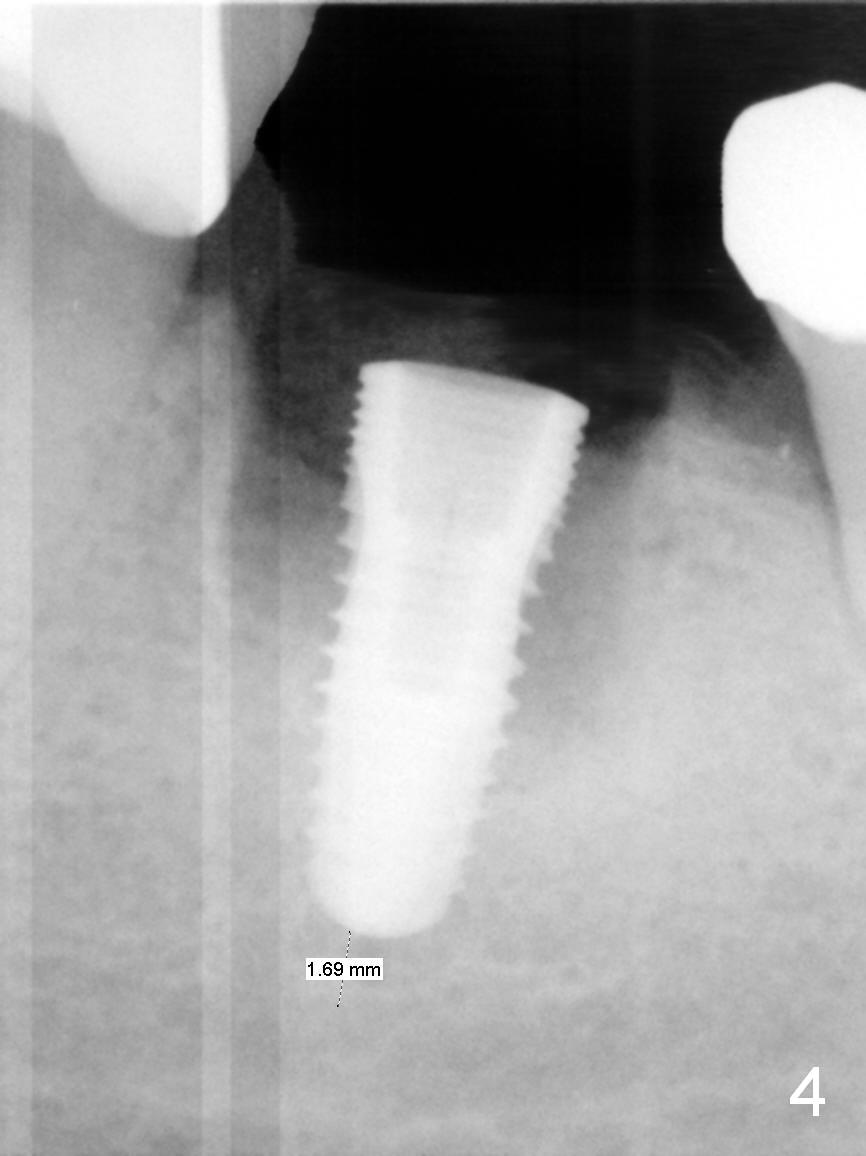
In fact, the buccal plate and the septum are defective. Osteotomy is initiated lingual to the center of the common sockets (Fig.1); depth is about 4 mm. When a 5x12 mm bone-level implant is placed (Fig.4), there is a gap mesiobuccally, which is later filled with bone graft (Fig.5 *). A large abutment (7.8x4(3) mm) is placed immediately (Fig.5 A) for an immediate provisional to close the sockets. The buccal abutment margin is ~ 1 mm subgingival, whereas the lingual ~2 mm supragingival. The abutment may need to be changed in the restorative phase (Fig.9,10).
As expected, the lingual margin of the abutment is supragingival 2 months postop. The immediate provisional is fractured (Fig.6). The abutment is changed to 5.8x4(2) mm and impression is taken.
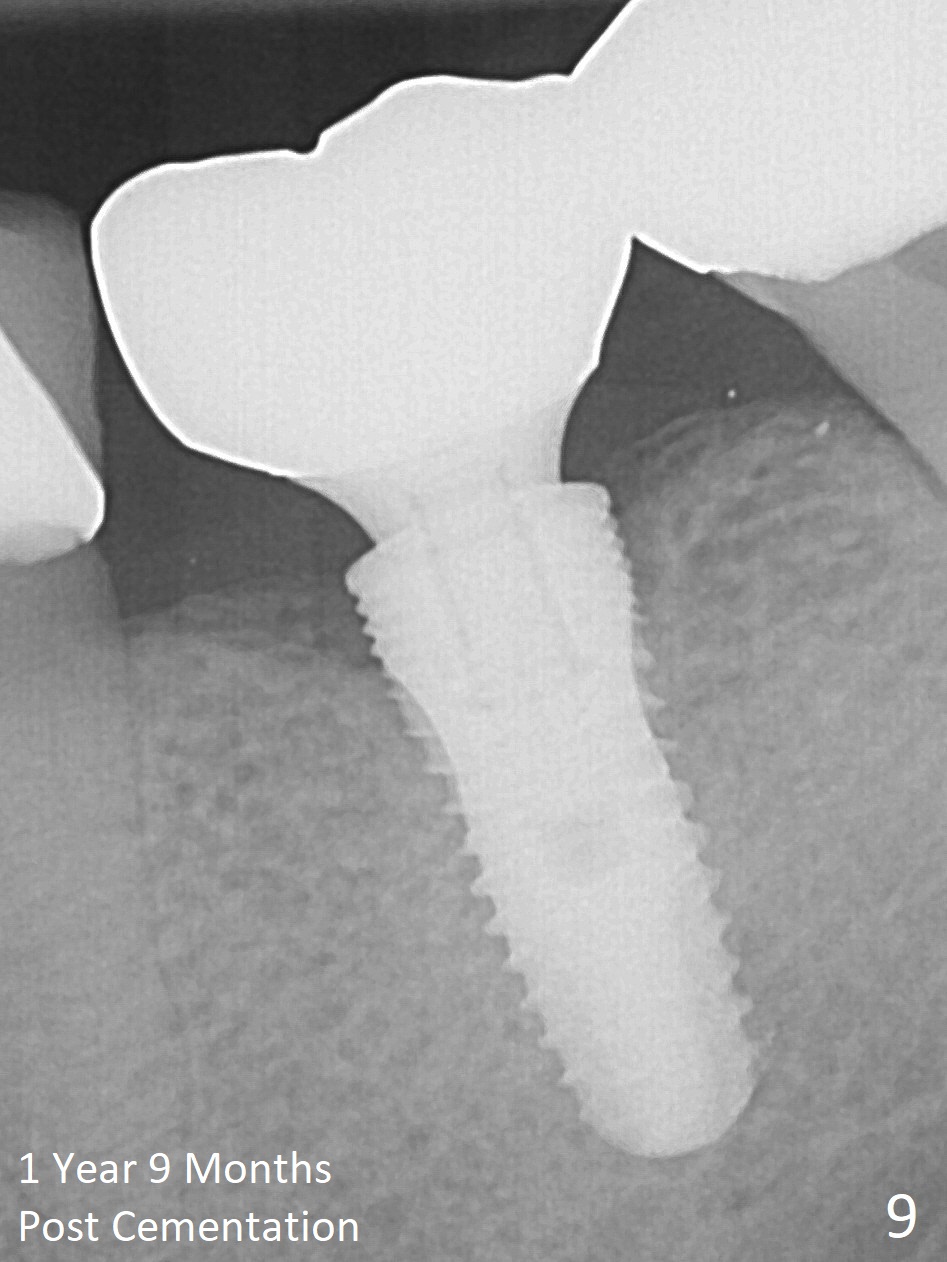
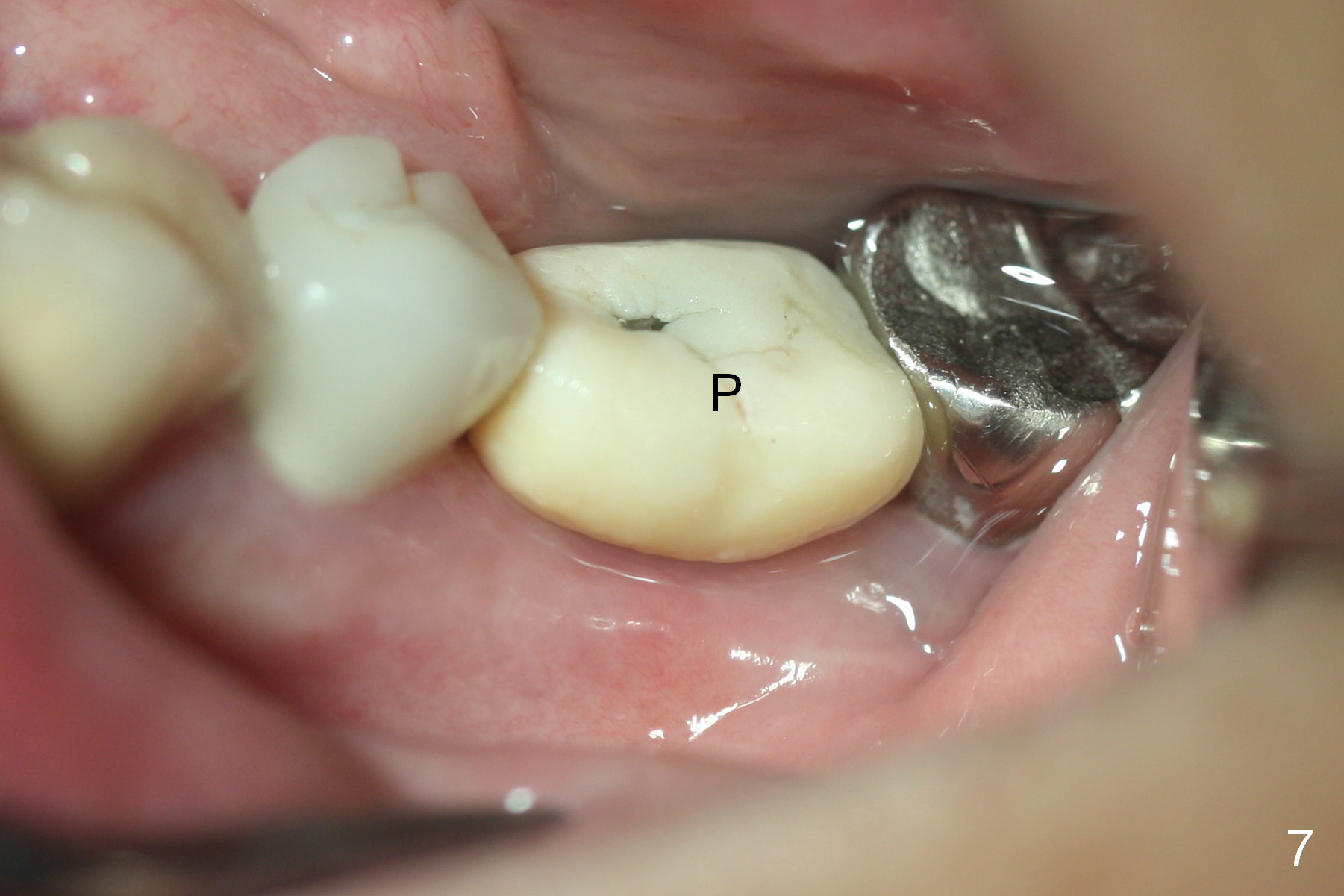
Two months post impression (4 months postop), the patient returns for cementation. The provisional is perforated again in the occlusal surface (Fig.7 P). When the provisional is removed, a shallow trough forms around the abutment (Fig.8*). The bony defect appears to be repaired 1 year 9 months post cementation (Fig.9).
Return to Lower Molar Immediate Implant,
Systemic Diseases
Xin Wei, DDS, PhD, MS 1st edition 11/06/2015, last revision 12/14/2017