

|
|
|
|
|
|
|
|
Long Immediate Implant: Beware
A 48-year-old lady has poor dentition. Four years and a half ago when the tooth #21 needed root canal therapy (RCT), the tooth #19 showed bone loss (Fig.1 arrowheads) and hidden caries (white *). The carious lesion caused severe toothache 2 years later (Fig.2 *), while the perio lesion remain severe. The tooth #19 received RCT; the patient remained asymptomatic until recently. Since the patient is satisfied with immediate implant with the tooth #2 (mainly perio lesion), she is not hesitant in accepting the same mode of treatment for #19.
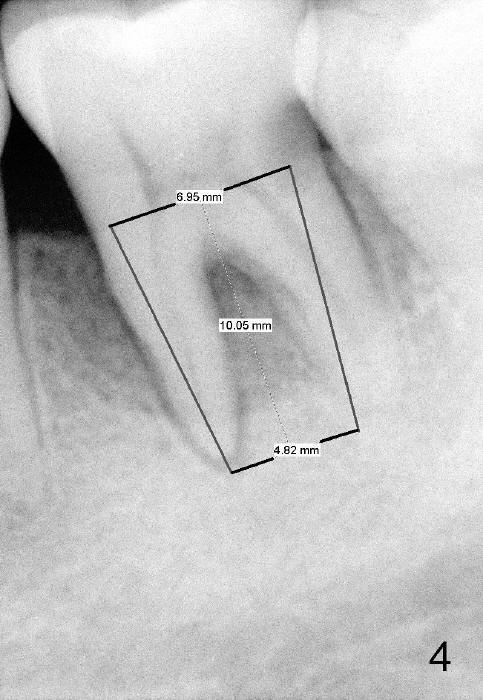
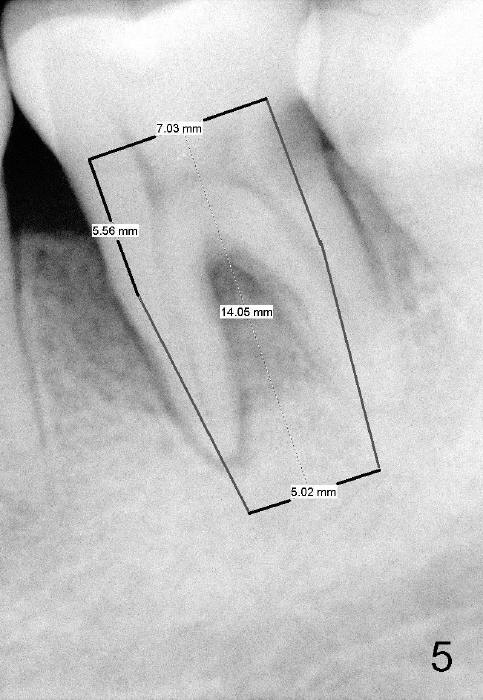
Considering severe bone resorption, a 6.9x10 mm bone-level (Fig.4) or 7x14 mm gingiva-level (Fig.5) implant does not seem to be long enough to achieve primary stability. Probably a 7x17 mm gingiva-level implant is more appropriate, but it carries more risk of nerve injury. Be careful. Take several intraop PAs for depth confirmation. Try shorter osteotomy and implant first and use longer one if necessary.
Use Lindamann bur to make a slot on the septum before osteotomy. The slot should be slightly more lingual to prevent buccal thread showing through. The implant to be placed should be large enough to obtain primary stability, but not too large. Too large an implant tends to make the buccal bone thin or perforated.
Immediate provisional is highly necessary, due to a previous history of shifting of a neighboring tooth. Anyway, is the buccal plate defective?
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 01/18/2015, last revision 02/19/2015