

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
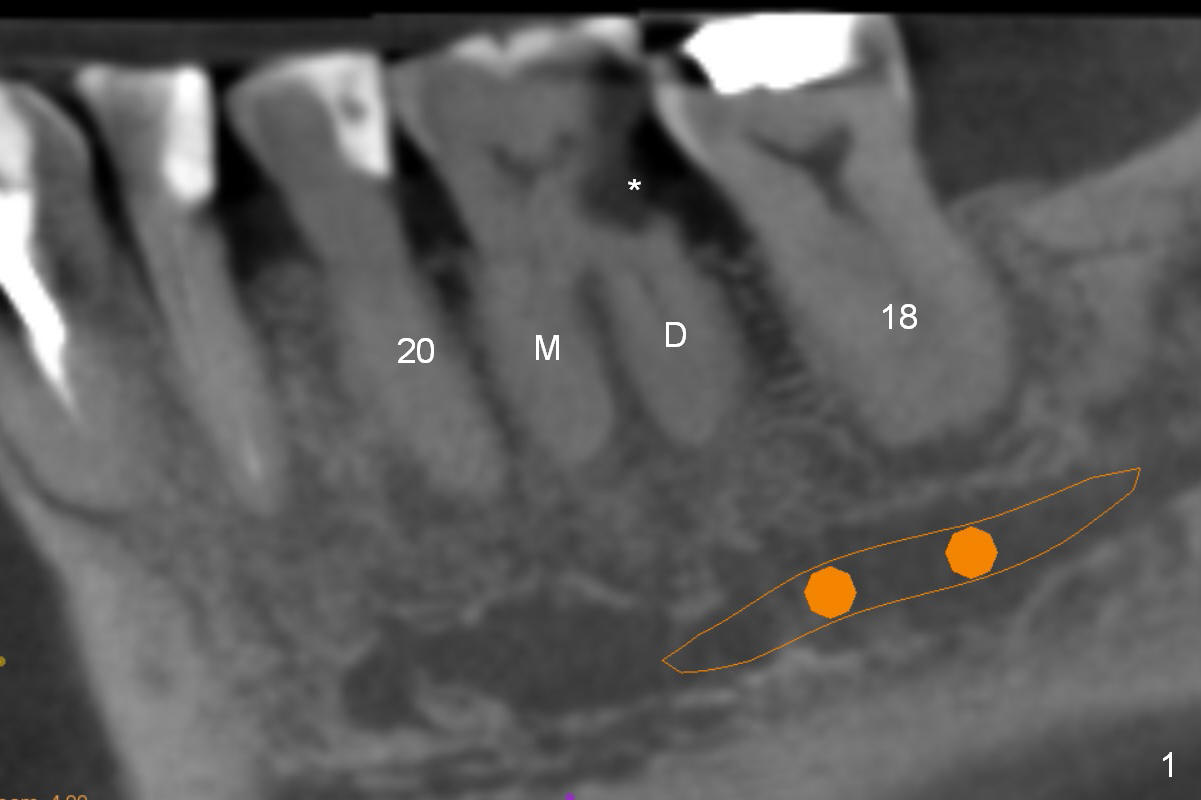
When Thick Roots of Lower 1st Molar are Deviated Mesial
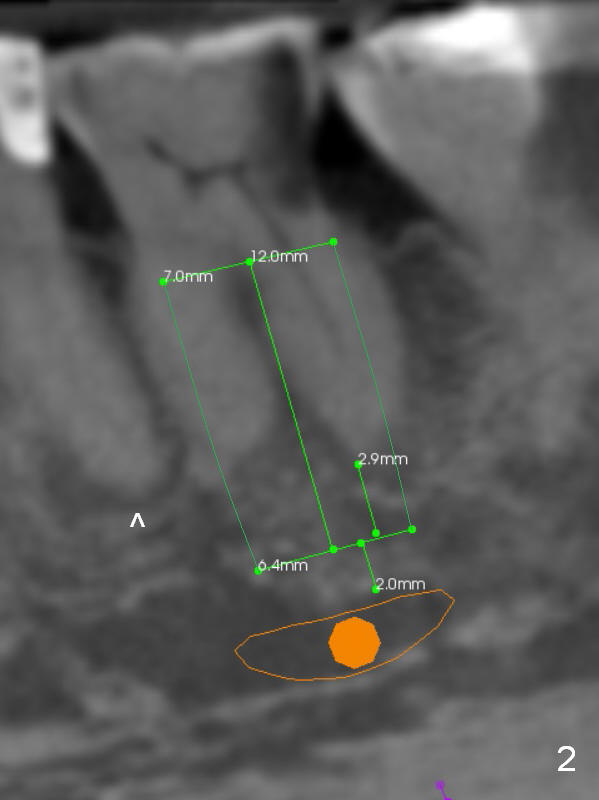
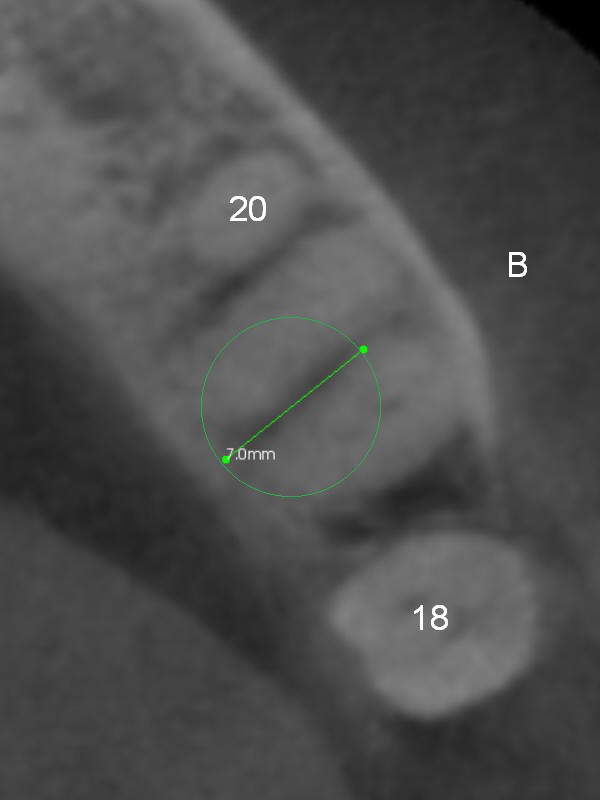
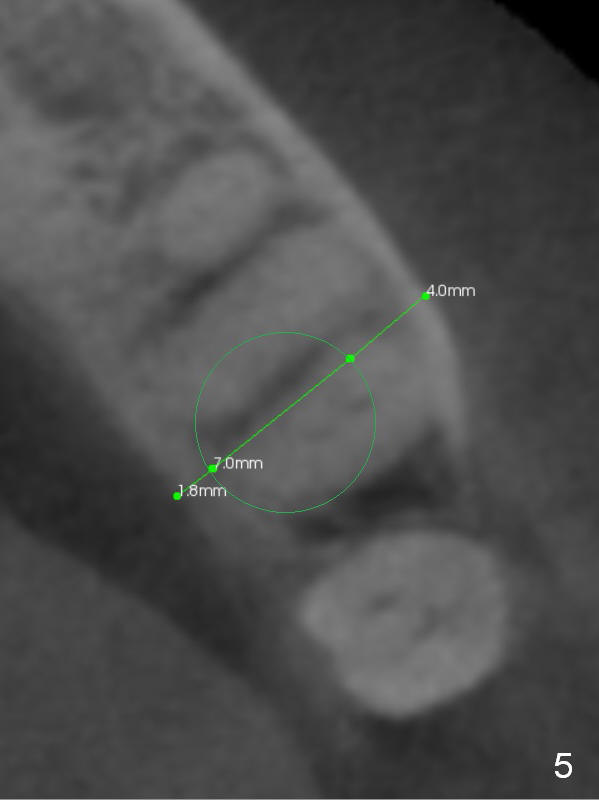
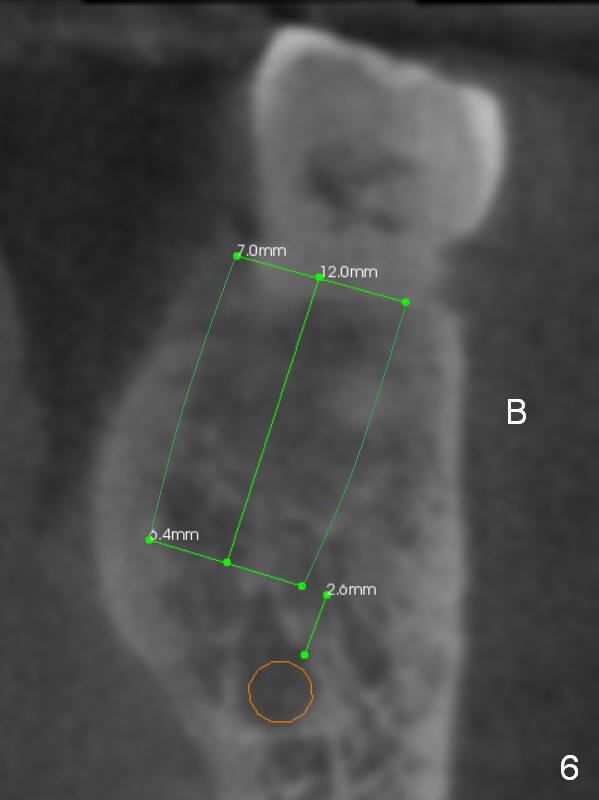
A 71-year-old man (CK) has pain in mastication when the upper left implant treatment is finished. The tooth #19 with distal caries (Fig.1 (CT sagittal section) *) seems to be non-salvageable. The mesial (M) and distal (D) roots appear to be large and closer to the root of the tooth #20 than that of #18. A large implant (7x12 mm) placed in the middle of the socket may increase the chance to invade the root of #20 (Fig.2, 4 (axial section)), as compared to that placed more distal (Fig.3,5).
The shorter implant (10 mm (Fig.7 (coronal section)). as compared to 12 mm (Fig.6) more or less placed in the middle of the septum may decrease the chance to penetrate the coronal extension (Fig.8 brown triangle) of the Inferior Alveolar Canal (brown circle).
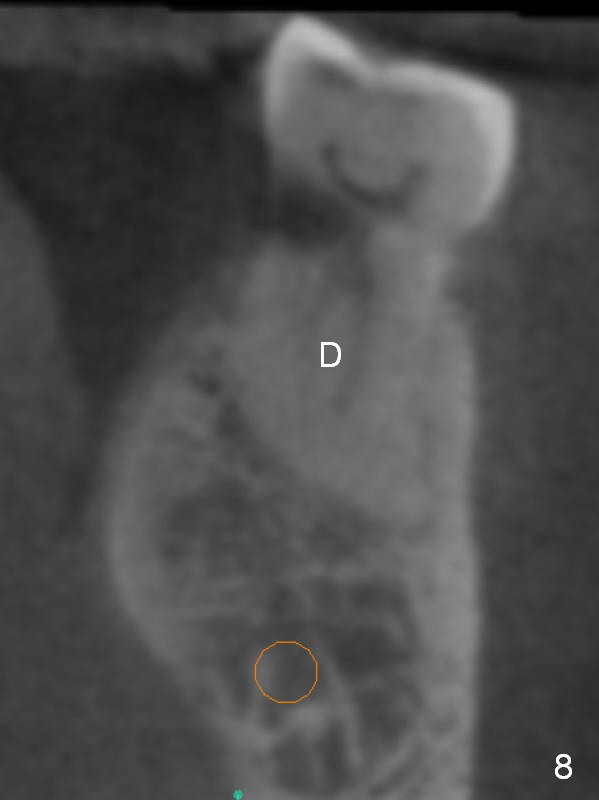
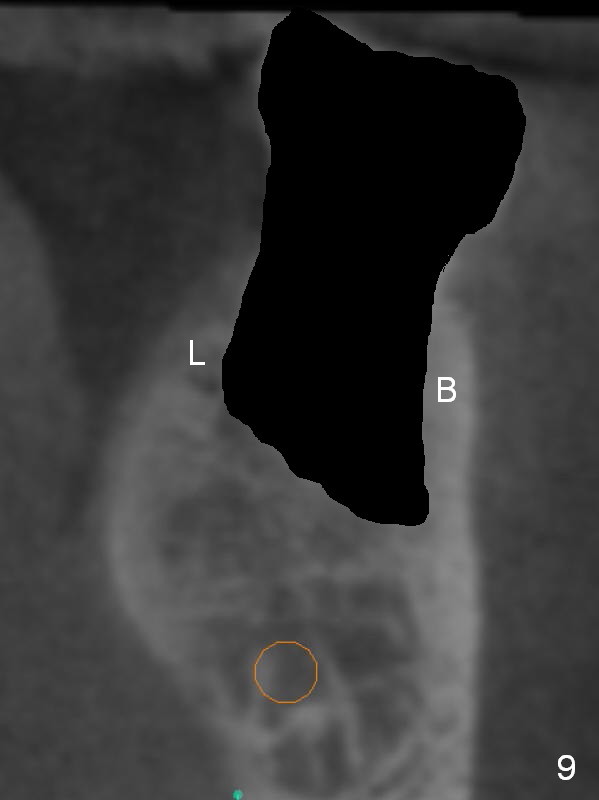
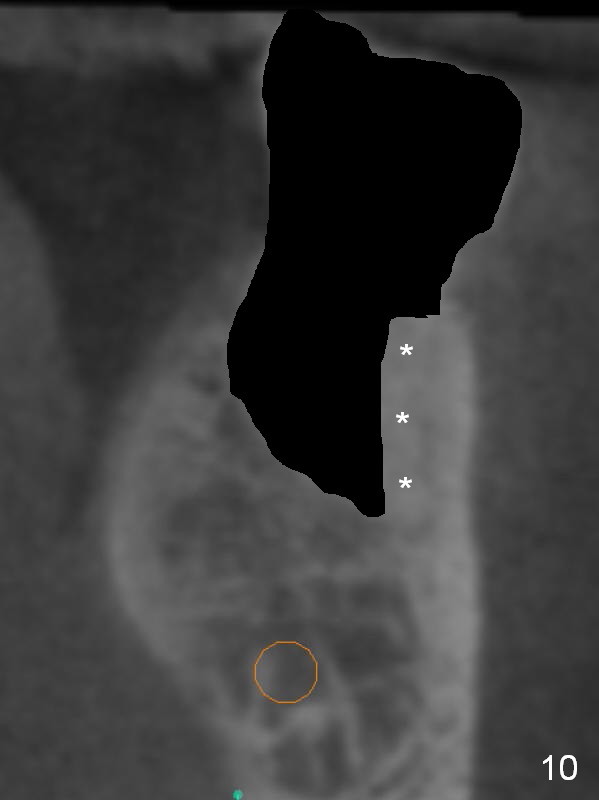
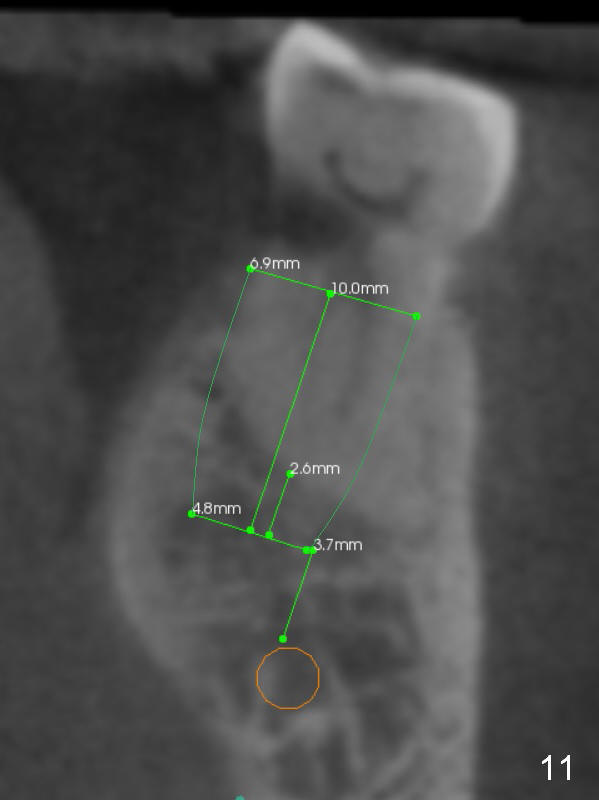
Coronal section through the distal root (Fig.8 D) shows that the lingual plate (Fig.9 (post extraction (Metronidazole)) L) looks thicker than the buccal one (B). When socket shield is performed in the distal root (Fig.10 *, surgical bur block with long surgical fissure bur), there will be less chance to place pressure on the thin buccal plate. The 6.9x10 mm implant may be oversized (Fig.11). Prepare DIO Sinus Master Kit so that 3-4 mm stoppers can be used for osteotomy.
Return to
Lower
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table),
IBS
Xin Wei, DDS, PhD, MS 1st edition 12/02/2016, last revision 12/04/2016