


|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Maxillary Buccal Plate Fracture Due to Bone Expansion
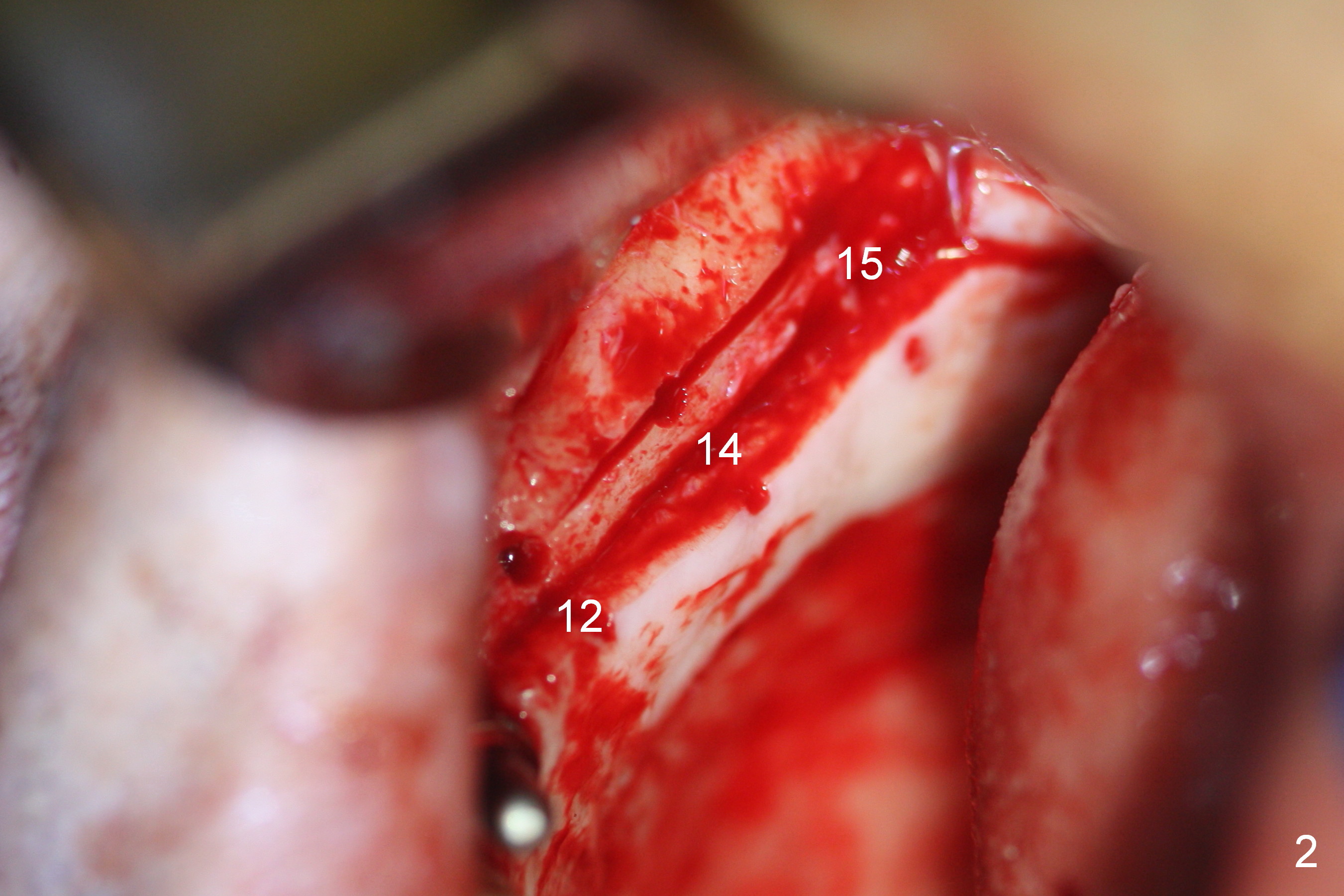
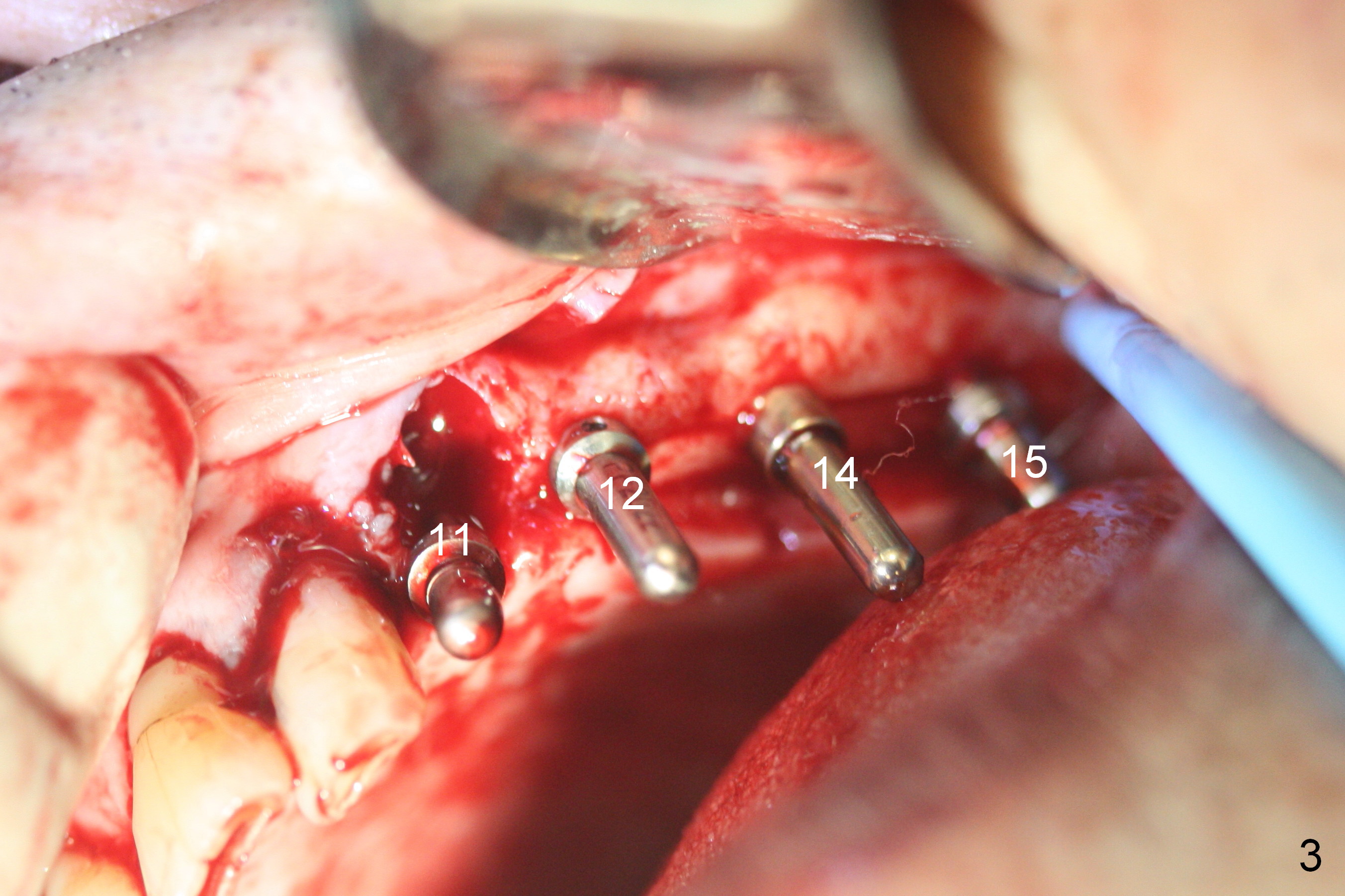
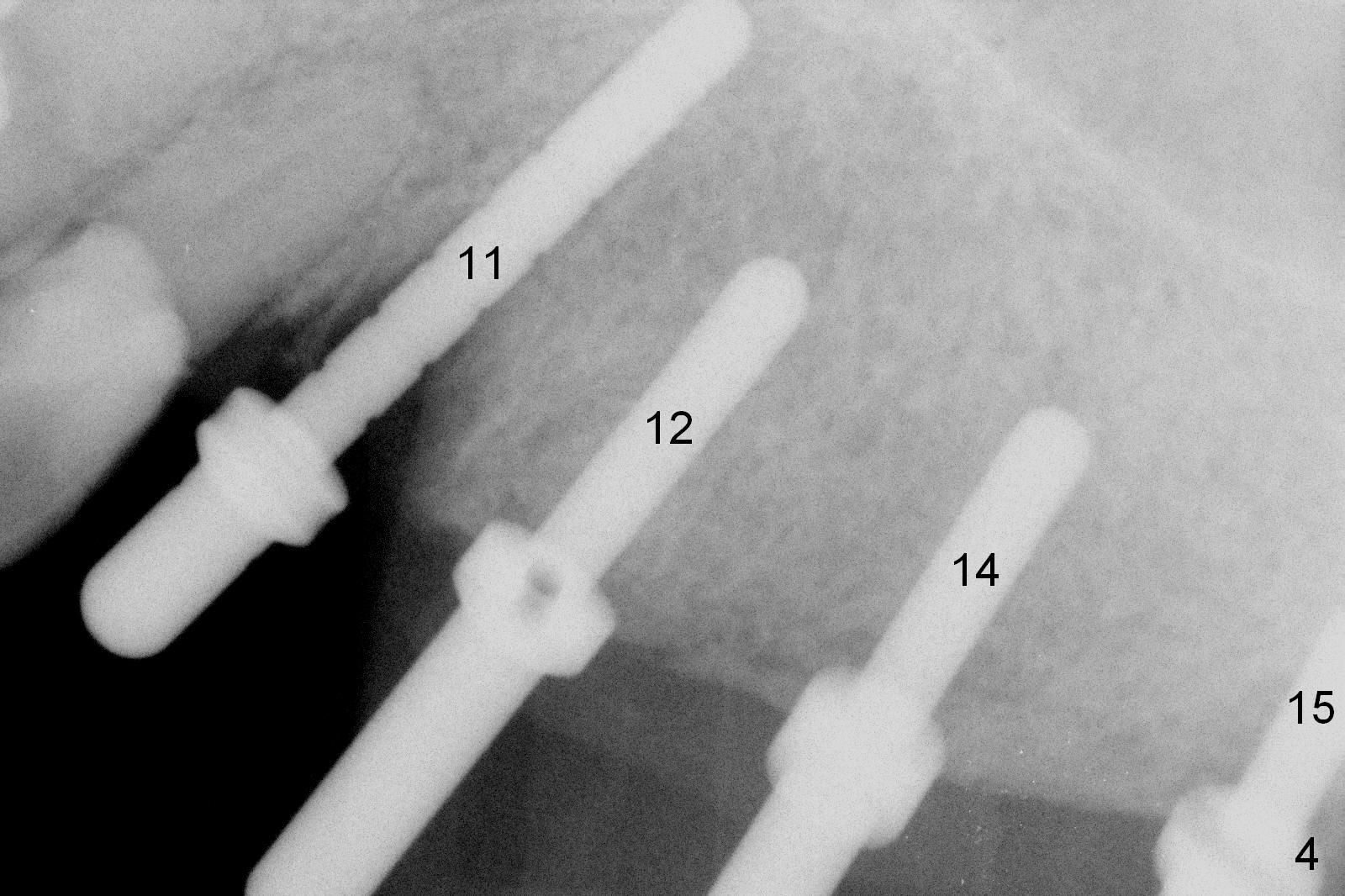
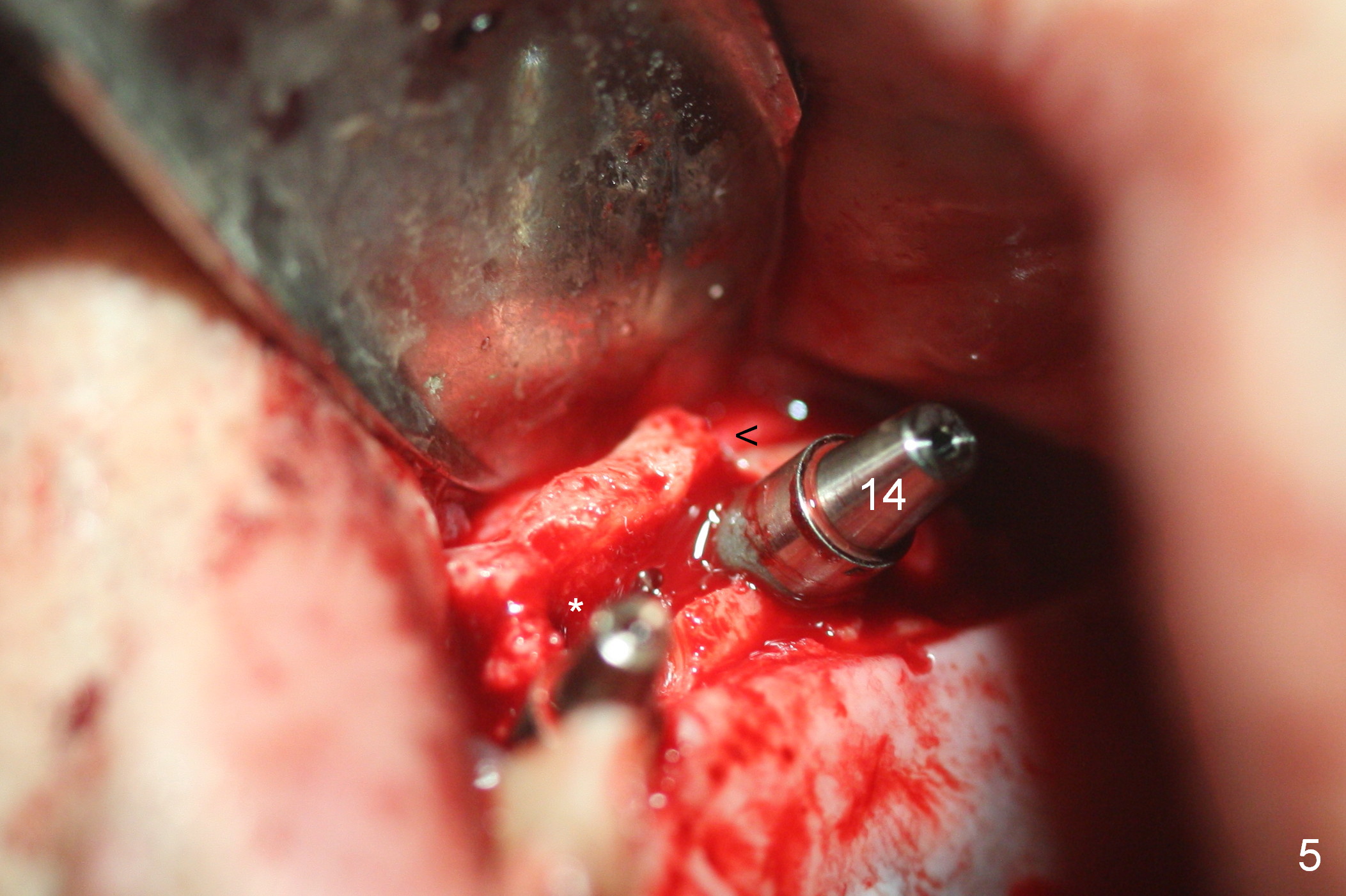
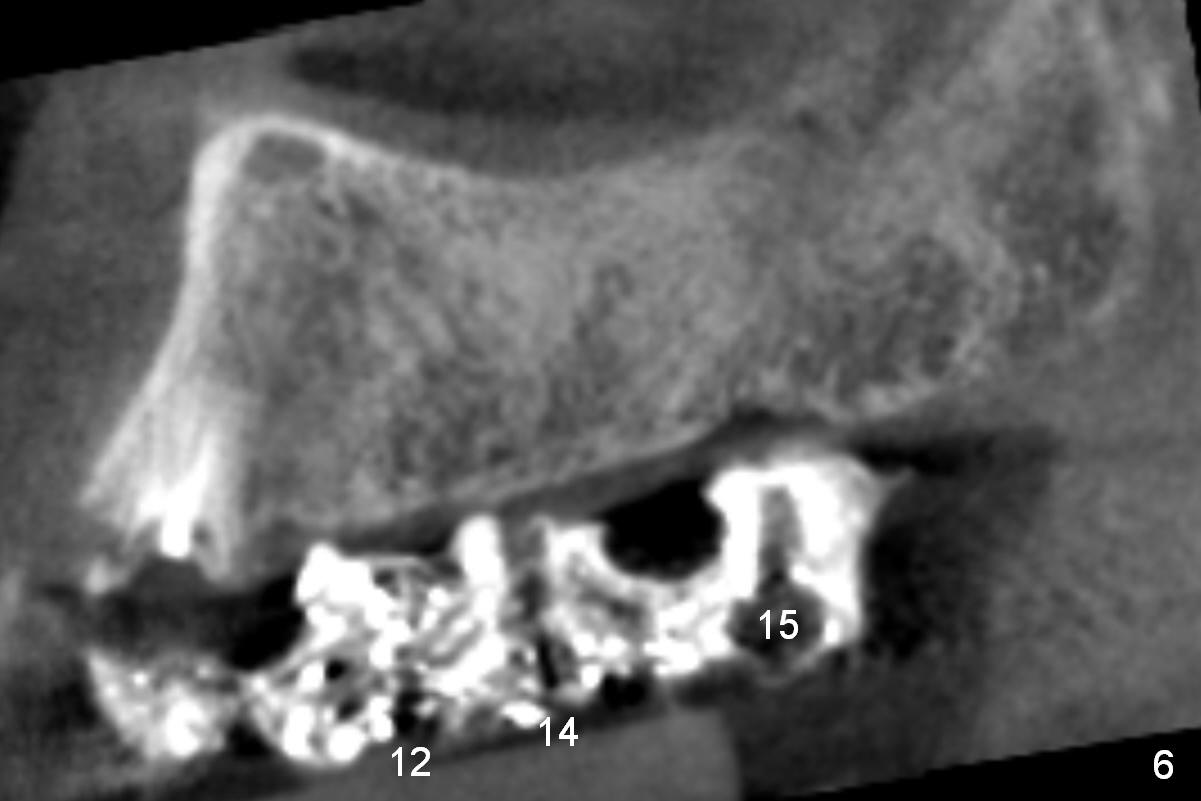
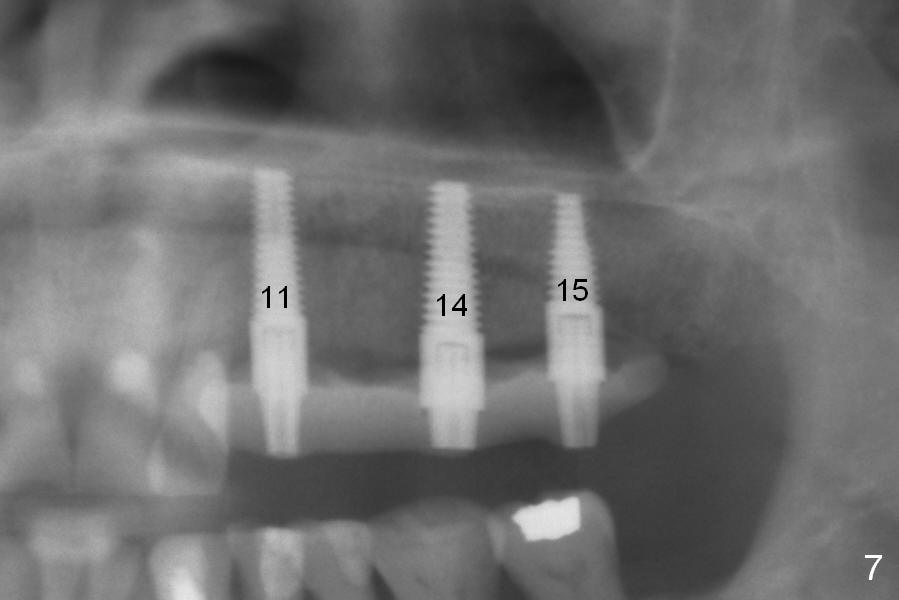
The edentulous ridge distal to #11 residual root is moderately atrophic (Fig.1). The ridge is split with 10 and 13 mm saws between initial osteotomies at #12,14 and 15 (Fig.2). Parallel pins are inserted for trajectory confirmation (Fig.3,4). The gap of the split ridge between #12 and 14 increases when bone expanders (2.7/3.6 mm) are being inserted. A 4.5x17 mm implant does not obtain primary stability at #12. When a 5x17 mm implant is being placed at #12, the buccal plate starts to crack. When the same implant is placed at #14, the crack appears to get larger. Drills are used to finish osteotomy at #14 with force being applied palatally. When the implant is re-inserted, the buccal plate fractures does not appears to get worse (Fig.5 <). In contrast, there is no obvious increase in the gap between #14 and 15 when bone expanders are being used at #15. To avoid complication, drills are used to finish osteotomy before placing a 4.5x14 mm at #15 (Fig.7 (#11: 4.5x17 mm)). CBCT shows that the bone density at #12 and 14 (400-500 Hounsfield units (HU)) is higher than that at #15 (200-300 HU). Ridge split is successful when HU is <200 with smaller diameter implants.
Postop pain is decreasing for 1 month (Fig.8). The ridge is particularly wide. The patient has no interest in getting an implant between those at #11 and 14. After preparation, a splinted provisional is fabricated between #11 and 15.
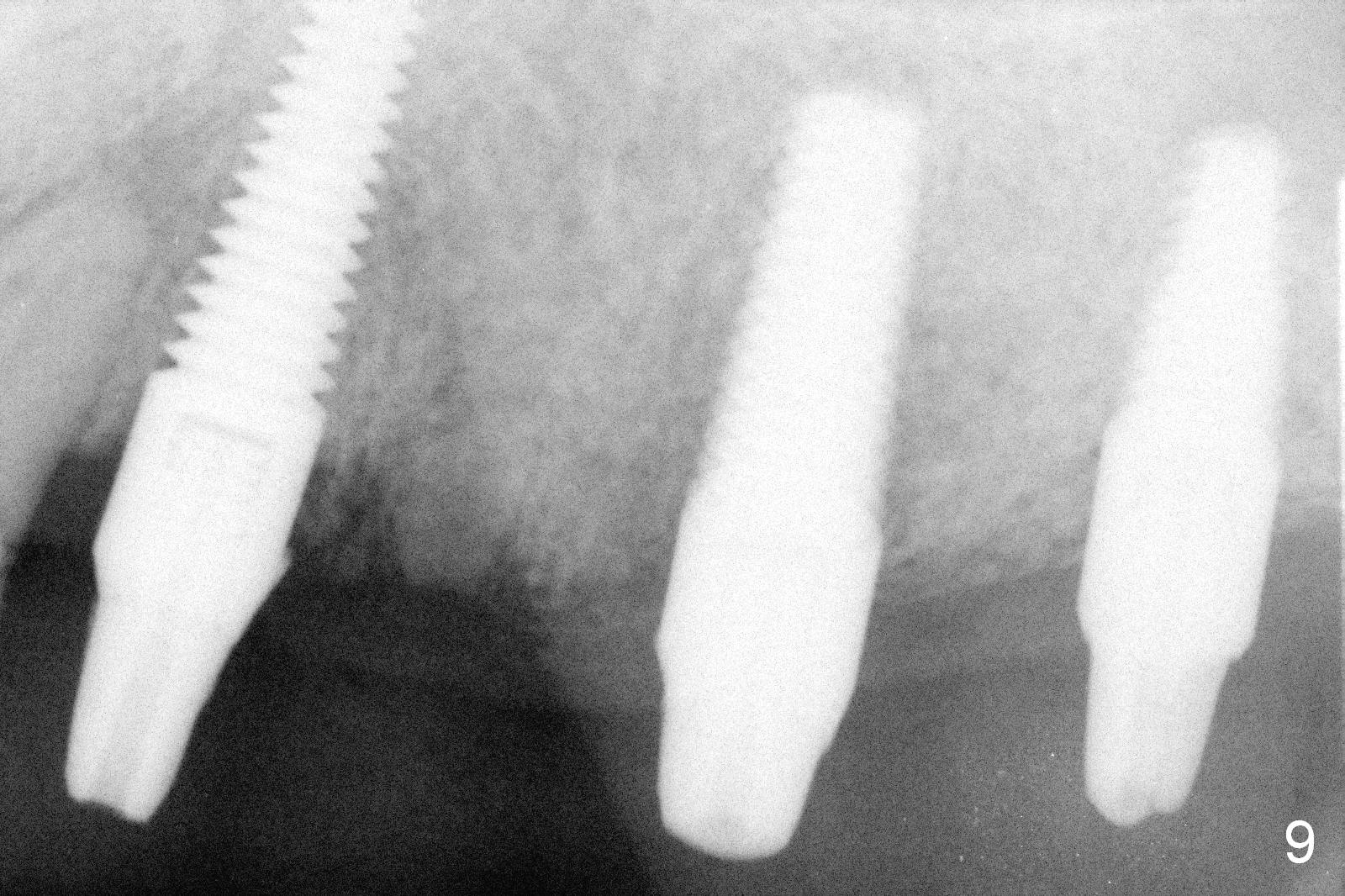
The patient returns for definitive restoration 3.5 months postop (Fig.9). A full arch custom tray is used to take final impression. Bite registration is taken. The opposing arch is available in the lab shelf. Make a 3-unit bridge between #11 and 14 (one premolar) and a single-unit at #15. Technician: please mount properly and check occlusion repeatedly.
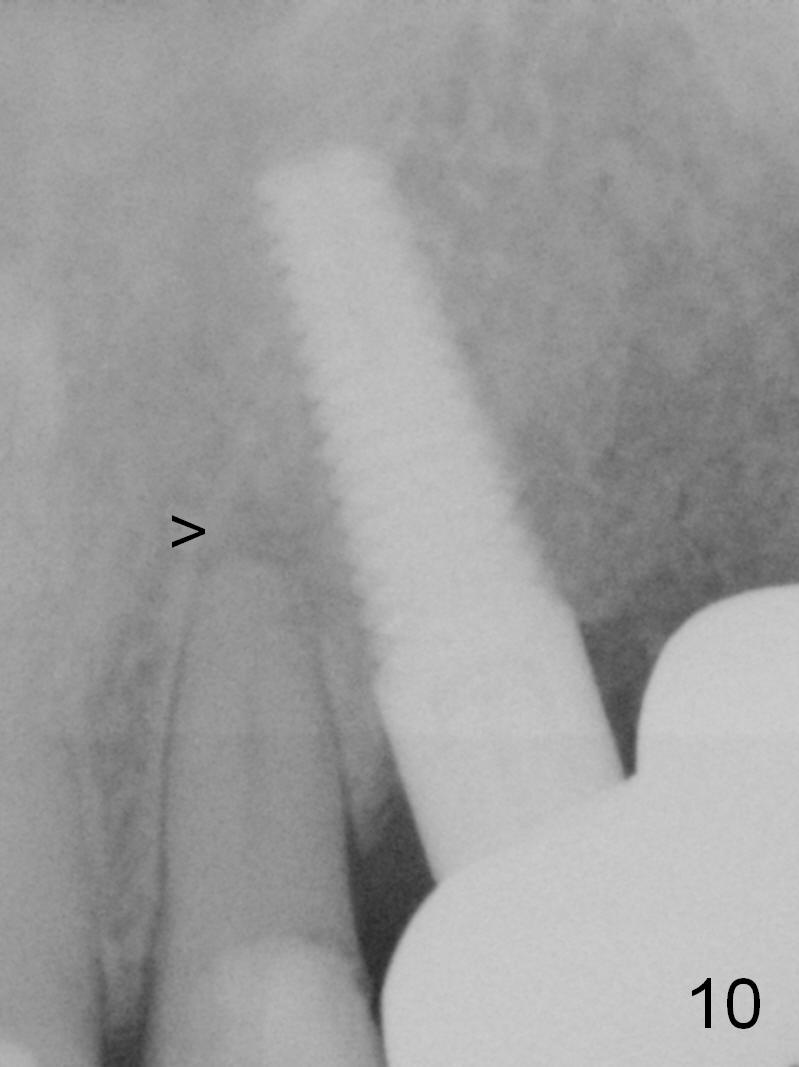
There is pain on mastication around #11, reported by the patient, 7.5 months postop (3 months post cementation). The patient refuses RCT for the tooth #10 with periapical radiolucency (Fig.10 >).
The patient keeps complaining of mastication pain on the left, 4 months post cementation (Fig.11). In fact, there is distal caries at #19 (<).
Return to Upper Arch Immediate Implant,
Technicians,
Training 1
2
Xin Wei, DDS, PhD, MS 1st edition 12/14/2015, last revision 06/25/2017