


.jpg)





|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
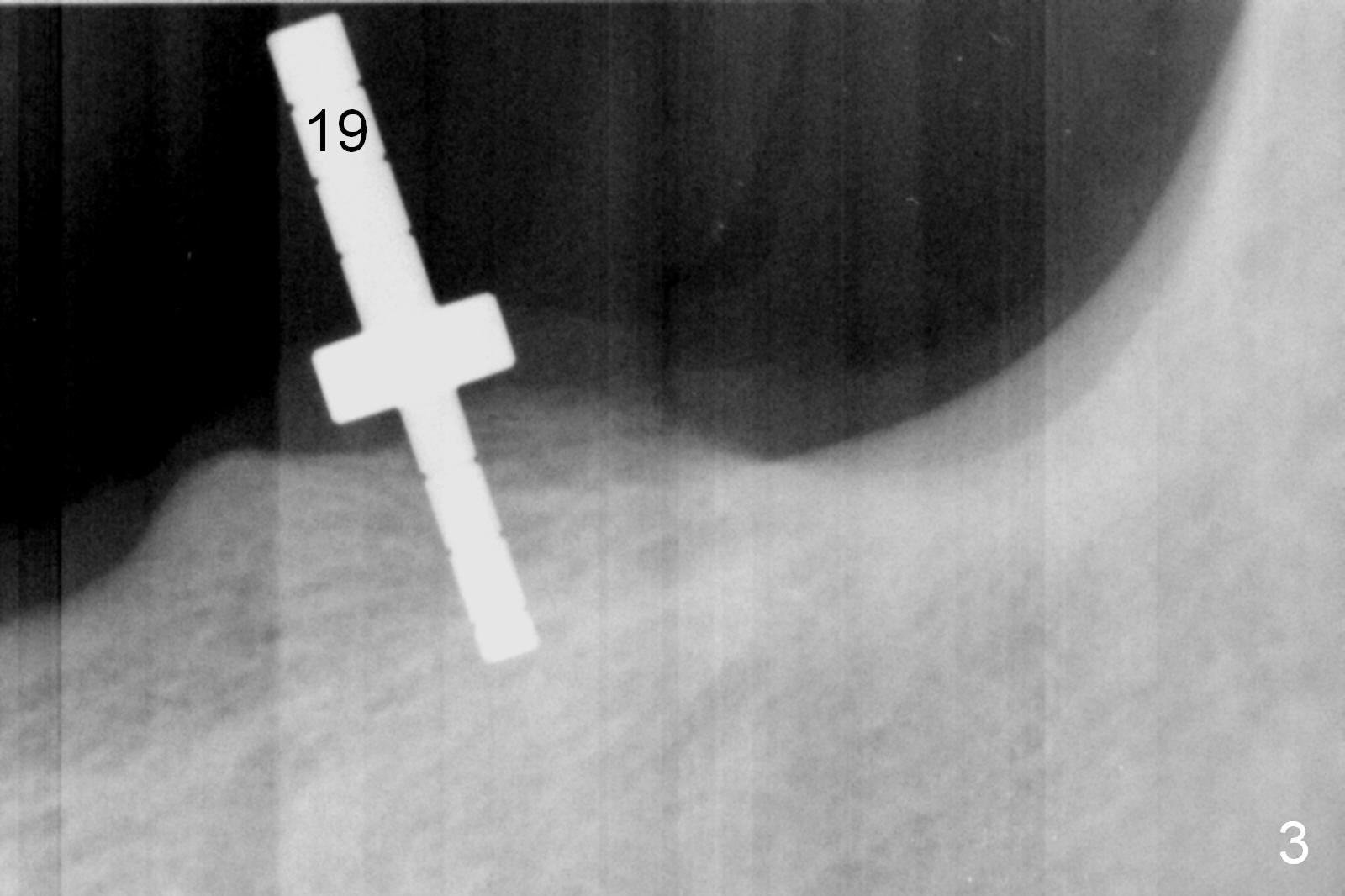
Longer Guide Pin is Needed
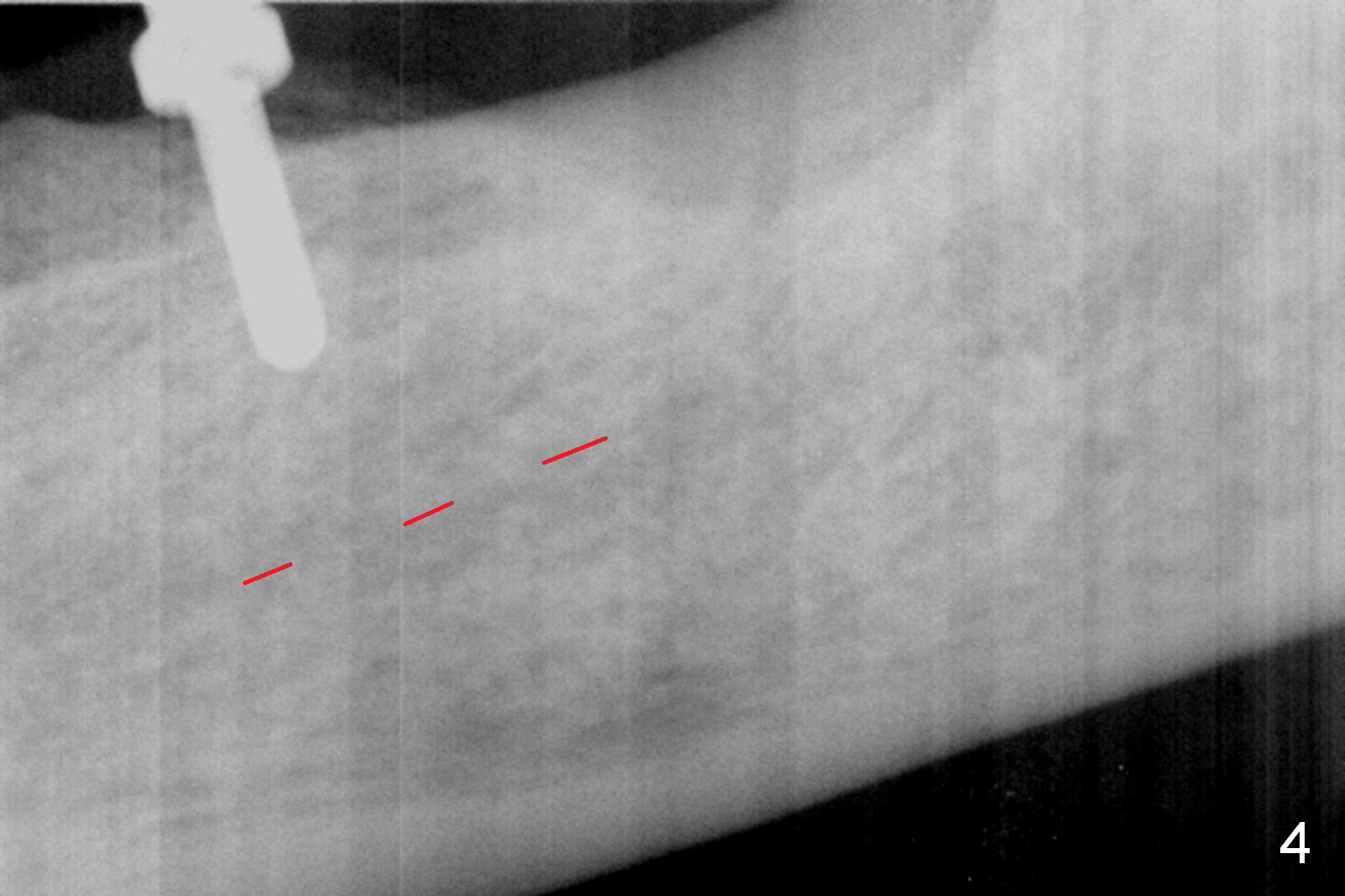
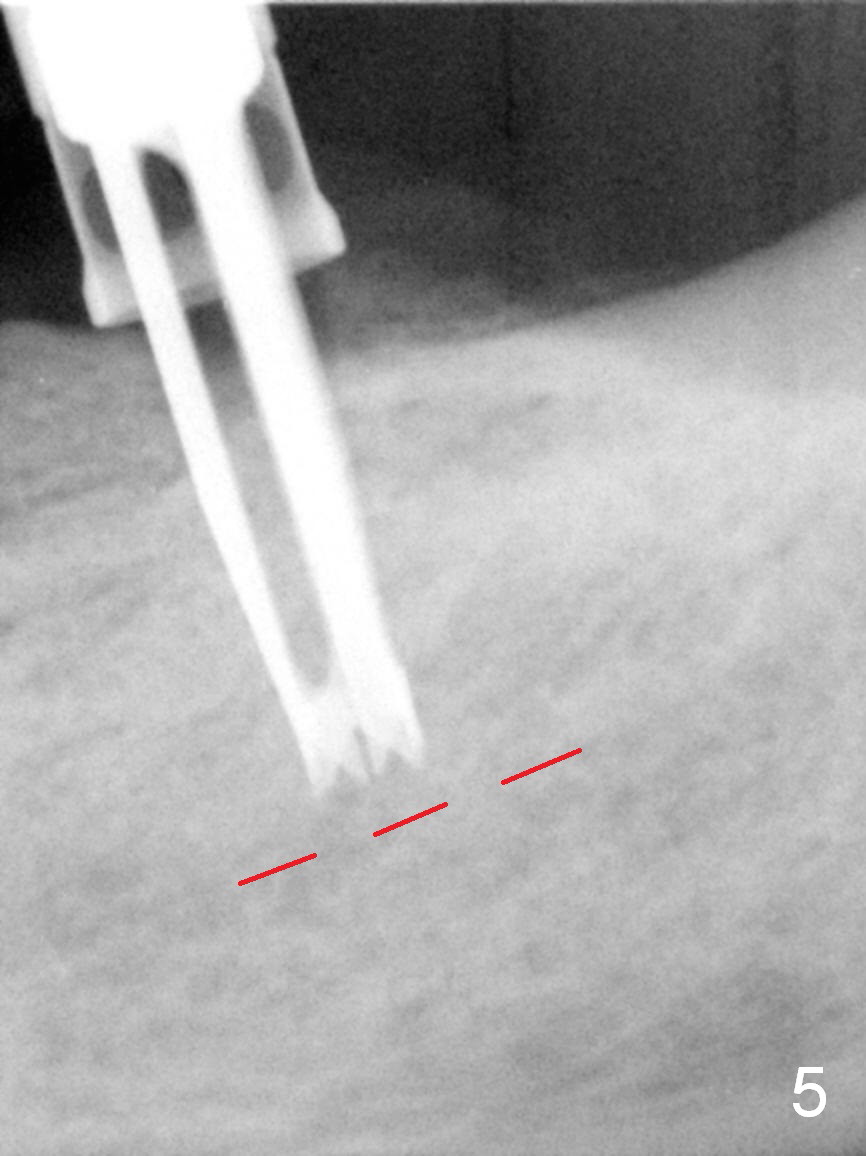
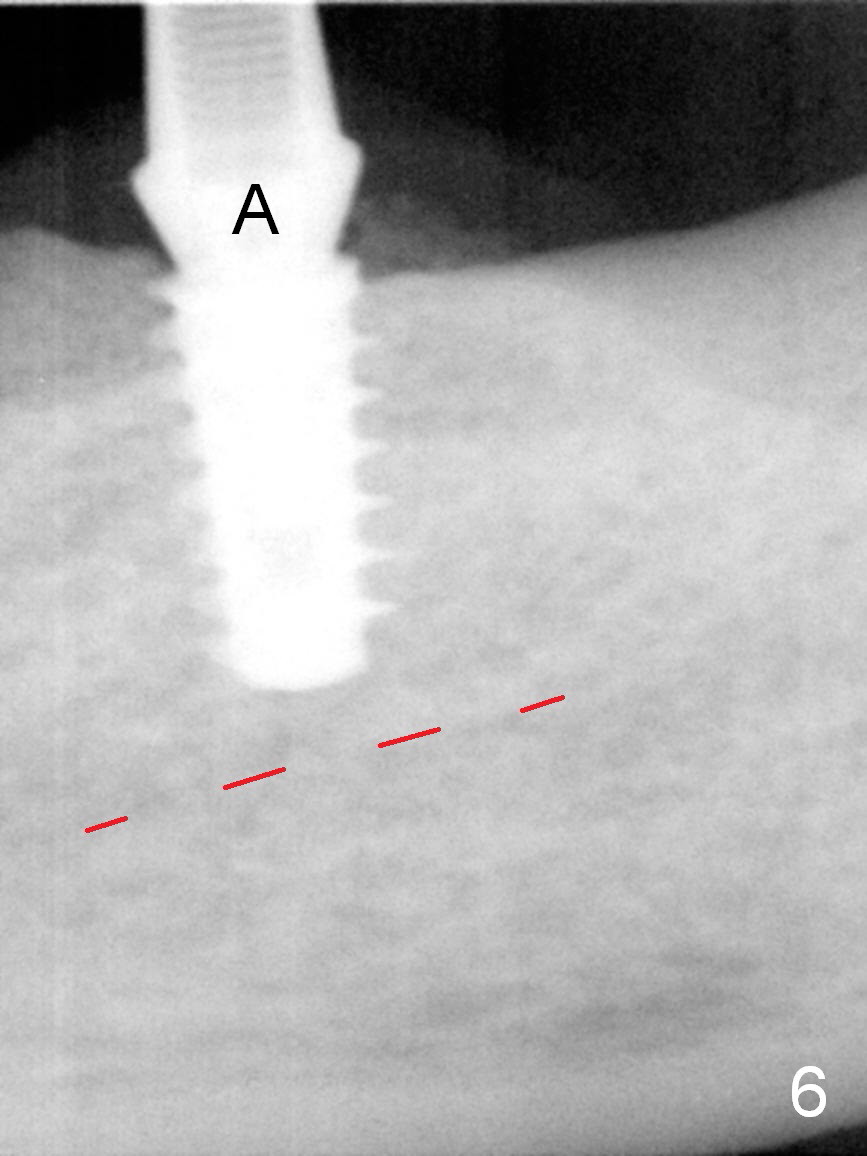
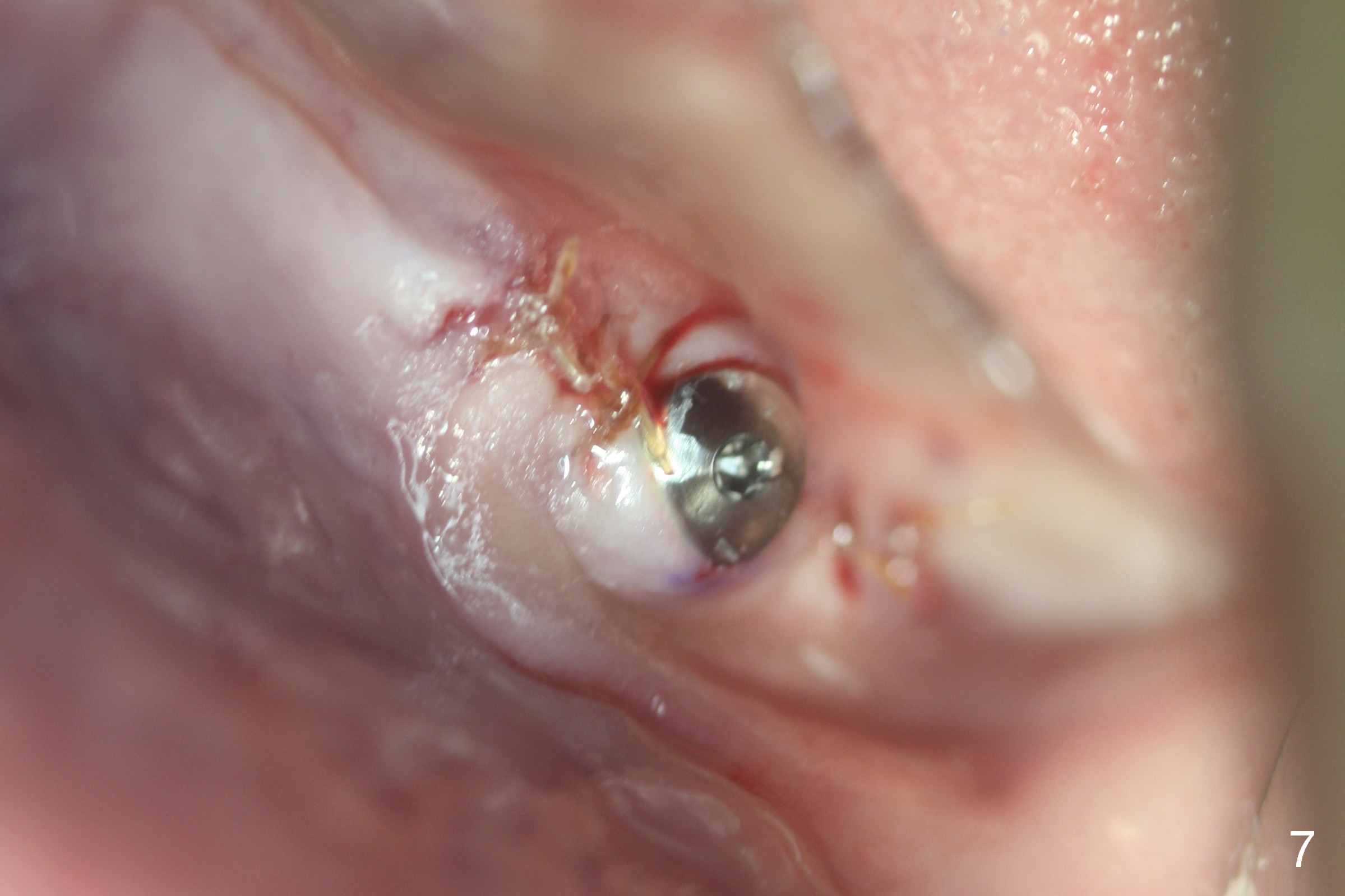
Except the tooth #30, the patient is completely edentulous (Fig.1,2). His chief complaint is "food gets into the missing tooth area". Due to short guide pin (Fig.3) and parallel pin (Fig.4), it is difficult to calculate precisely at the site of #19 the distance to the superior border of the Inferior Alveolar Canal (Fig.4 red dashed line). The clearance appears to be limited when a 4.3 mm drill is in place with 11 mm depth (Fig.5). Therefore an implant shorter than the last drill is placed (5x9 mm, Fig.6). Insertion torque is >50 Ncm. A 5x4(2) mm pair abutment is inserted temporarily to check occlusion with the opposing dentition (A). Finally a 5x2 mm healing abutment is placed with harvested autogenous bone placed between the implant and abutment (Fig.7). Before discharging the patient, the lower RPD is in place to check the position of the implant/abutment (Fig.8).
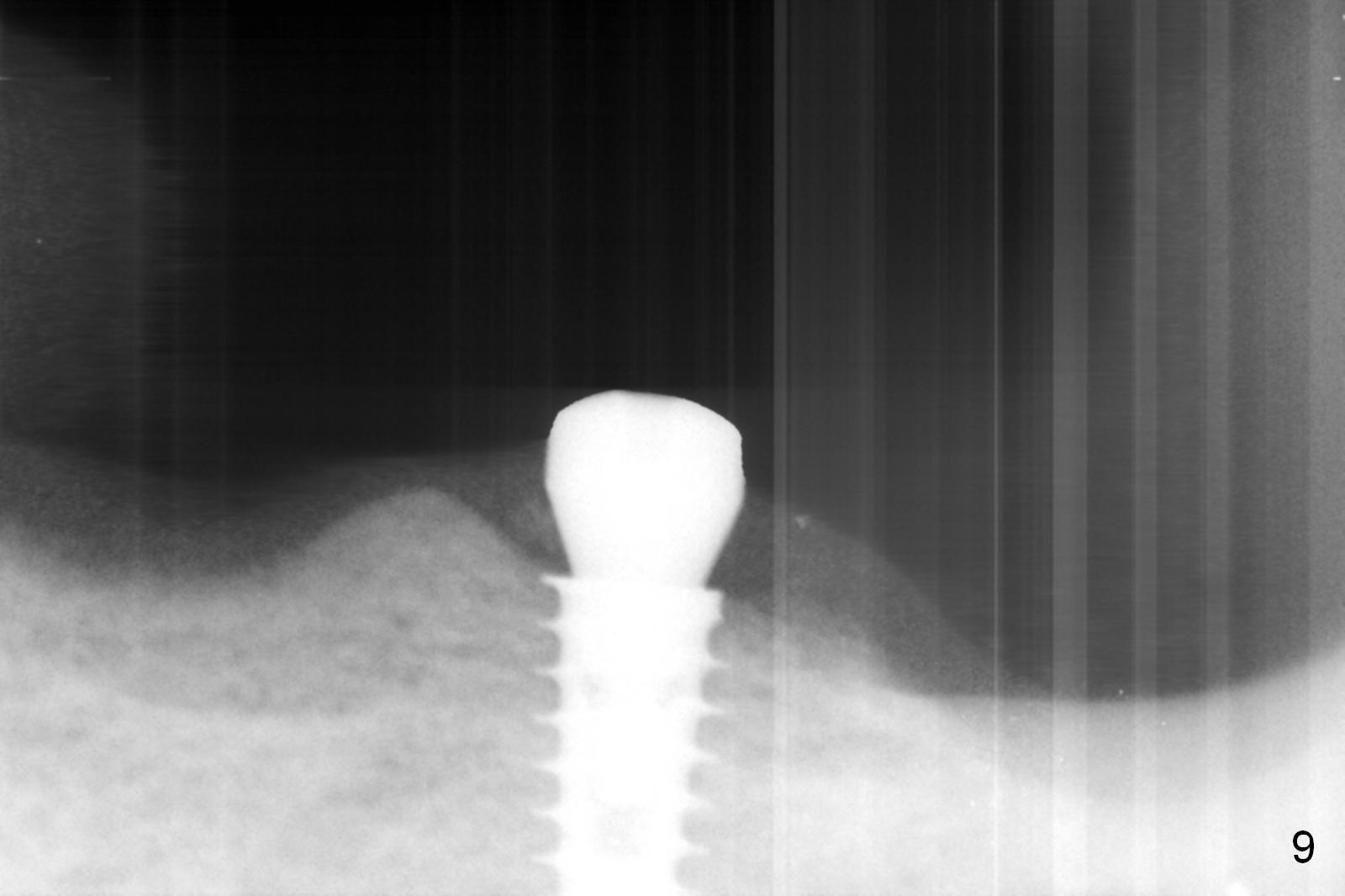
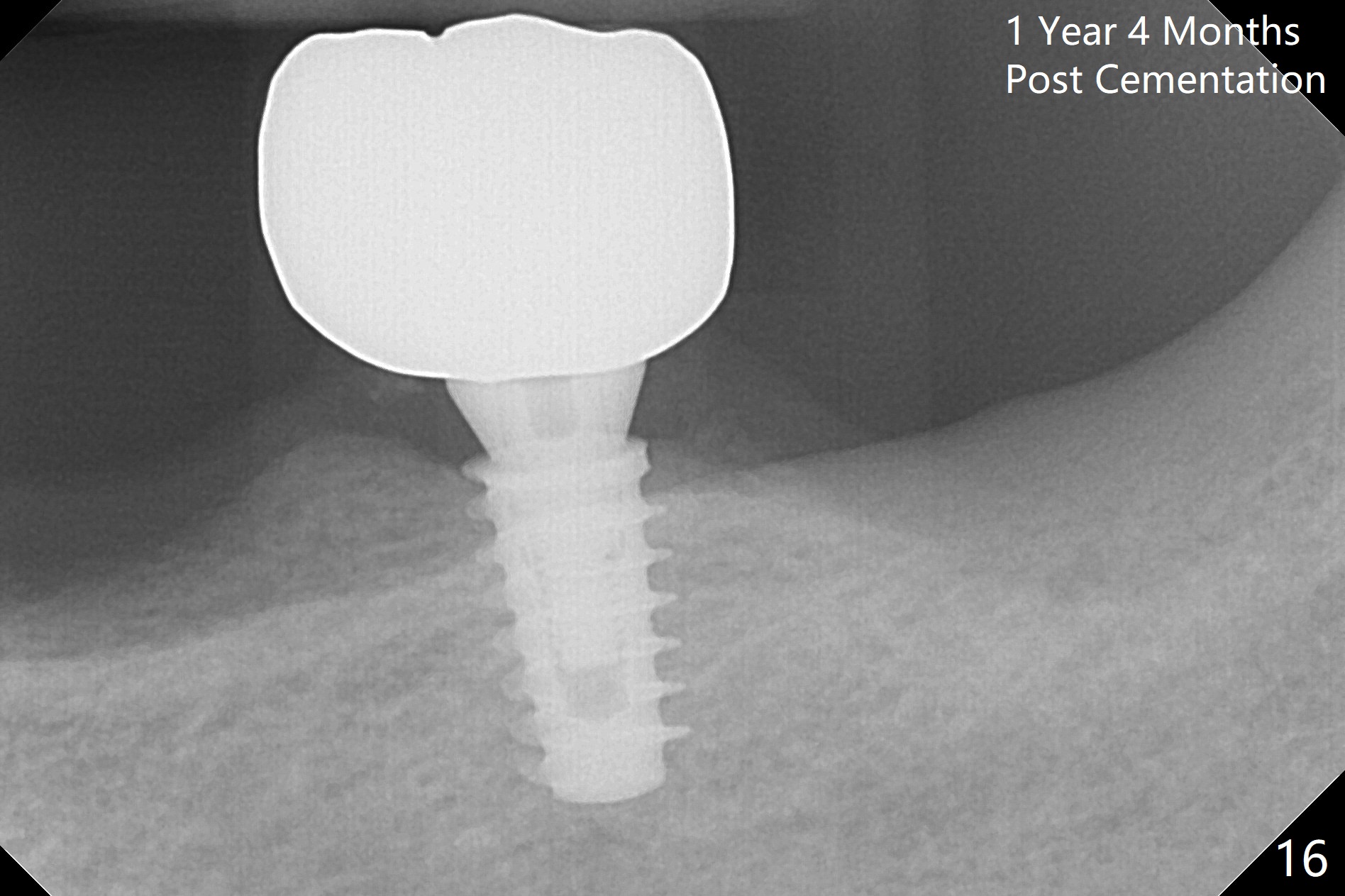
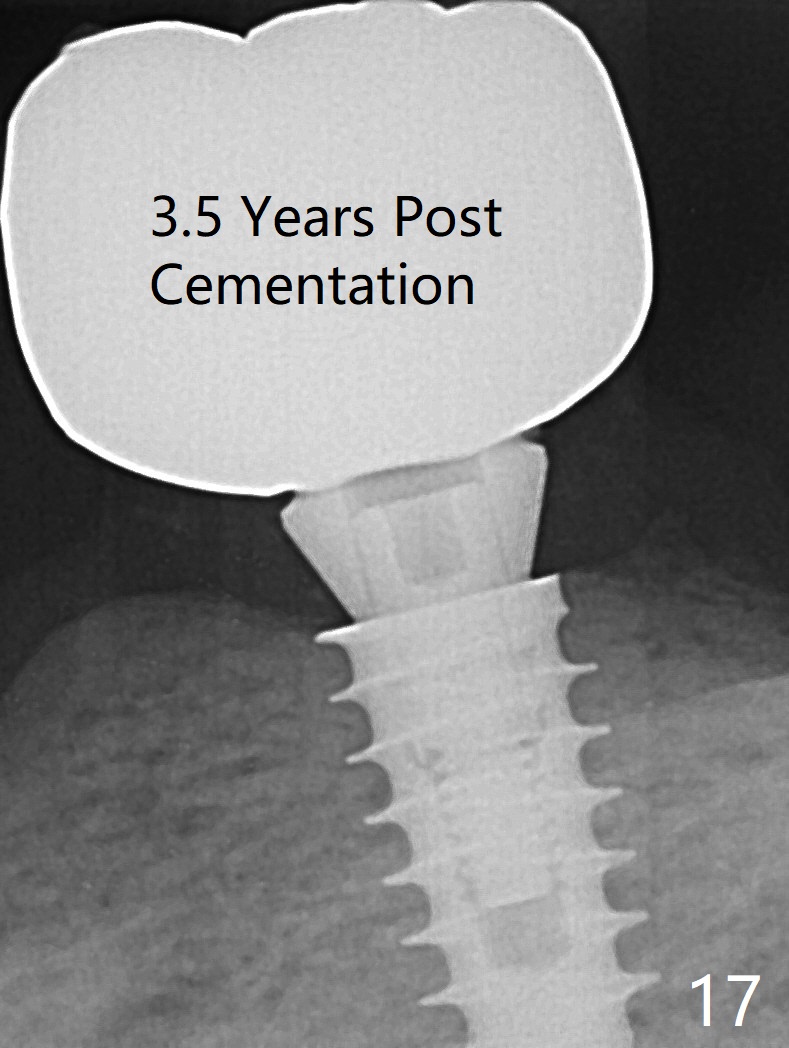
The implant osteointegrates 2 months postop (Fig.9). A pair abutment is placed (Fig.10: 5x4(2) mm) for a provisional (Fig.11). Wax up for final restorations (Fig.12-15). There is no bone resorption 1 year 4 months post cementation (Fig.16). The RPD is doing fine. The implant remains stable 3.5 years post cementation (in spite of open margin), while the other abutment for the RPD (the tooth #30) has mobility with gingival recession.
Return to
Lower Molar Immediate Implant,
IBS,
Thread Patterns,
Course
2
Xin Wei, DDS, PhD, MS 1st edition 07/28/2016, last revision 10/25/2020