


|
|
|
|
|
|
|
|
Extraction Complication Results in Change of Procedure
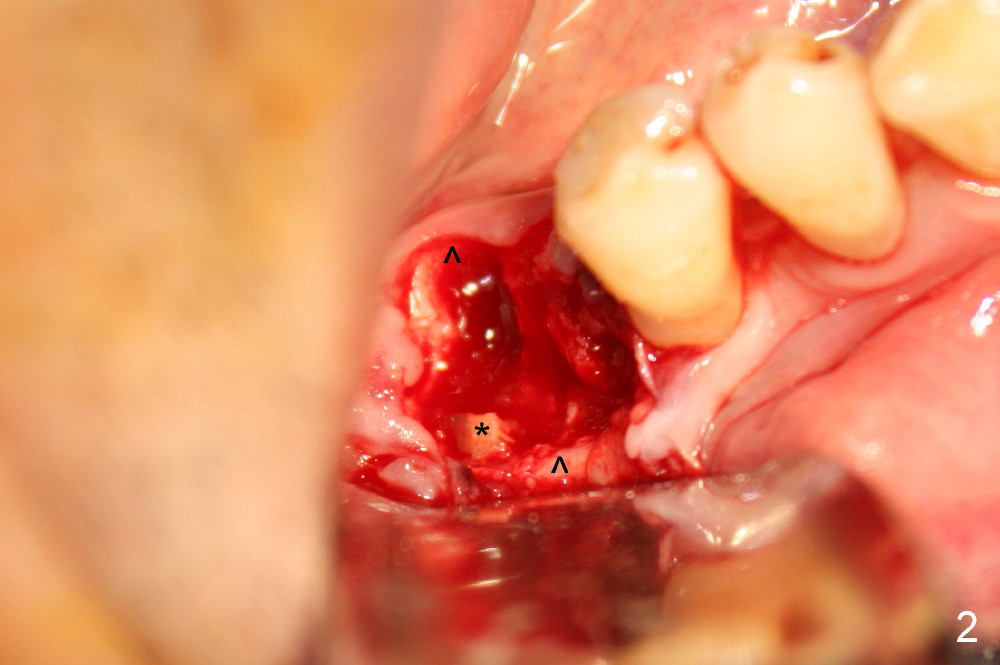
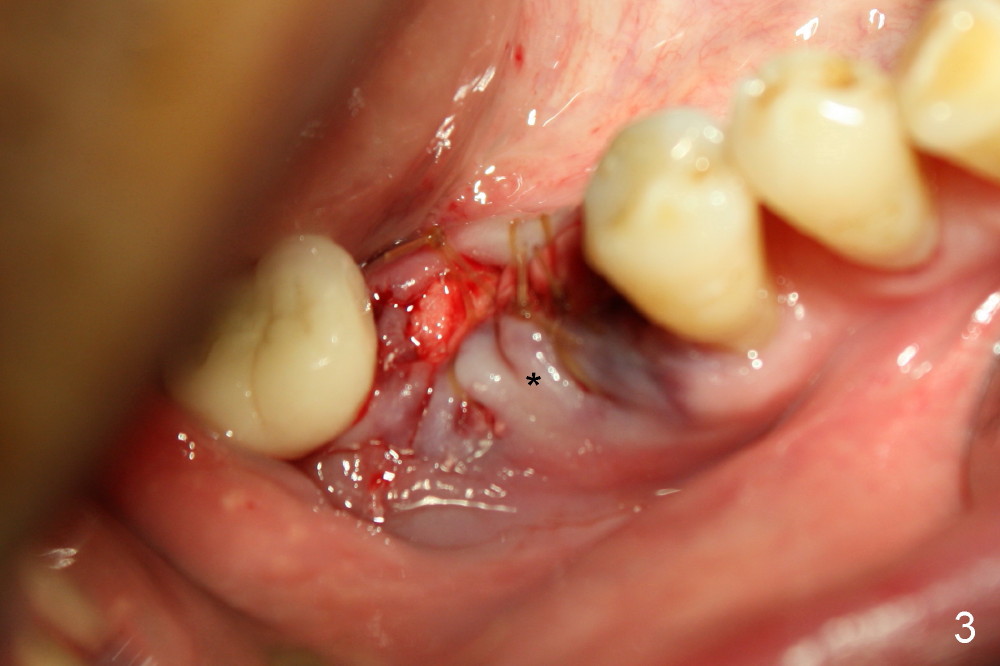
When the patient presents for consultation, the tooth #30 shows crack line. Two weeks later when he returns for extraction and immediate implant with possible immediate provisional, the tooth has infection (Fig.1 <). He has taken oral Clindamycin for 2 days, which is our immediate implant protocol. In order to prevent accidental injury to the inferior alveolar nerve, infiltration with Xylocaine and Septocaine is administered outside of the swelling. The tooth is sectioned with surgical bur. Extraction turns out to be difficult. The patient develops transient chest discomfort and systemic shivering intraoperatively, which is consistent with bacteremia. Bacteria are apparently pushed into blood stream during injection and root retrieval. When the symptoms subside, the patient does not want to have an immediate implant placed. Immediately prior to distal root tip removal (Fig.2 *), inferior alveolar nerve block is administered. Photos are taken to show that the buccal plate is lower than the lingual one (Fig.2 ^). It appears that bone graft would be more secure when an immediate implant is placed (implant threads as a framework, coral) than without the implant. But the patient is adamant. When allograft/Osteogen is placed followed by Collagen Plug, the buccal plate is apparently collapsing (Fig.3 *). If an implant were placed, the collapse would not be so severe. The implant should be able to provide with bulkiness. We will see the result of socket preservation. Delayed implant is planned in 6 weeks.
The patient returns for implant placement 8 weeks post socket preservation. As expected, the buccal plate is atrophic (Fig.4). To preserve blood supply from the periosteum, a 4 mm tissue punch is used for access. Three implants are tried without primary stability. There is postop pain. The implant exfoliates less than a month postop (Fig.5, photo taken 2 days post exfoliation).
Retrospectively, non-resorbable membrane with Titanium framework should be used to keep space for socket preservation.
Now it is 5 months post exfoliation. The buccal plate should remain atrophic. Incision will be made for the best vision, place an implant in the best possible position and place bone graft buccally. Take preop PA and photos. The patient is a gagger. Prepare Ethanol, wipe his finger and let him hold the sensor in place.
Return to Lower Molar Immediate Implant, Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 11/07/2014, last revision 01/19/2018