.jpg)
|
|
|
|
|
|
|
|
|
|
Drill Stop from Sinus Master Kit
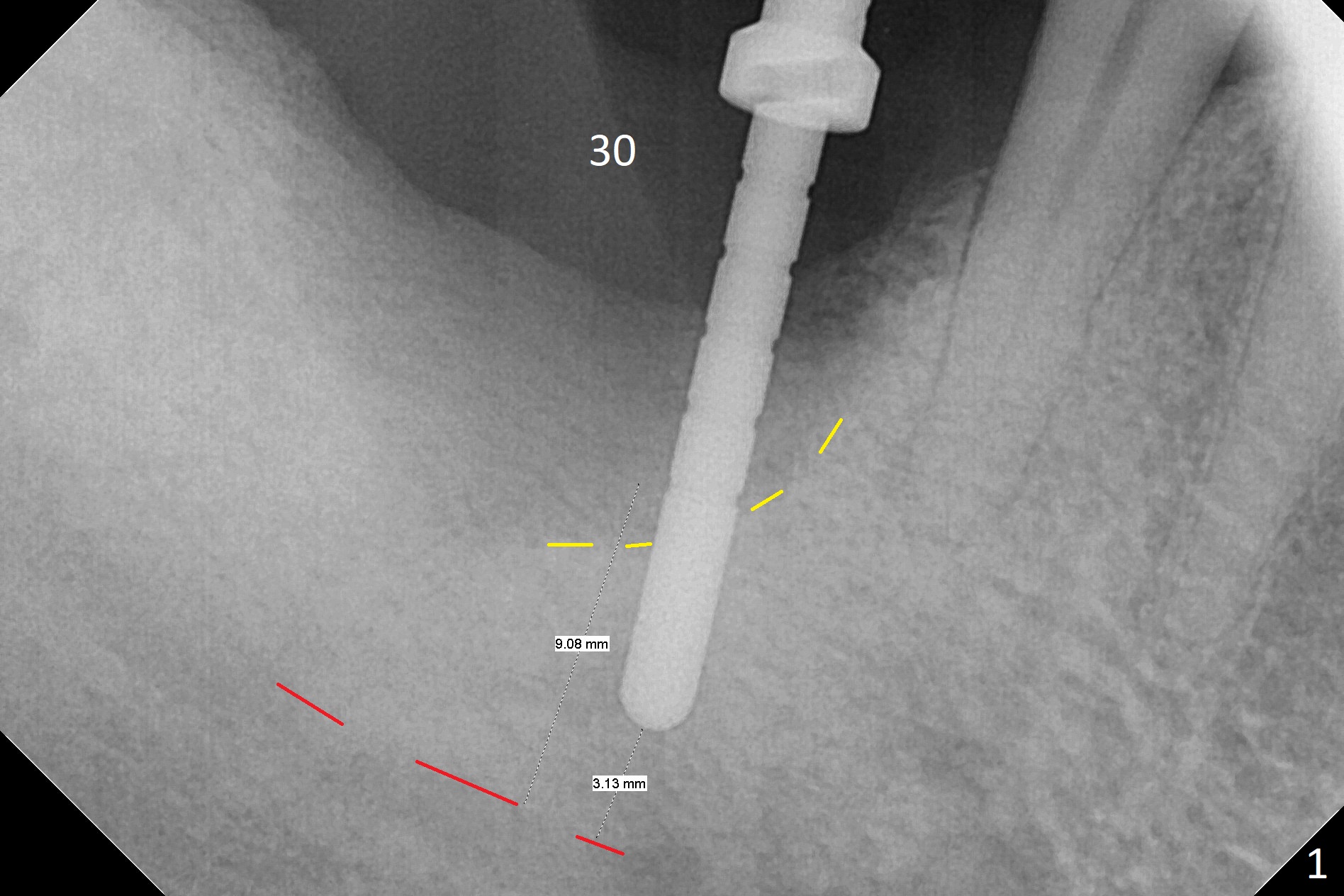
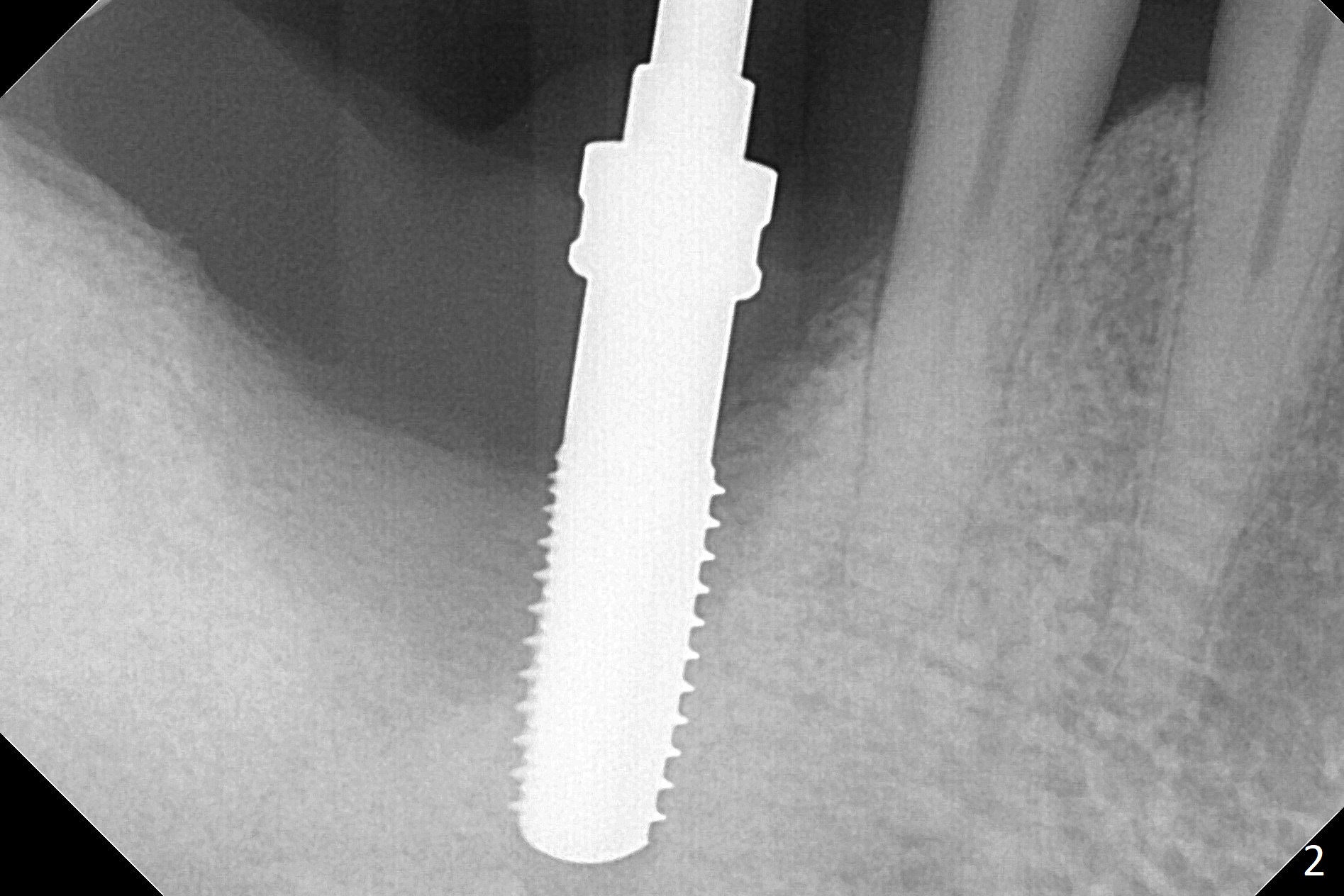
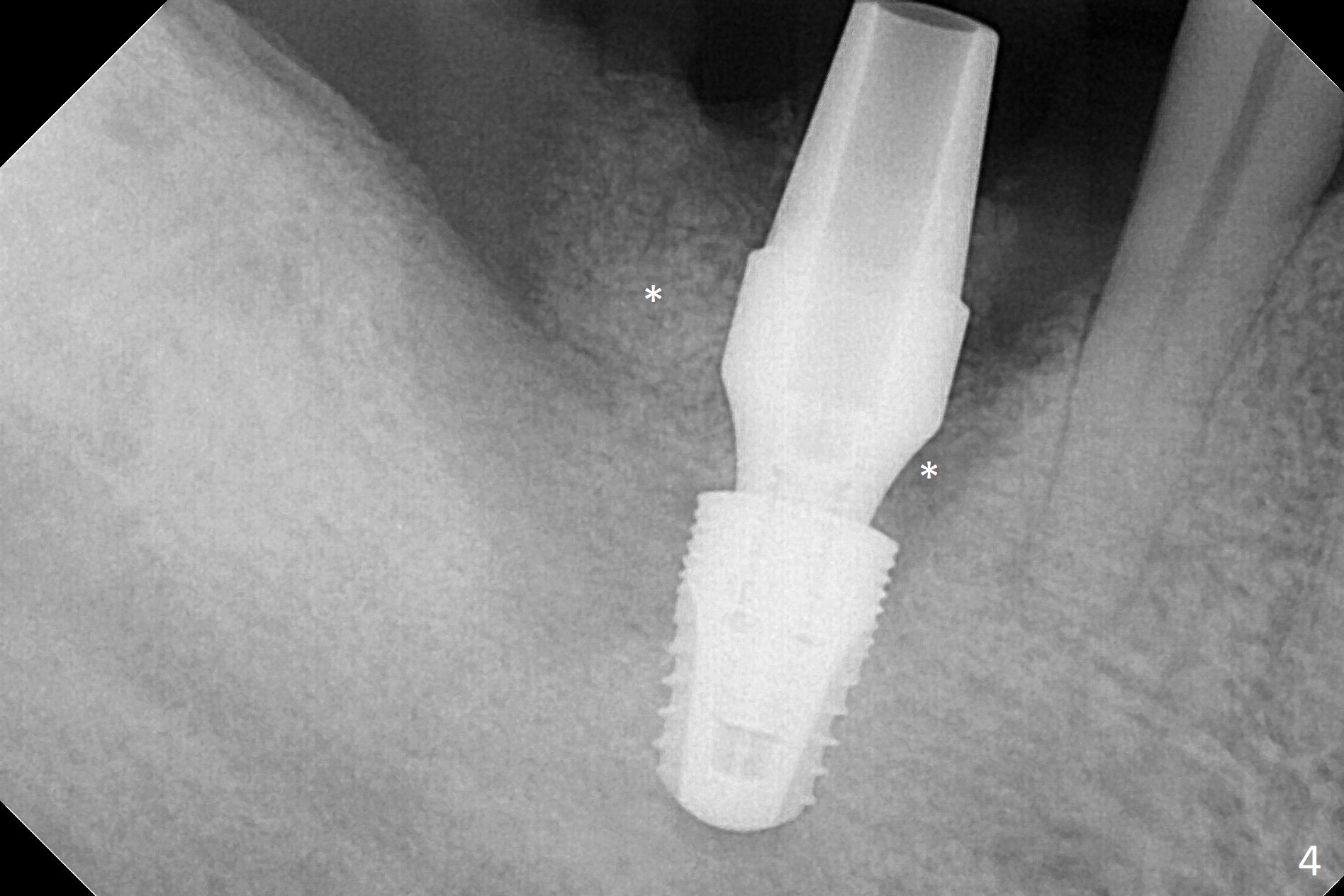
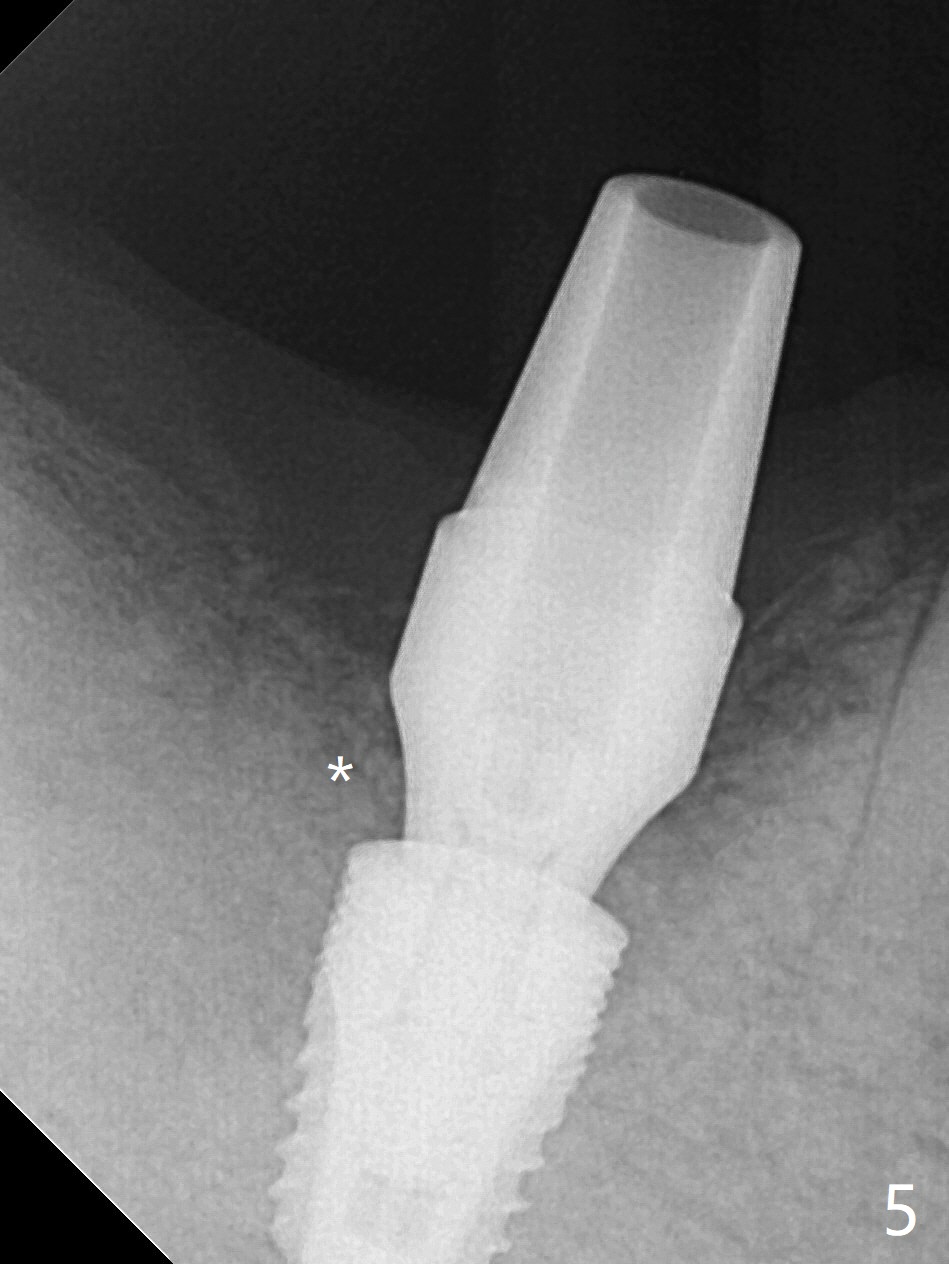
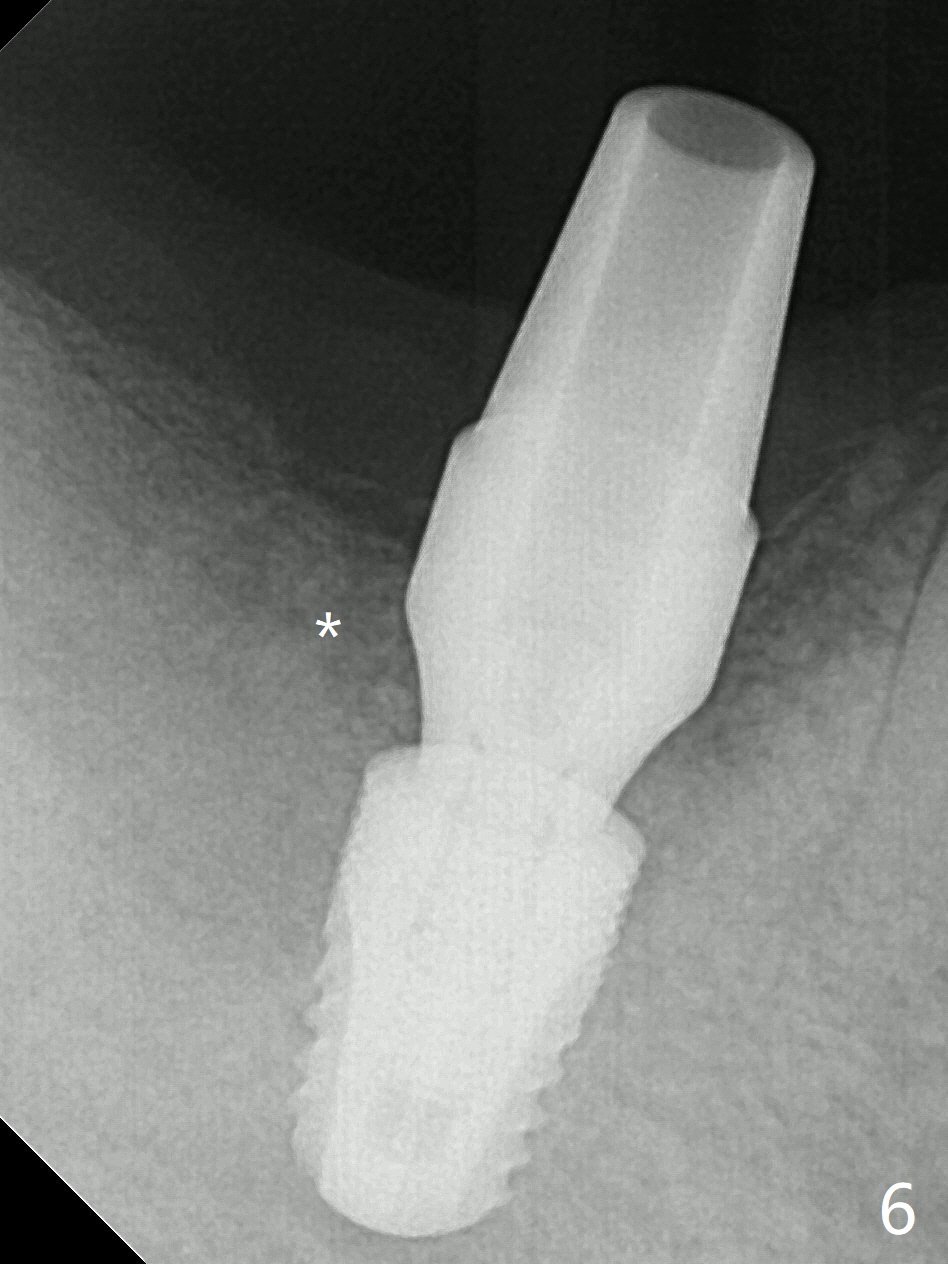
After extraction of the tooth #30, hemorrhage is excessive. With incision and buccal flap elevation, it is easy to remove residual granulation tissue and see the bony defect. With gauze pressure, hemostasis is manageable. Osteotomy is established in the mesial socket, i.e., mesial slope (Fig.1 yellow dashed line) with 2 mm initial drill from DIO Sinus Master Kit with 6 mm stop. After use of 3.8 and 3.6 mm round burs from the Master Kit for 6 mm, 4.1-5x8 mm drills from SM Kit are used with 50 RPM to control depth until the patient feels light pain with infiltration anesthesia. A 5.3 mm tap drill is inserted with 50 Ncm (Fig.2). A 5.3x8 mm SM implant is placed with >55 Ncm with clearance from the Inferior Alveolar Canal (Fig.3 red dashed line) with tightening a 5.8x7(6) mm abutment. The implant is subcrestal mesiolingually, equicrestal buccally and supracrestal distally (Fig.3 thread exposure distally between arrows). With Osteogen plug placed in the distal socket, allograft is placed around the implant and abutment (Fig.4 *). Periodontal dressing is applied following buccal placement of Collagen Dressing and suturing. The gingiva around the abutment is healthy 3.5 months postop; new bone appears to form distocoronal to the implant (Fig.5,6 *).
Return to
Lower
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table), IBS, #13
Xin Wei, DDS, PhD, MS 1st edition 06/30/2017, last revision 01/14/2018