
.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
Ridge Reduction
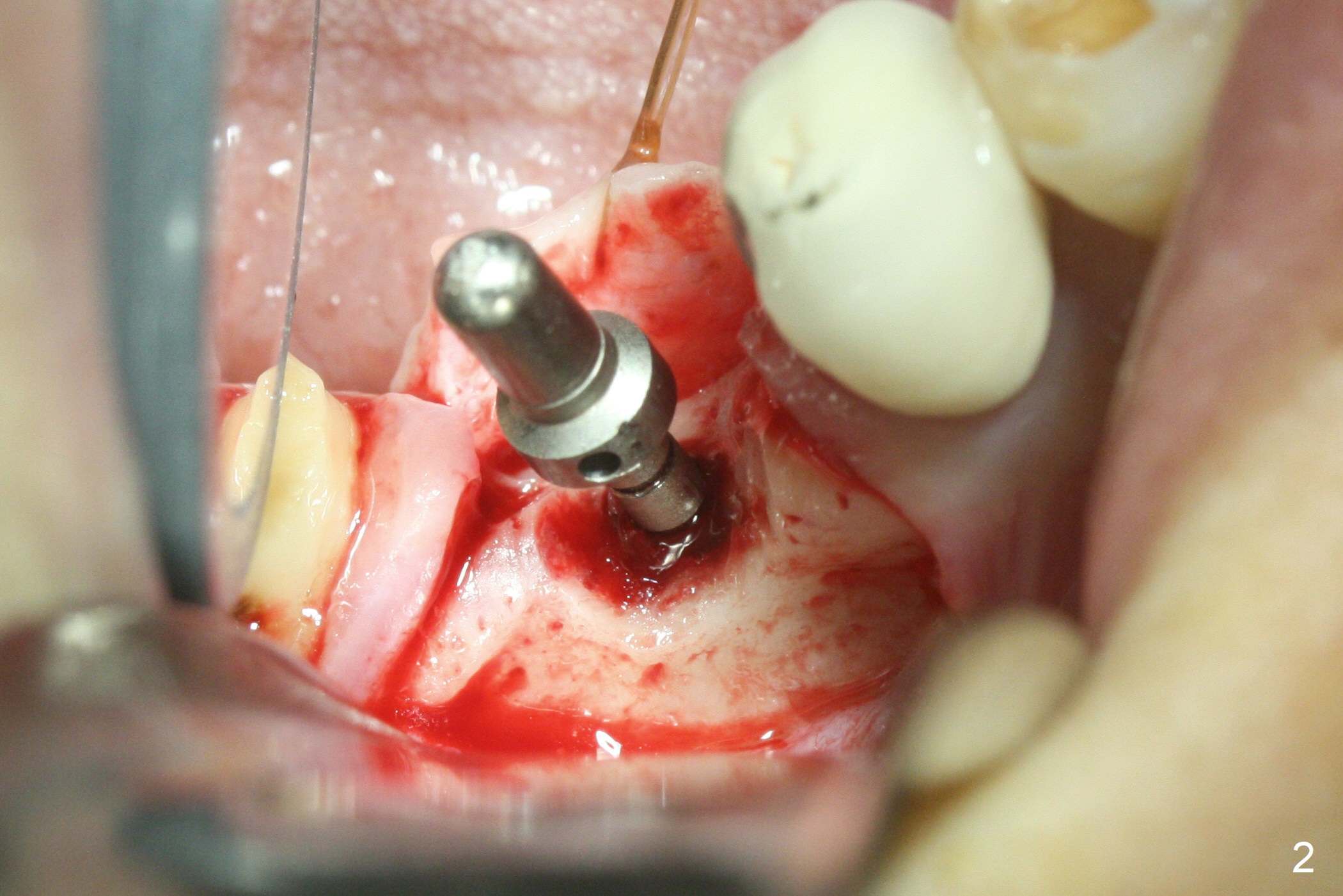
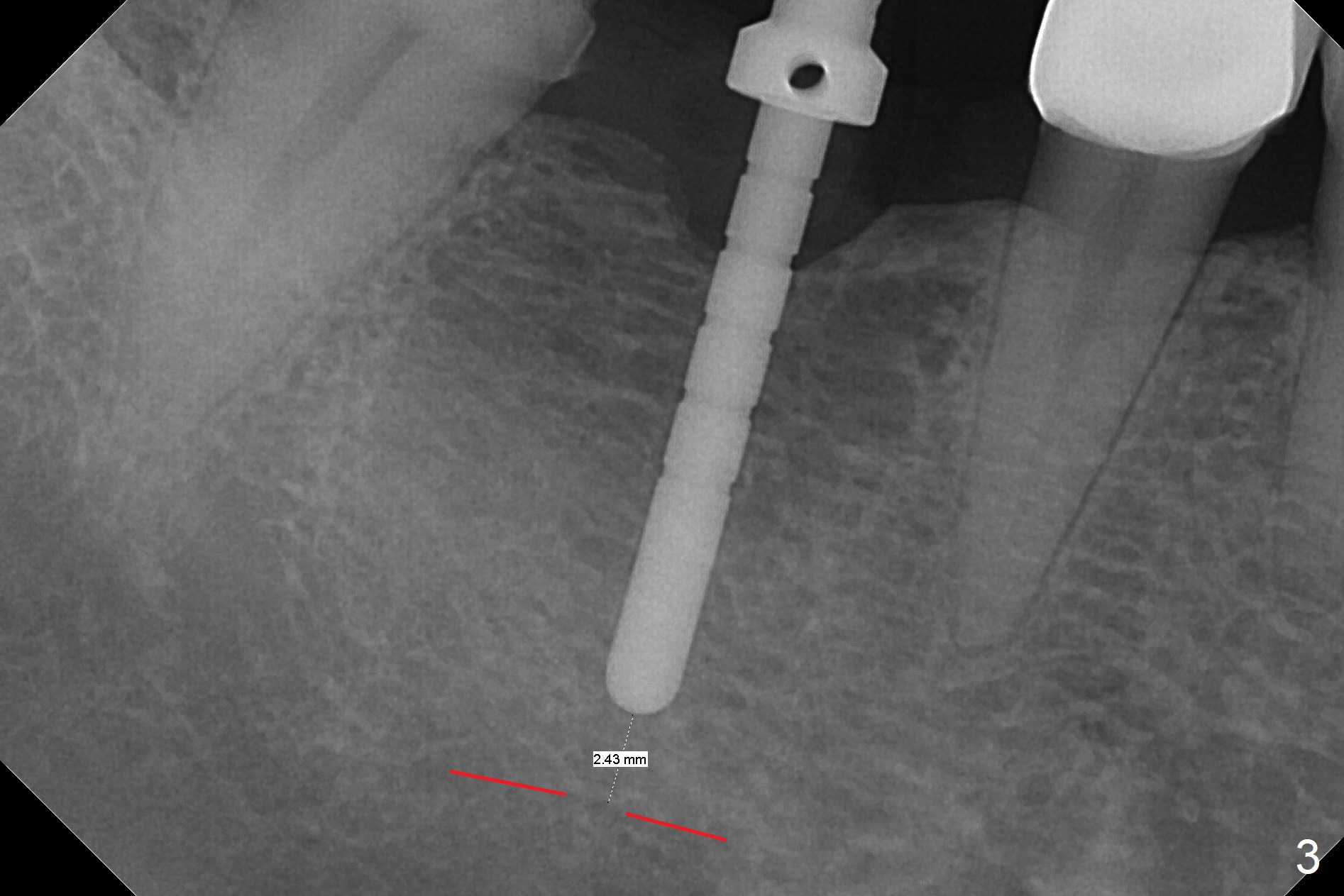
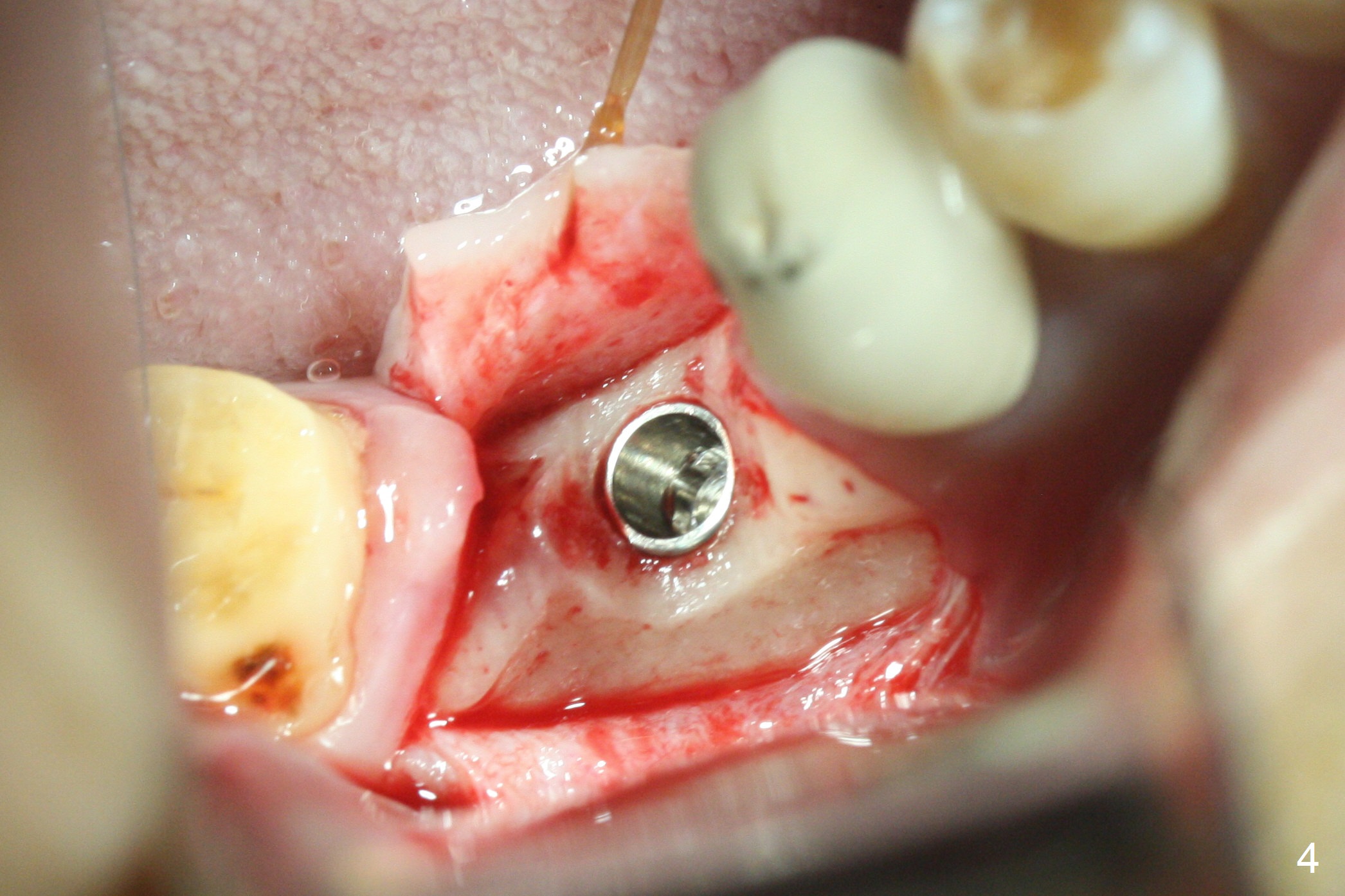
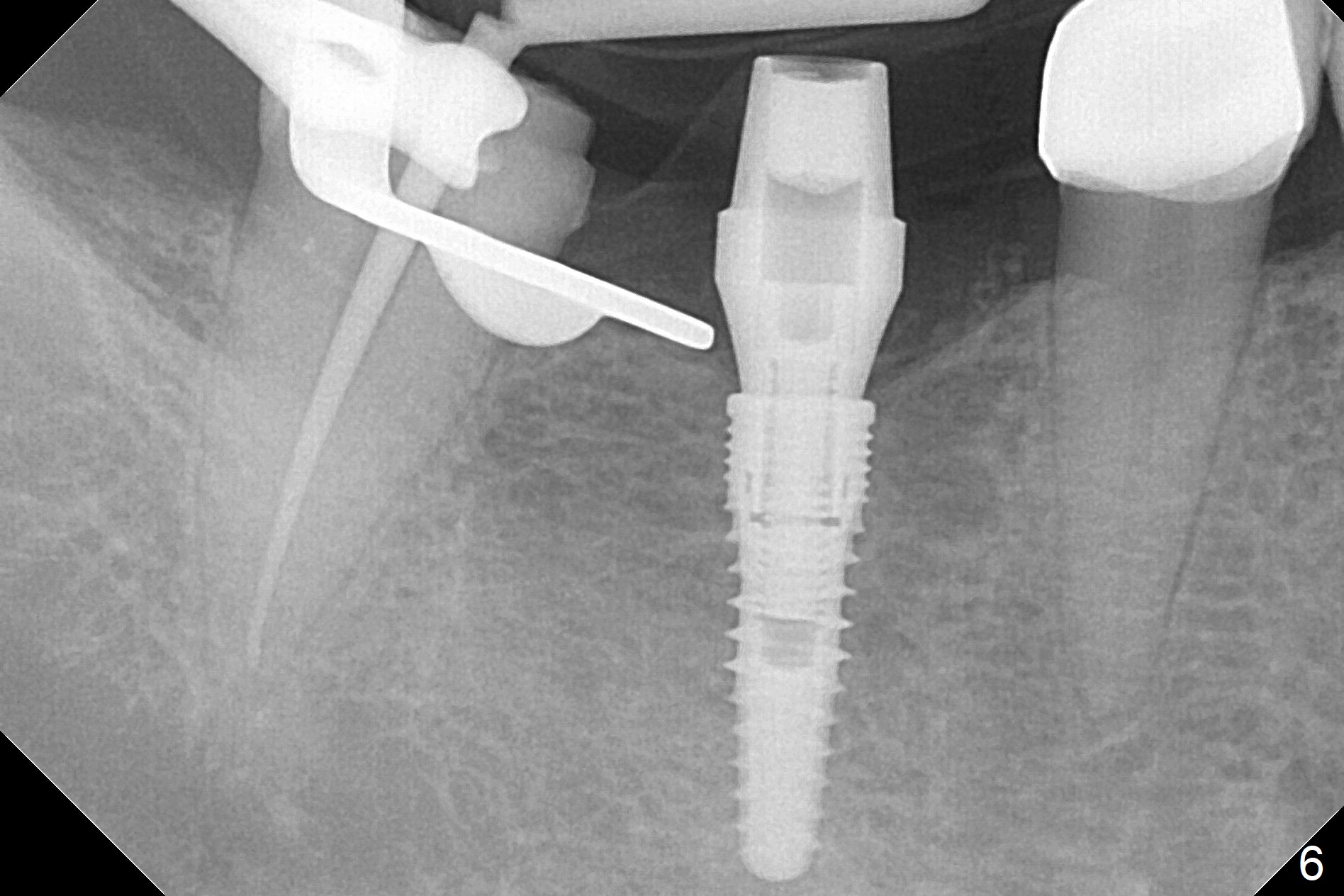
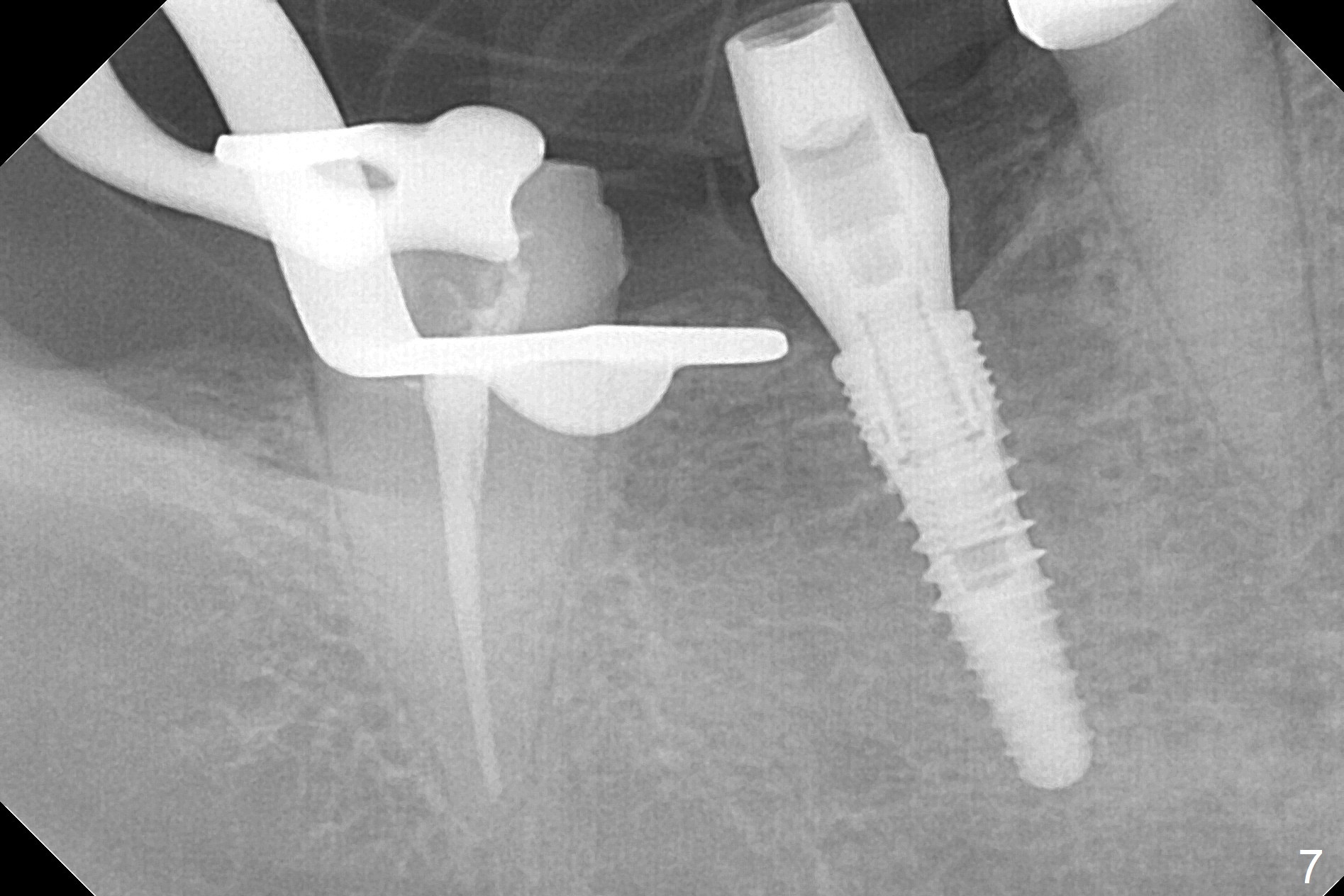
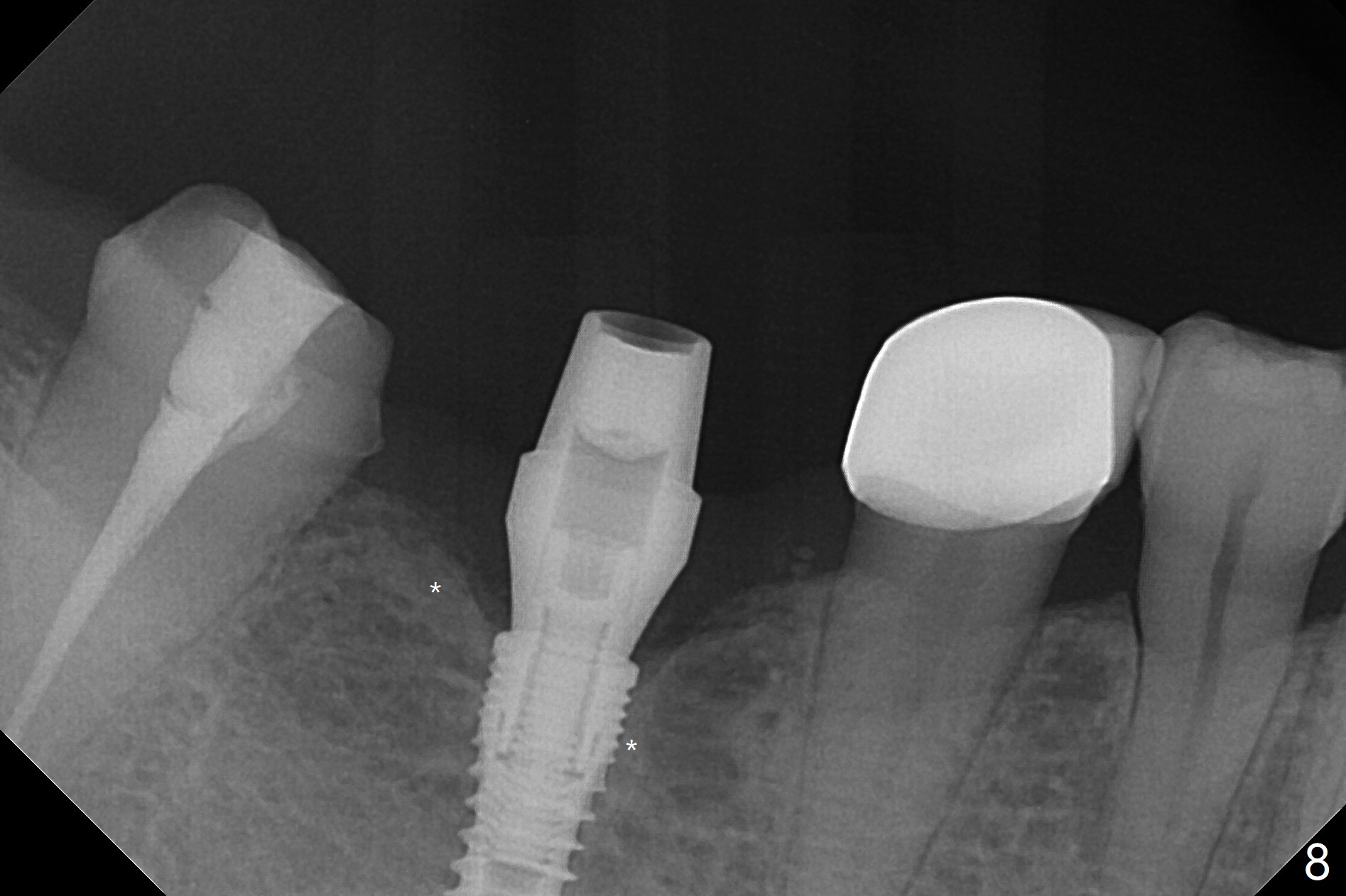
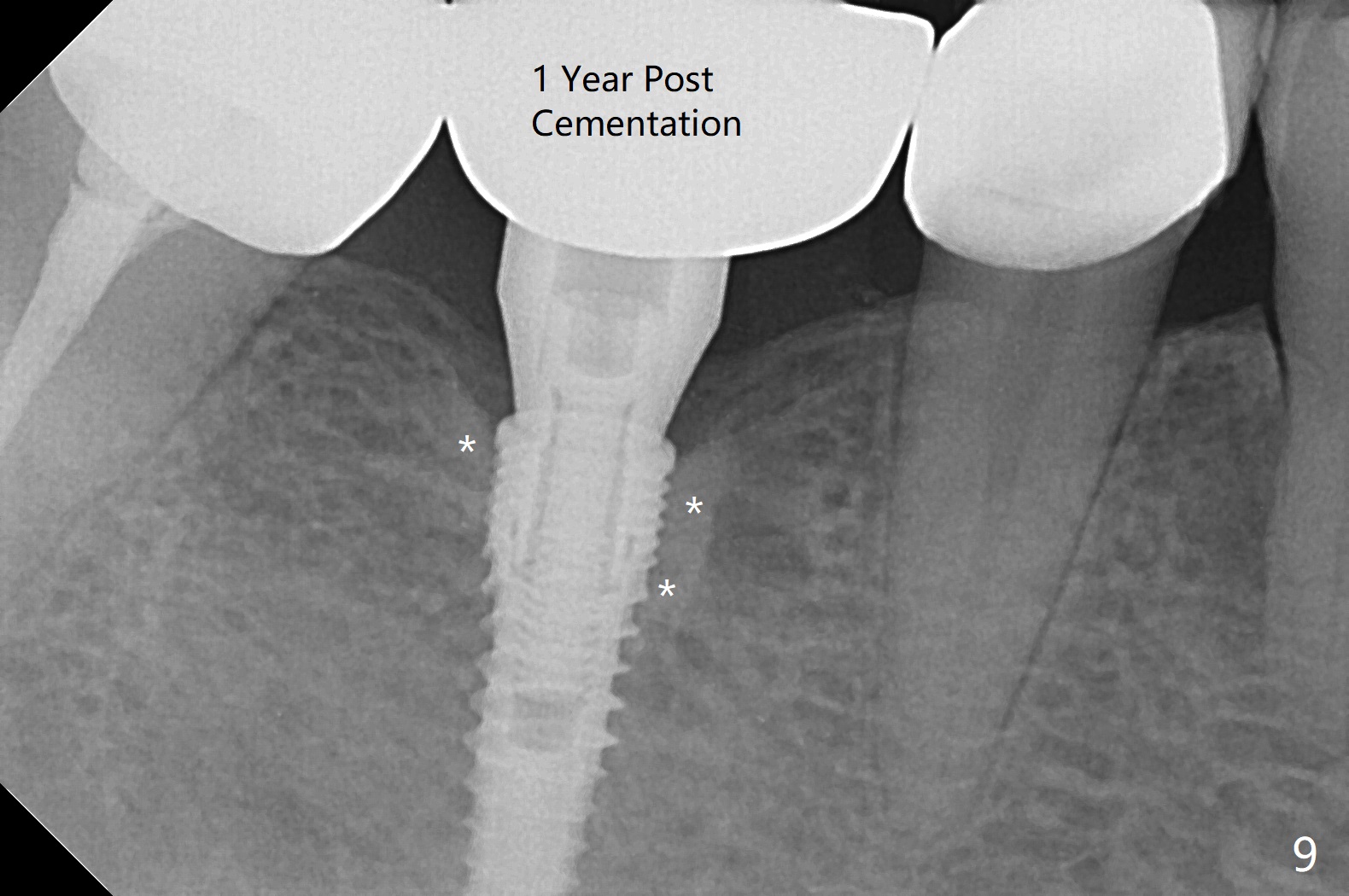
The apparently narrow ridge at #30 before bridge sectioning (Fig.1) is confirmed with incision (Fig.2). Following ridge reduction, osteotomy is initiated with 2 mm pilot drill (Fig.3). When a 3.8x12 mm SM narrow implant is placed with 40 Ncm, there is 1-2 mm cortical bone buccolingually (Fig.4,5). The thick cortices do not seem to be easy to be bent, i.e., expanded. RCT is finished at #31 one month post implant placement (Fig.6,7), the flattened ridge appears to have started to undergo remodeling. Ridge reduction makes it possible for the implant to remain subcrestal postop (Fig.4). The bone surrounding the implant may reduce the likelihood of implant fracture. The crowns at #30 and 31will be fabricated together with light occlusion at #30. In fact the splinted provisional dislodges. There appears dense bone formation 3 months postop (Fig.8 *). The drawback of using a SM narrow implant is that a narrow abutment has to be used (4.8x4(4.5) mm). The implant crown is dislodged immediately after the patient finishes lunch. Following recementation, the occlusion is reduced. In fact, UF or IBS has no such drawback: the implant could be small, but the abutment could be large. One year post cementation, the crown at #31 needs recementation (Fig.9); the bone density next to the coronal implant increases (*).
Return to
Lower
Molar Immediate Implant, IBS,
#19
Xin Wei, DDS, PhD, MS 1st edition 07/13/2017, last revision 11/10/2018