



|
|
|
|
|
|
|
|
Goal is to Prevent Nerve Injury
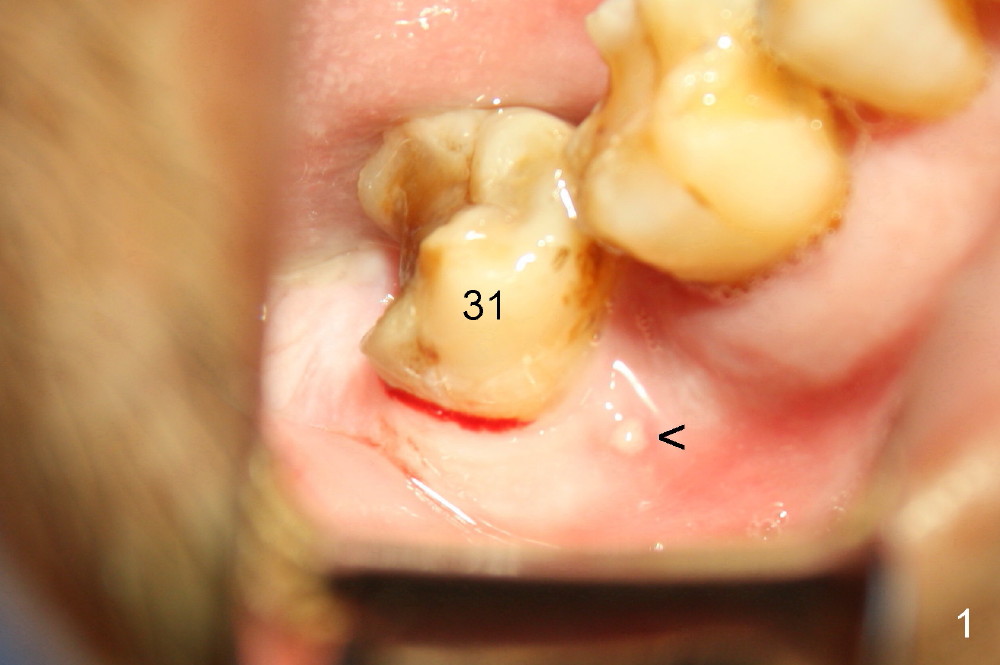
A 52-year-old man (heavy smoker) presents to office without schedule. He has severe pain at #31 and wants extraction immediately (Fig.1,2). He likes the idea of immediate implant, but we do not have time for it that day. Therefore the tooth is extracted (Fig.3). The socket is single. After debridement, bone graft (Fig.5 *) and collagen membrane (Fig.4) are placed.
The patient will return for implant placement 2.5 months post extraction. He must be a gagger, because PAs in Fig.2,5 are taken with sensor 1. The Inferior Alveolar Nerve is out of view. It appears that he is too busy to have CBCT taken in the other office.
To prevent nerve injury, a PA should be taken prior to implant placement, preferably using sensor 2. If bone density in the socket increases, a shorter implant can be used. Prepare implant positioners, which will be used to determine whether a tissue punch will remove too much keratinized gingiva or not. If the gingiva over the original socket is thin, #15 scalpel will be used to make a short mesiodistal straight incision (~10 mm for 6 mm diameter implant for example). Most importantly, try not to use drills. If there is need to use them, confine the drills within the original socket. It is possible to use taps to finish osteotomy (1, 2).
Return to Lower Molar Immediate Implant,
Systemic Disease
Xin Wei, DDS, PhD, MS 1st edition 12/07/2014, last revision 03/11/2015