|
|
|
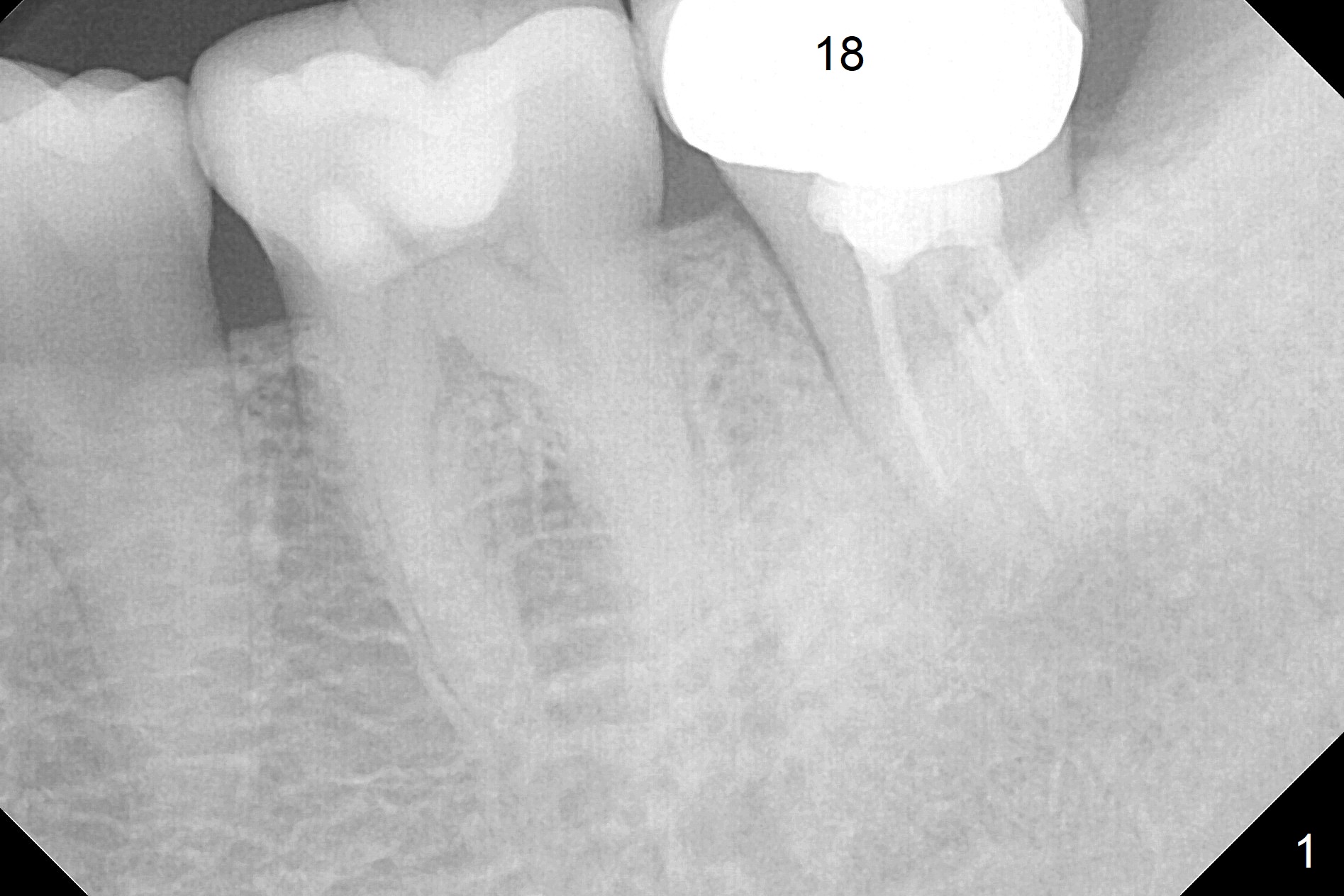
Fistula after RCT with Several Canals
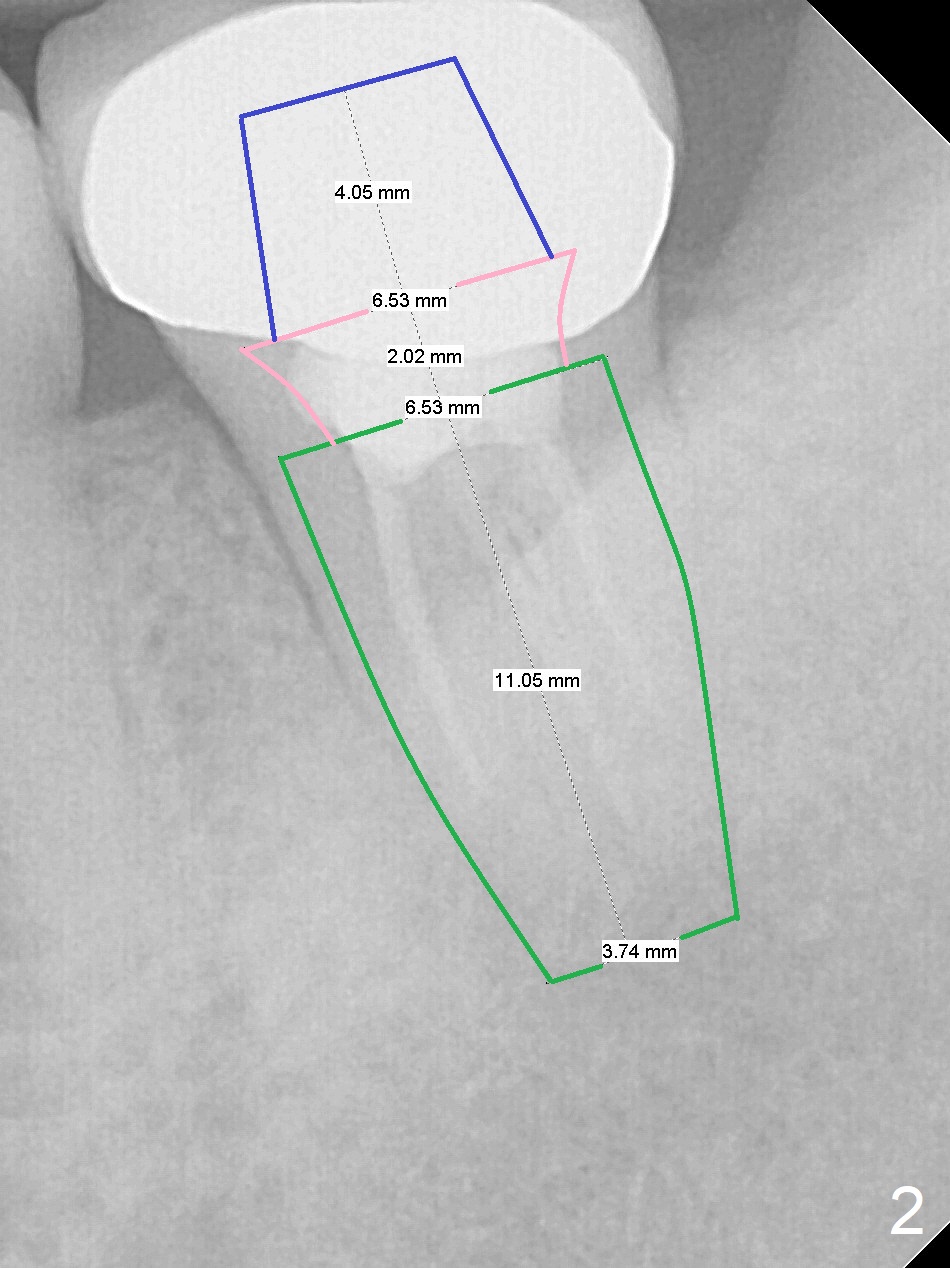
A 32-year-old woman has a buccal fistula after RCT (Fig.1). She would like to have extraction and implant to eradicate the lesion. In addition, there appear to be several canals which need to be retreated. Since the Inferior Alveolar Canal (IAC) is indistinct, osteotomy and implant placement will be confined 1-2 mm beyond the socket after debridement (Fig.2). Take the 1st intraop PA as early as possible (after use of 2 mm Bicon drill with extension and insertion of marked parallel pin). Osteotomy is buccal (if the buccal plate defect is not severe), as the IAC is lingual at this site. Also consider initiate osteotomy in the mesial slope of the socket. Prepare Sinus Master Kit for possible use of its short stoppers (2-6 mm).
Return to Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), IBS, Clindamycin Xin Wei, DDS, PhD, MS 1st edition 07/12/2017, last revision 08/20/2019