
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
How to Change Osteotomy Trajectory and Position
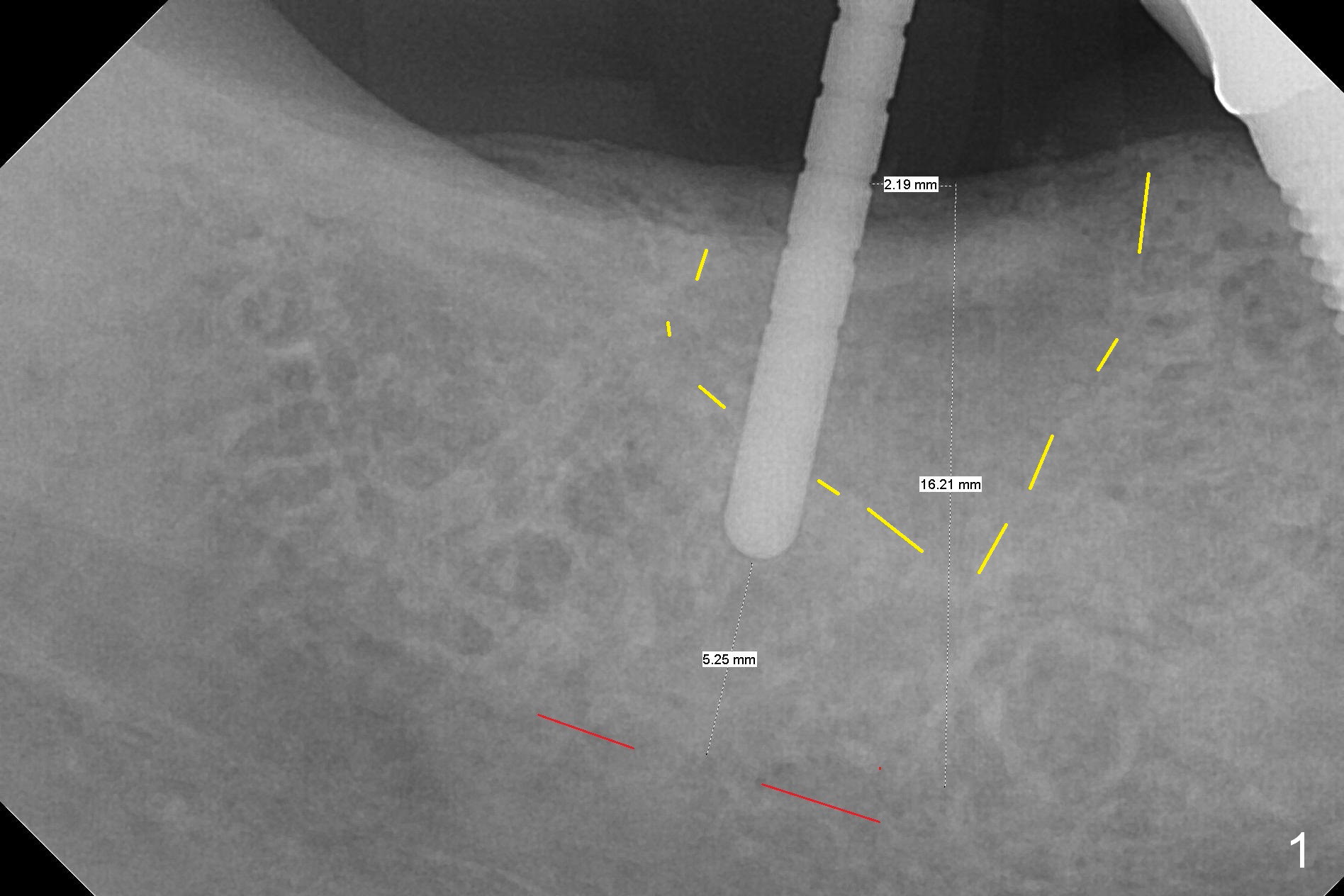
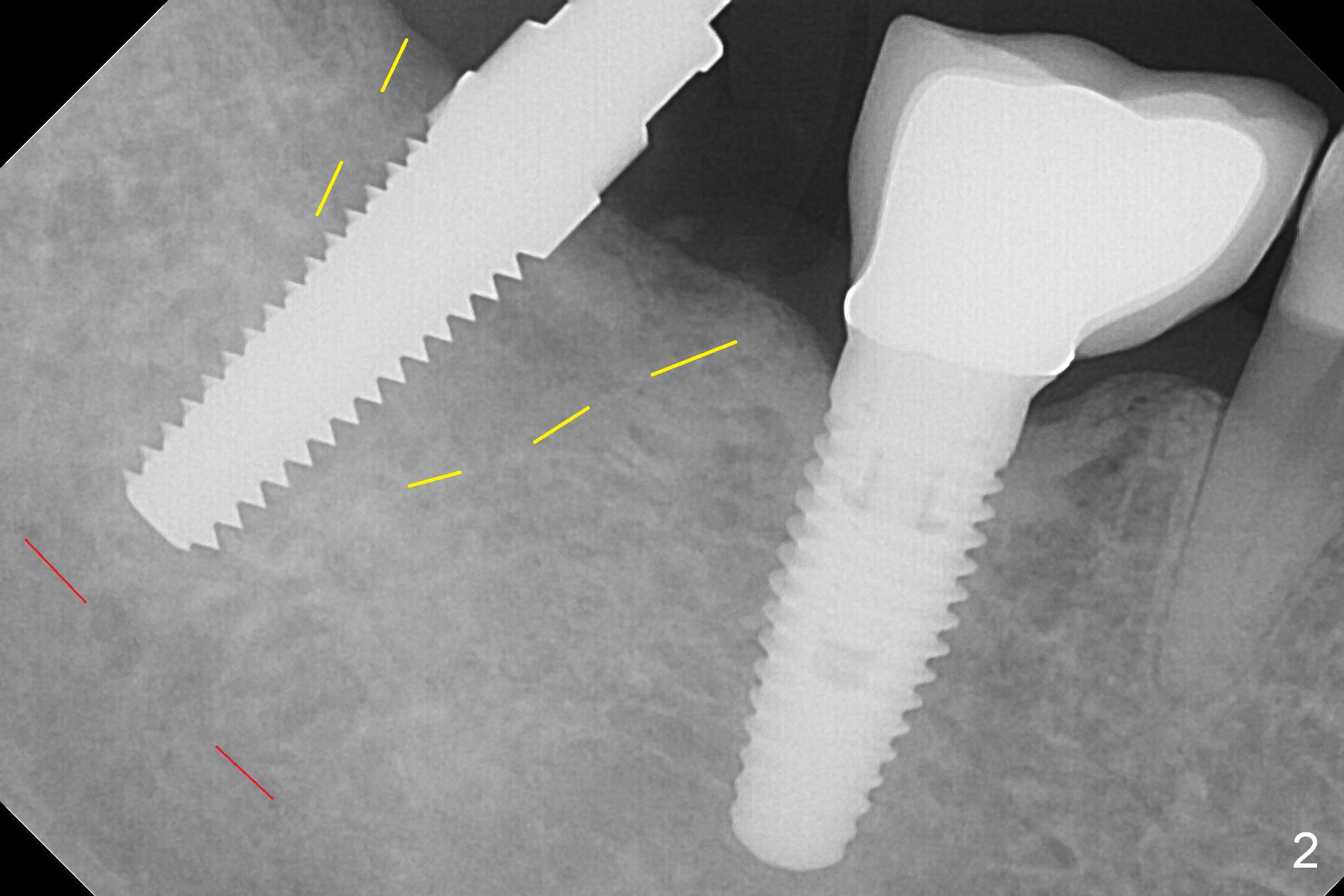
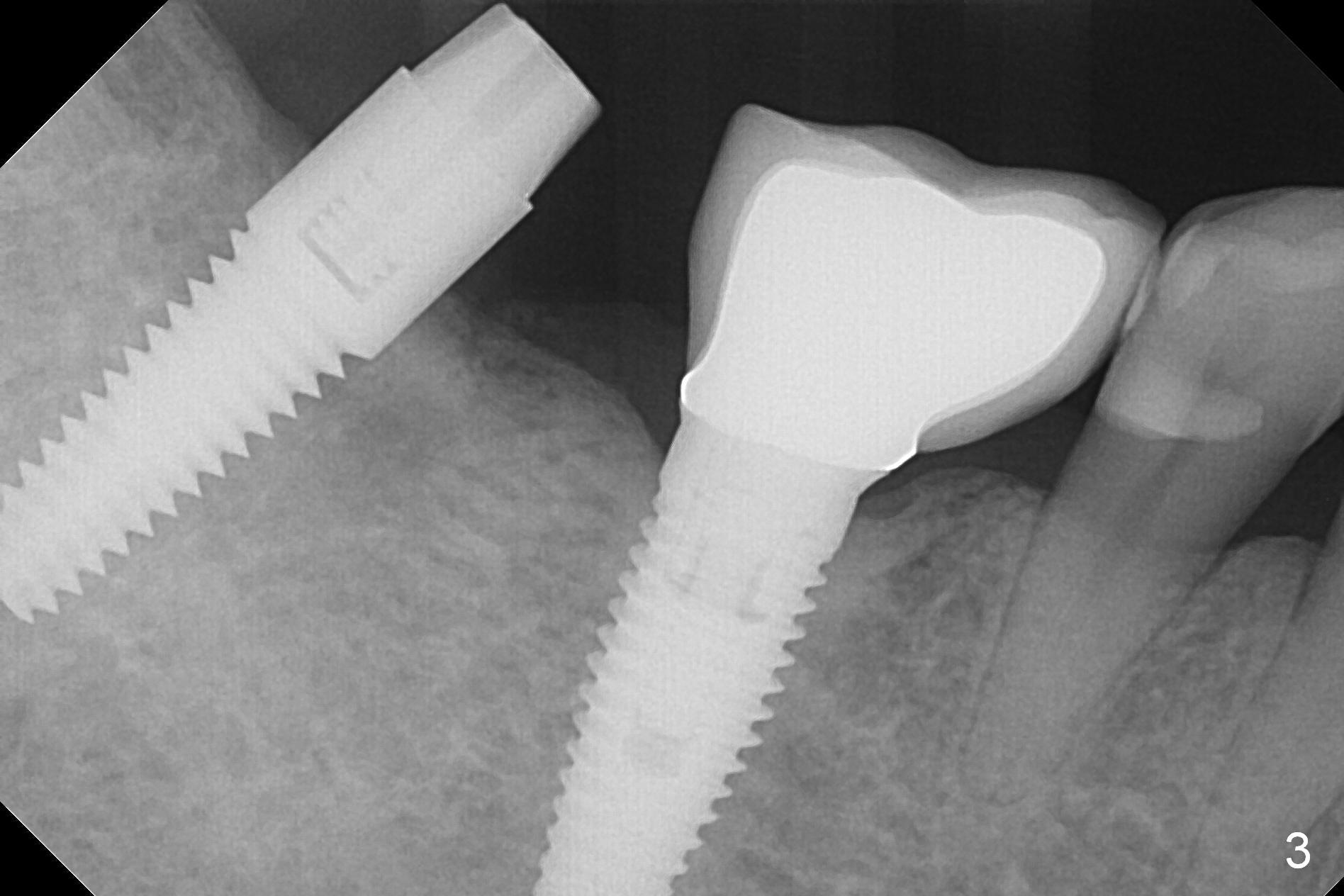
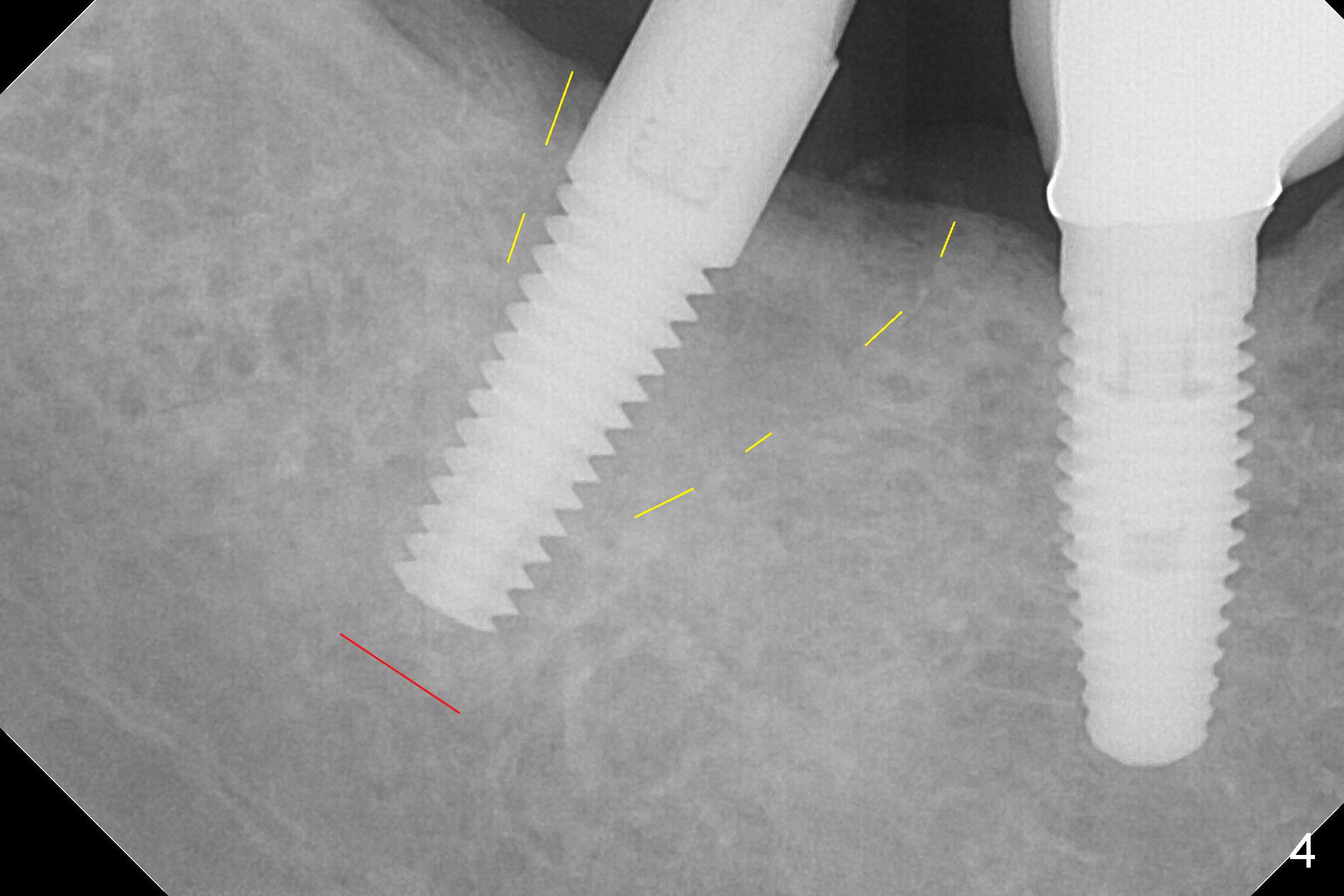
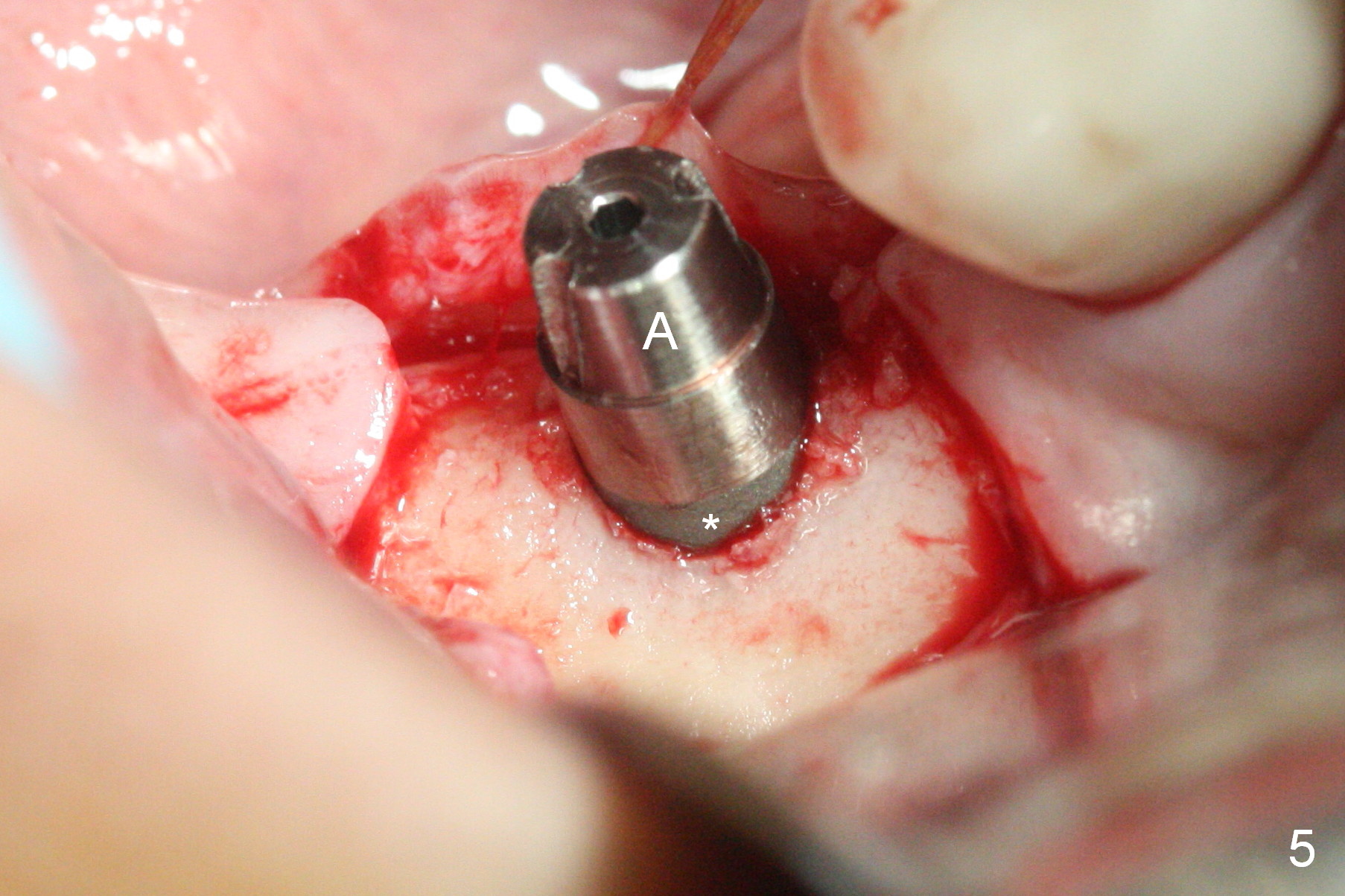
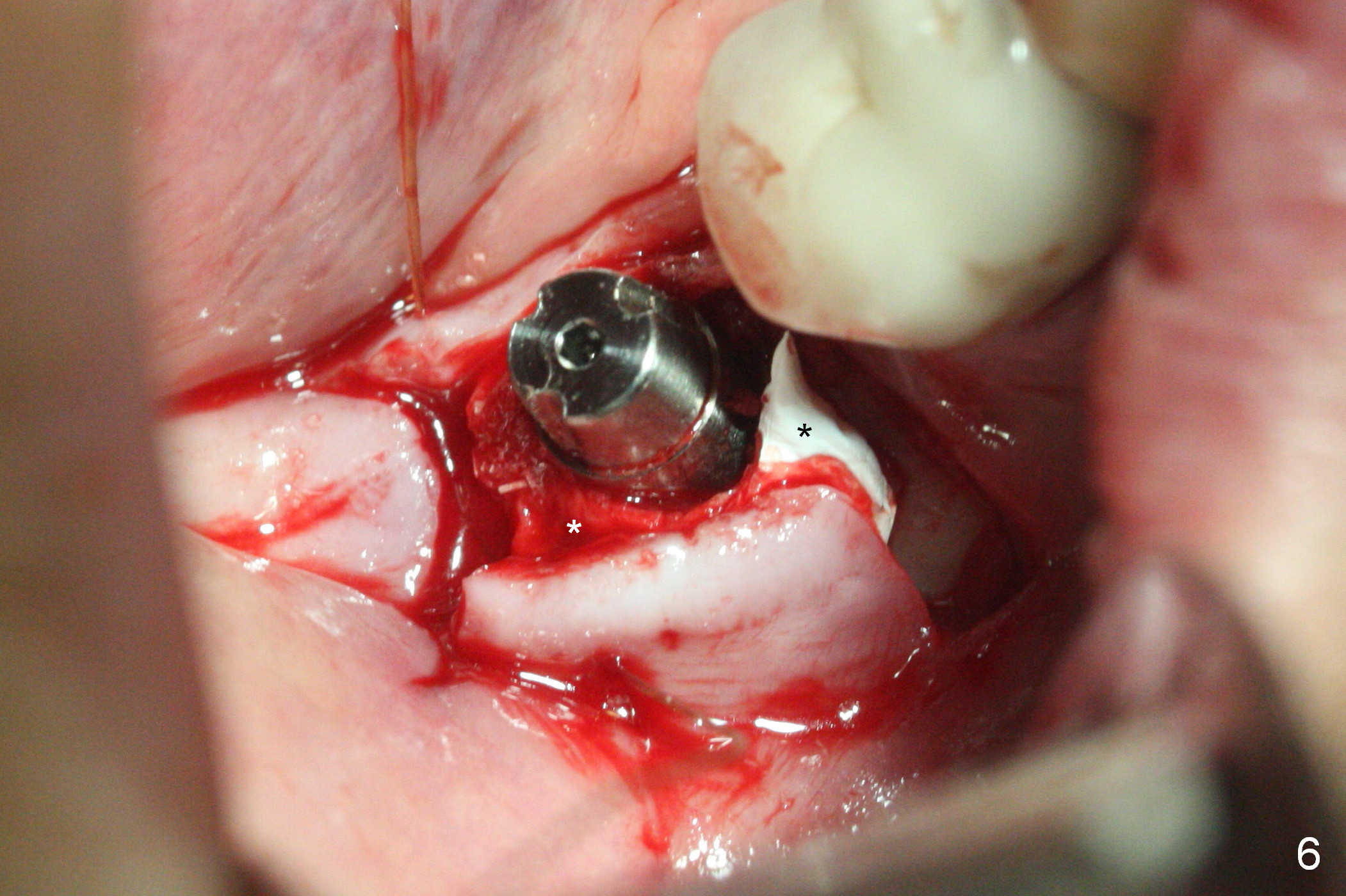
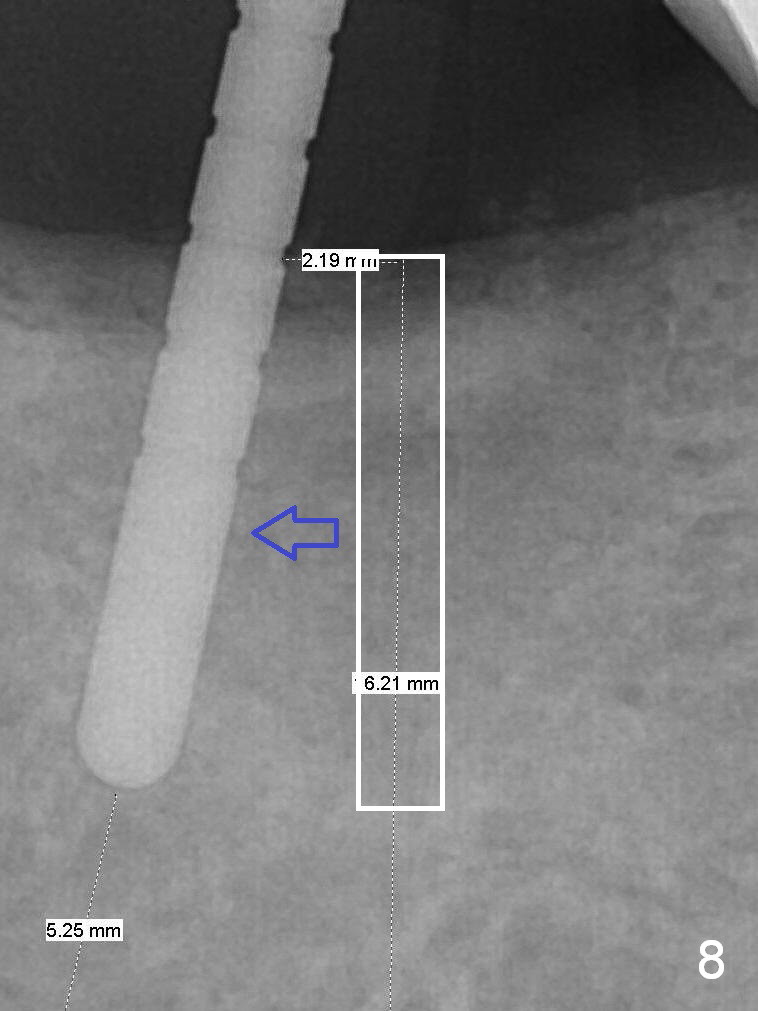
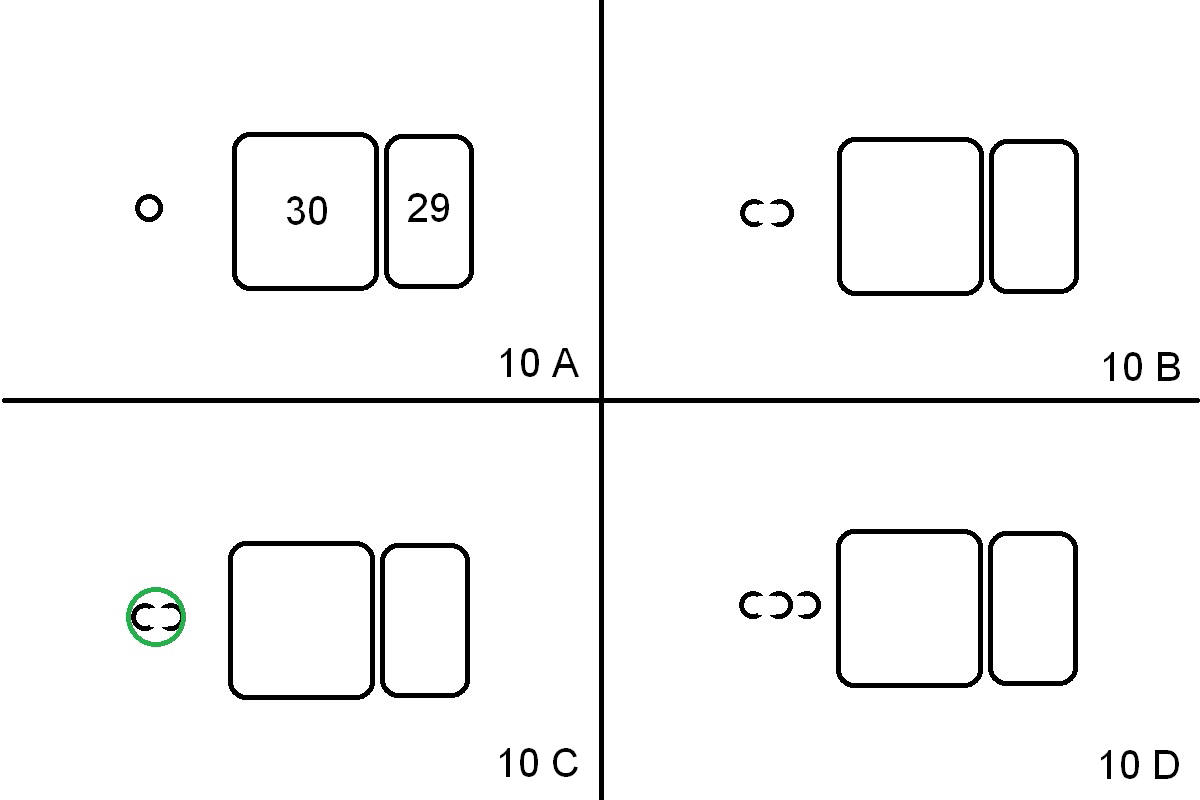
Initial osteotomy at the site of #31 using 2 mm pilot drill for 11 mm appears to be distal by 2-3 mm (Fig.1, Fig.10 A (circle, occlusal view of the edentulous and dentate (#29 and 30) areas)). Lindamann bur is used to move the osteotomy (Fig.8 white rectangle, Fig.10 B). It seems that the osteotomy returns distal as the osteotomy increases (Fig.2 (5x17 mm tap), Fig.8 arrow, Fig.10 C (green circle)). It appears to be late to change; a 5x17 mm tissue-level implant is placed with > 60 Ncm (Fig.3-5). The buccal and lingual rough surface of the implant (Fig.5 *) is covered by autogenous bone/Osteogen and Collagen Dressing (Fig.6 *). After suturing (Fig.7), periodontal dressing is applied around the abutment (Fig.5 A (4.5x3 mm)).
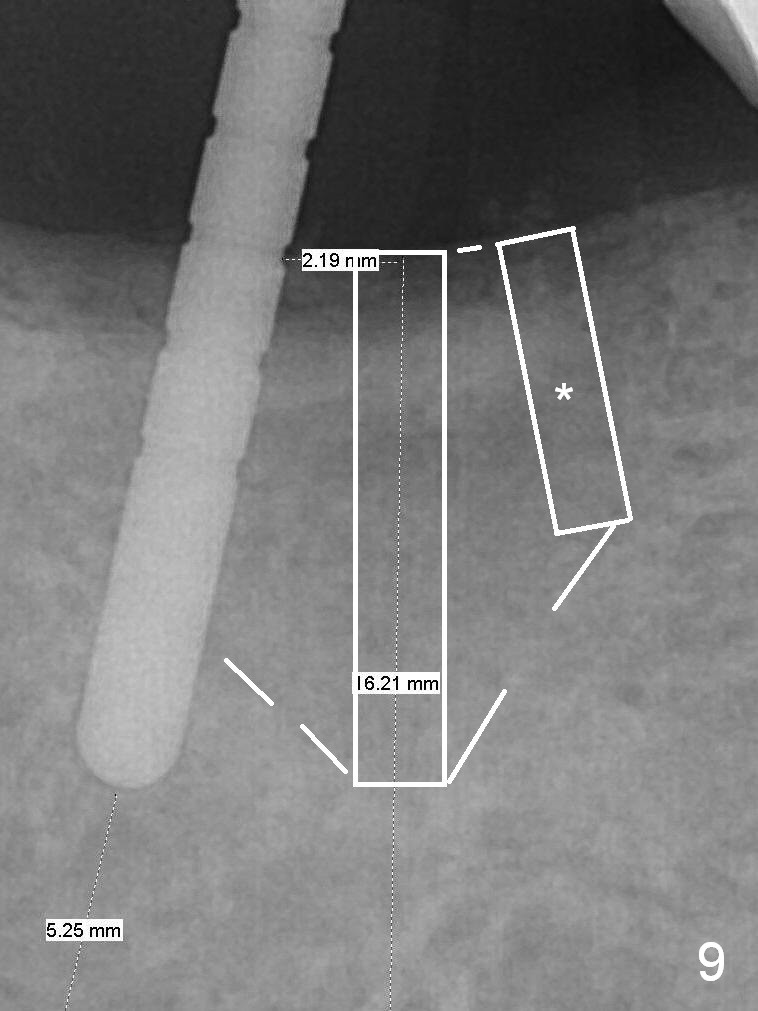
To change osteotomy trajectory and position correctly, it should be overcorrected (Fig.9 white rectangle with *, Fig.10 D).
The patient will return for provisional >`1 month postop with chief complaint "the implant is too high". The 2nd and 3rd options are to place healing screw and healing abutment.
Return to
Lower
Molar Immediate Implant, IBS,
Improvement
Xin Wei, DDS, PhD, MS 1st edition 12/12/2016, last revision 01/12/2017