
|
|
|
|
|
|
|
|
|
How to Prevent Paresthesia Associated with Immediate Implant in the Lower 2nd Molar?
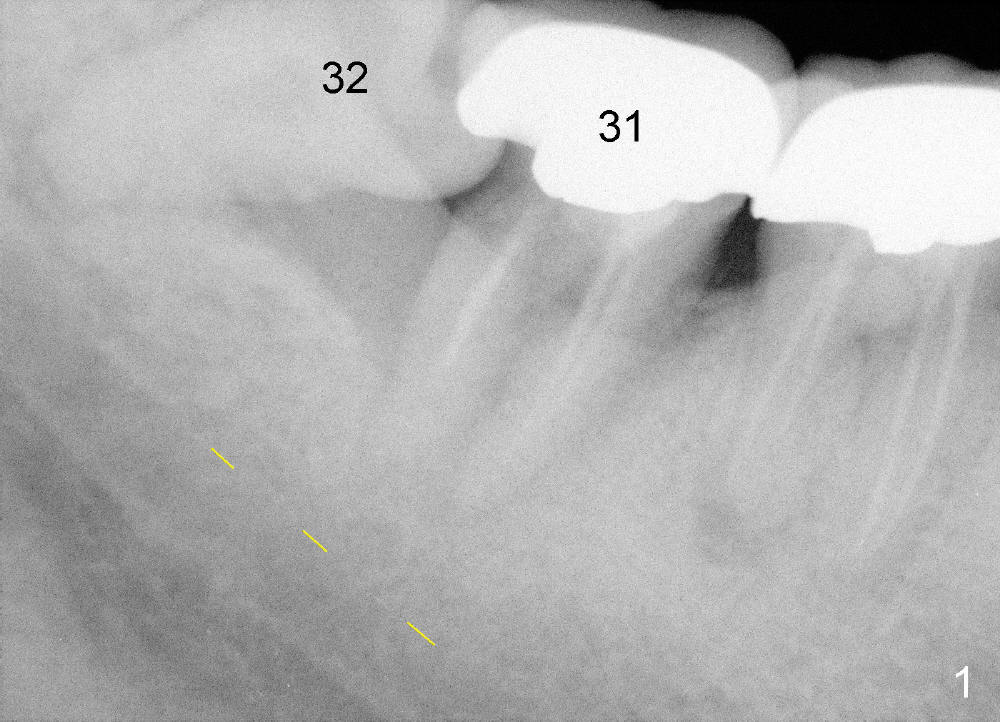
The lower right 2nd and 3rd molars are nonsalvageable for a 51-year-old lady (Fig.1). An immediate implant is to be placed at the site of #31. There is no acute infection. Anesthesia should be easily obtained with infiltration. If pain is associated with osteotomy, the drill must be close to the inferior alveolar nerve (yellow dashed line: upper border of the inferior alveolar canal). If the pain is not controlled, the procedure will be changed to socket preservation without any hesitation.
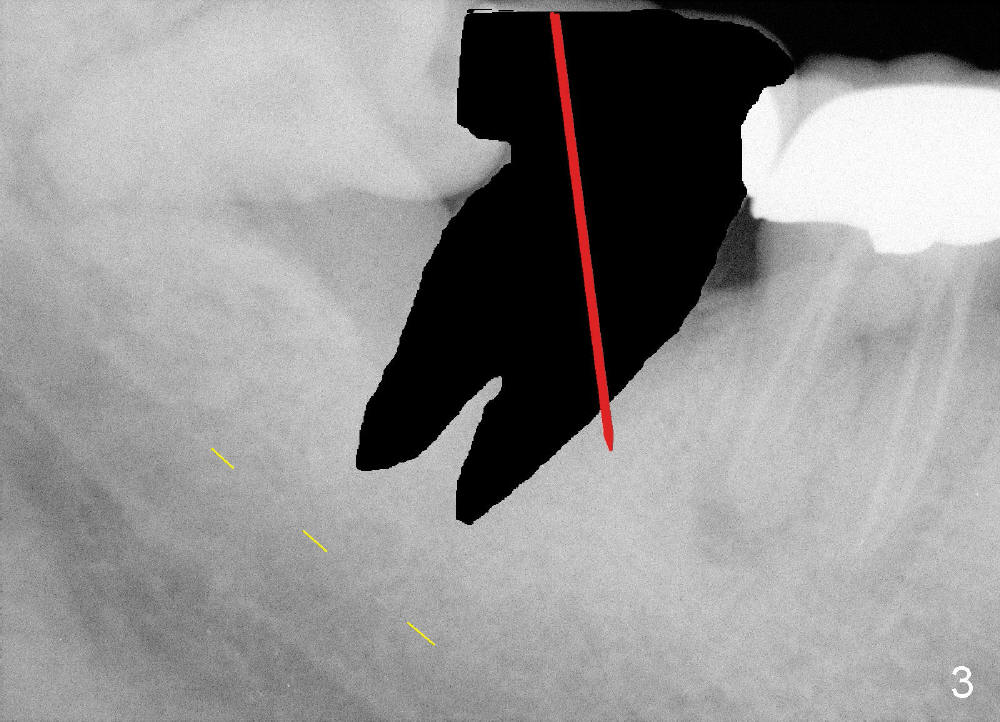
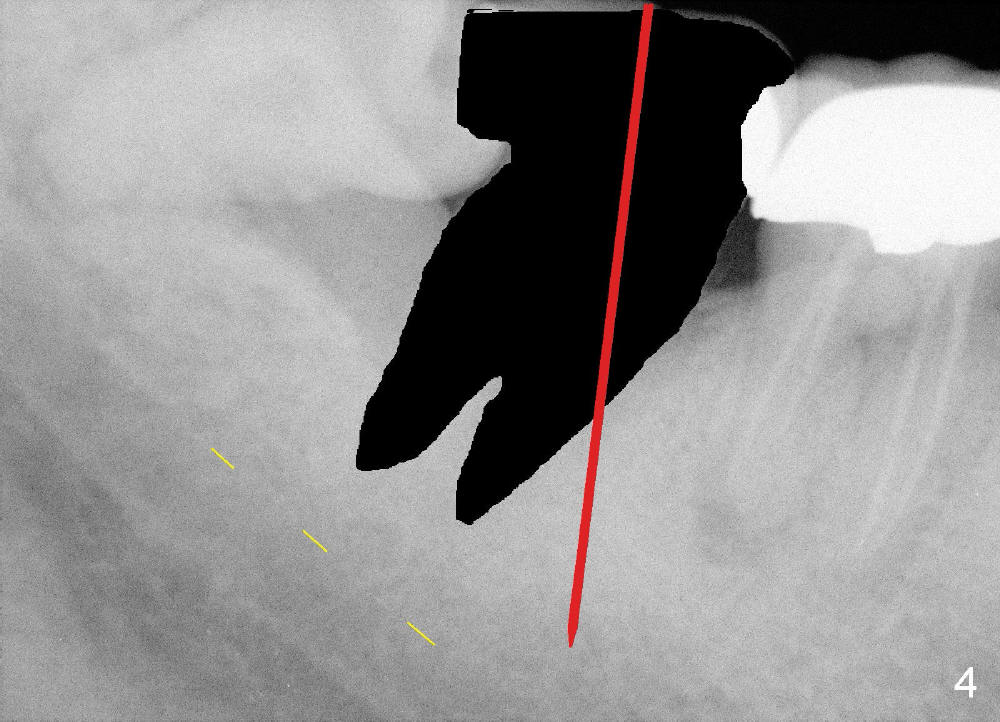
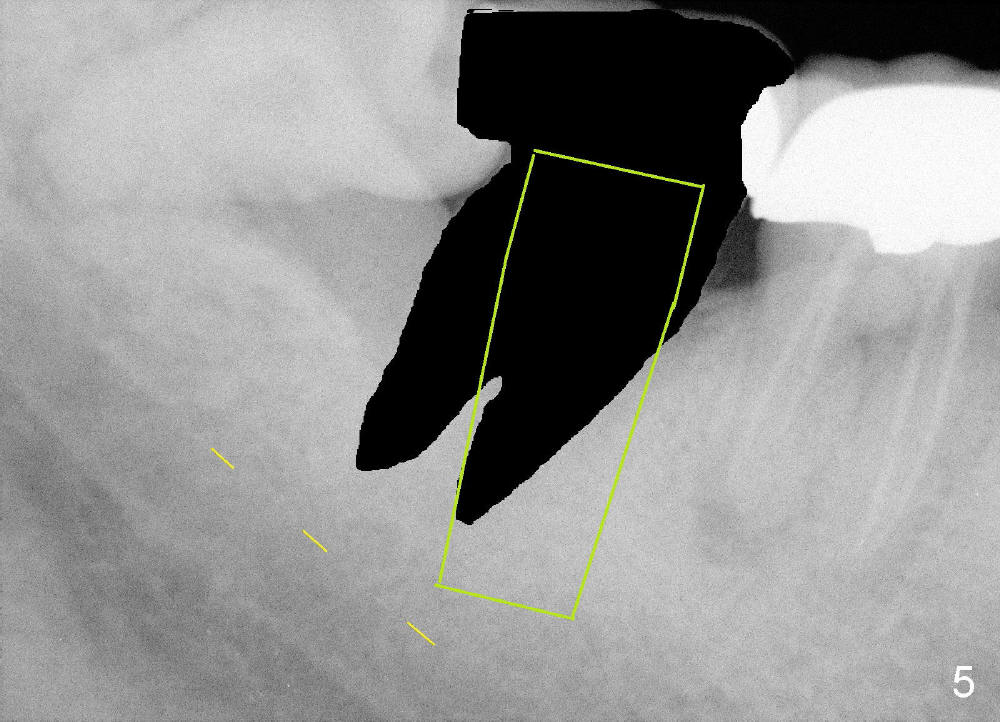
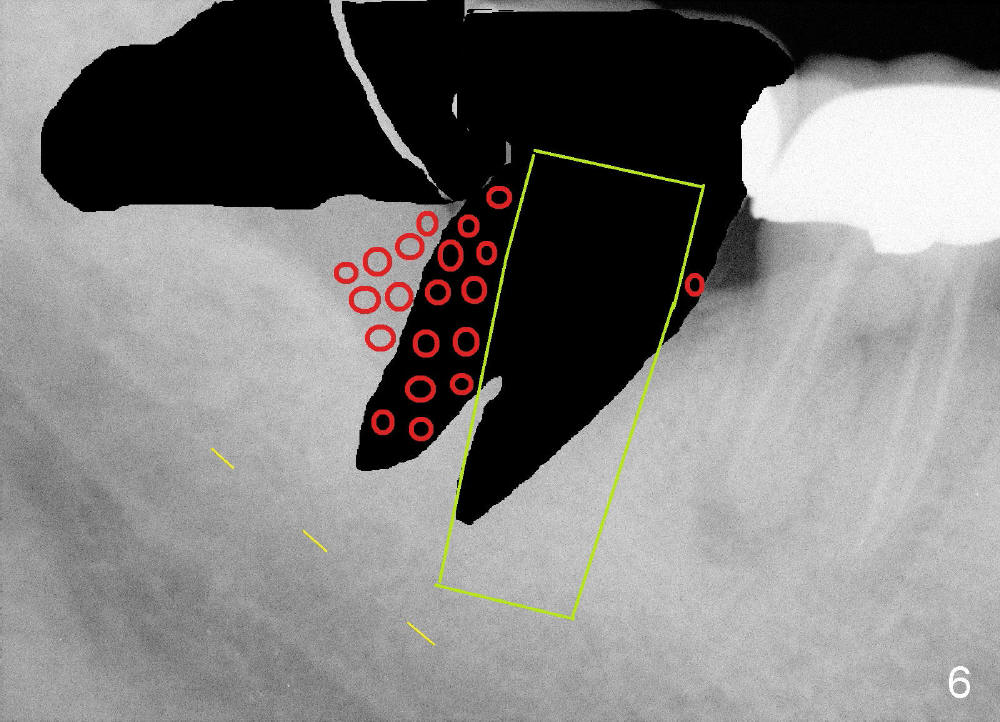
To keep reliable landmarks for osteotomy, the tooth #31 will be extracted first (Fig.2; sectioning to protect the septal bone). Osteotomy is initiated in the mesial slope of the socket, with a pilot drill leaned on the 3rd molar (Fig.3). Once the pilot drill penetrates the lamina dura, the position of the upper end of the drill changes to the center of the edentulous area (Fig.4), while the depth is increased with caution. When the implant is placed (Fig.5), the tooth #32 is extracted (Fig.6) and bone graft (red circles) is placed to cover exposed threads of the implant.
Return to Lower Molar Immediate Implant,
Periimplantitis
Xin Wei, DDS, PhD, MS 1st edition 09/25/2014, last revision 02/13/2016