



|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Socket Bone Injection for Pain Control
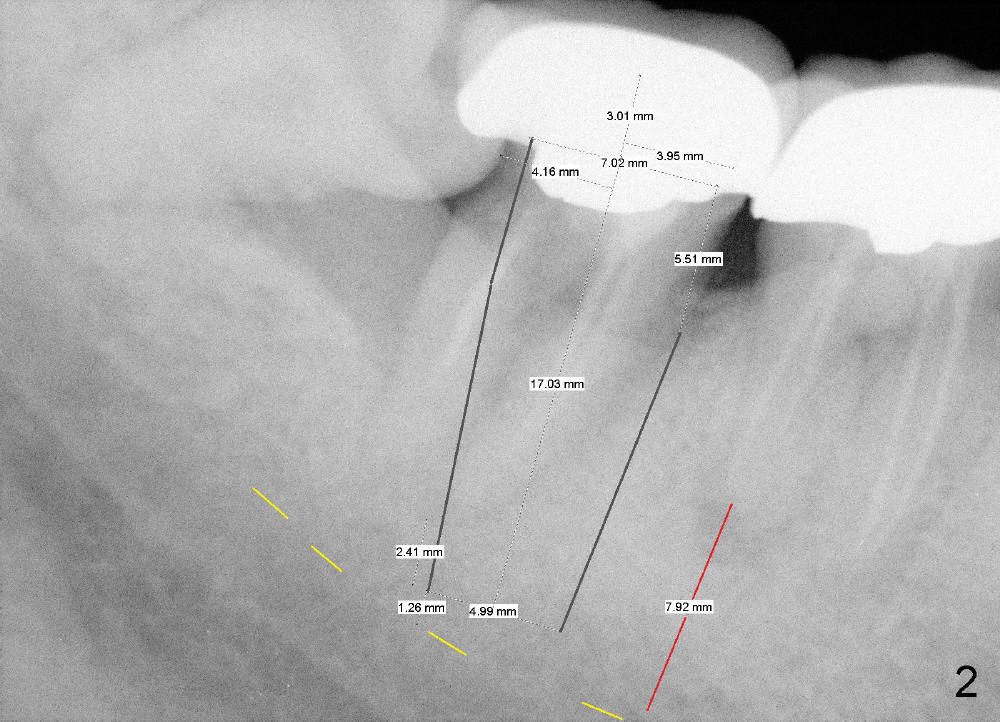
Although there is no infection around the tooth #31 (Fig.1), there are multiple deep pockets. Infiltration is administered first. Extraction reveals that the distal root is fractured from #31.
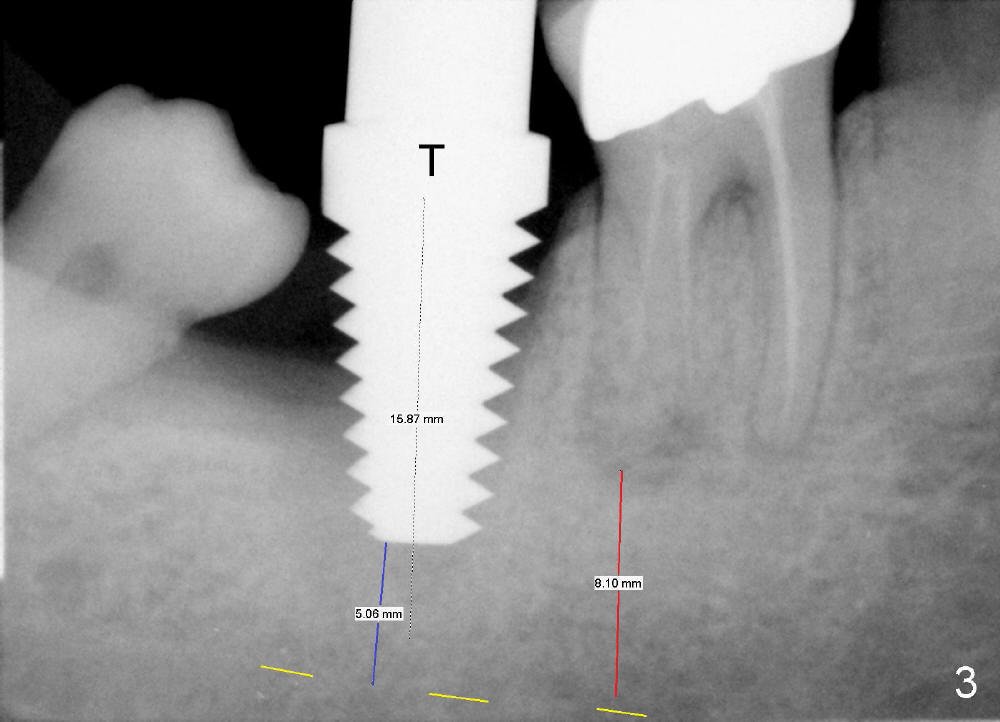
Without drilling, taps do not engage into the socket (Fig.3). This PA does not show the lower border of the inferior alveolar canal (IAC) completely. The upper border of IAC (yellow dashed line) is referred by the distance from the distal apex of #30 of Fig.2 (preop PA). It appears that there is about 5 mm from the bottom of the tap to the upper border of IAC.
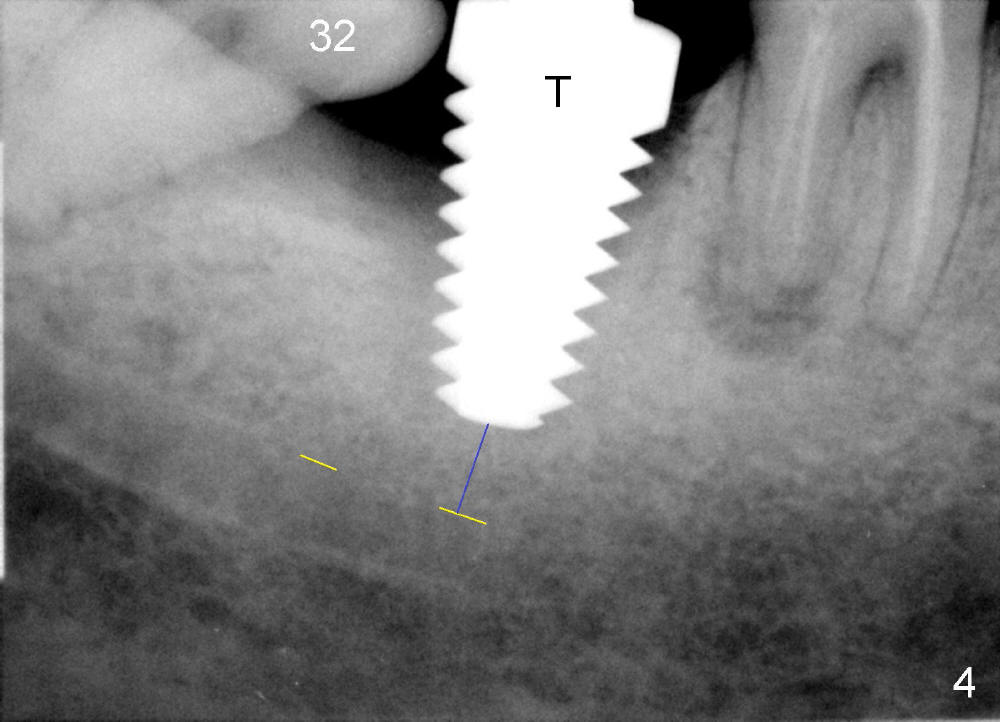
The bottom of the socket is sensitive. For safety, block anesthesia is not attempted at this moment. Instead, local anesthetic (2% Lidocaine with 1:100,000 Epinephrine) is injected into the socket bone without leakage (30 gauge needle). It works! The patient allows us to finish osteotomy 2-3 mm deep into new bone (2 mm pilot drill, 2.5-4.0 mm reamers) with minimal pain. Finally a 8x17 mm tap is able to bind to the socket (Fig.4).
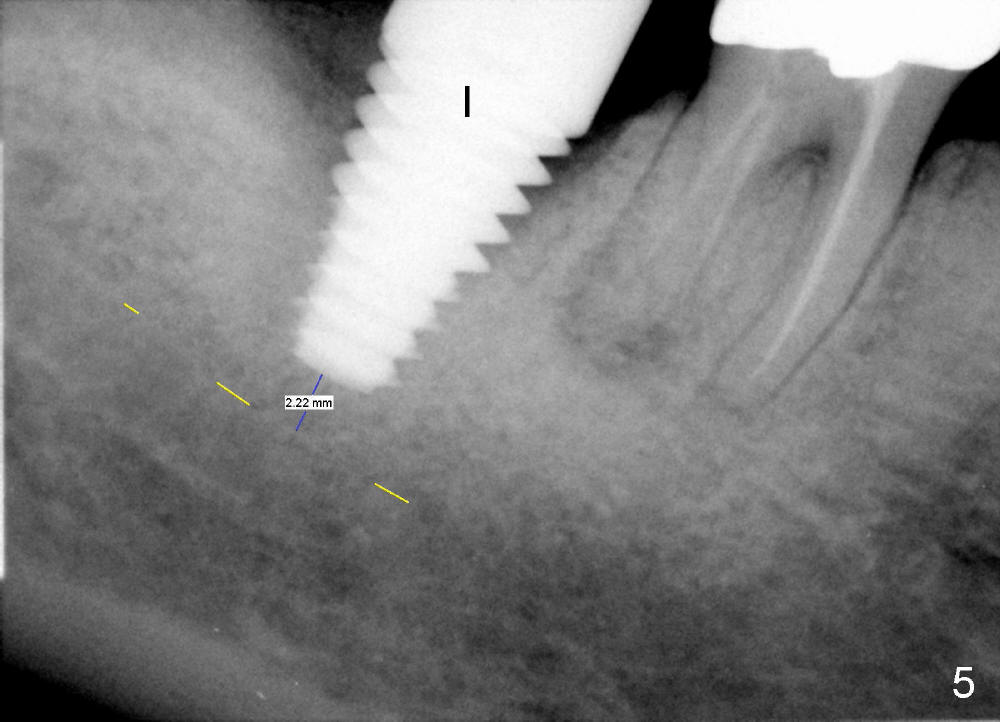
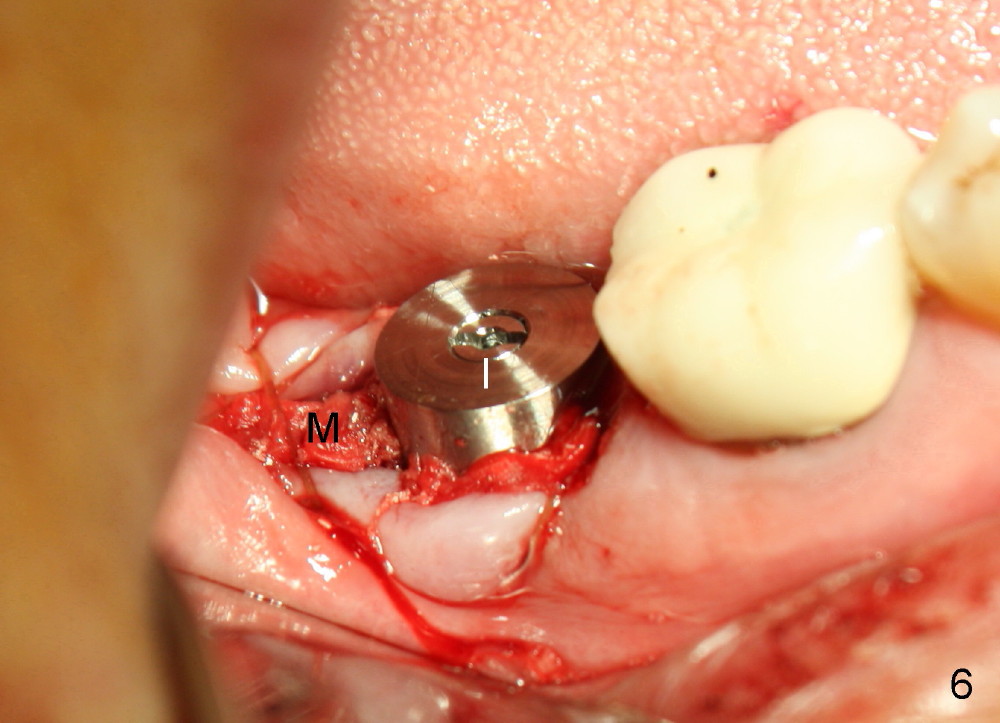
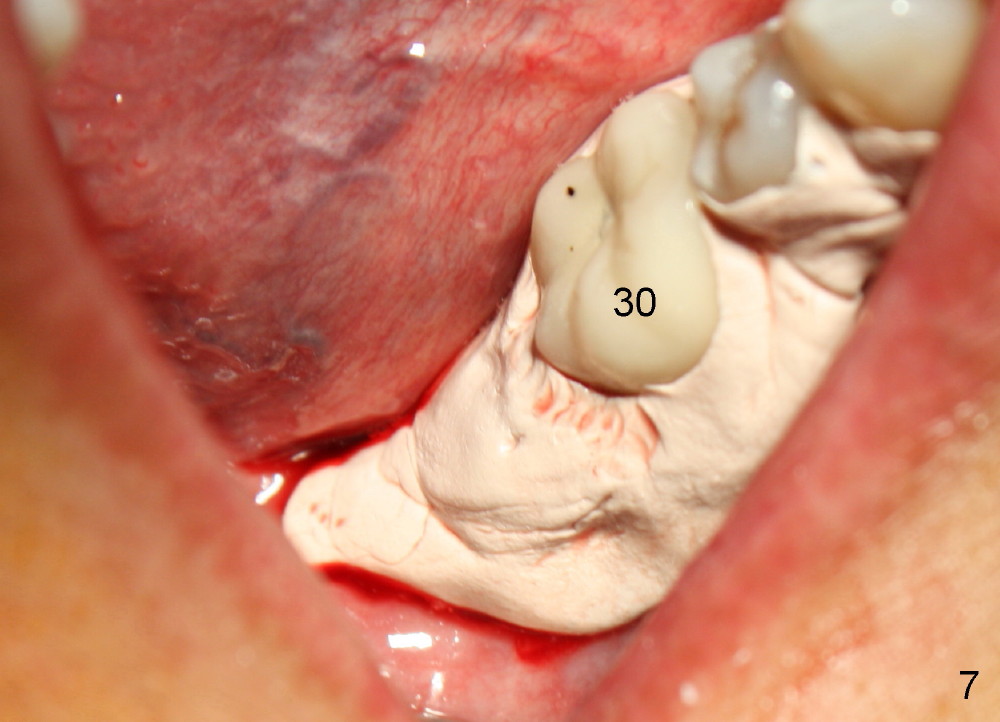
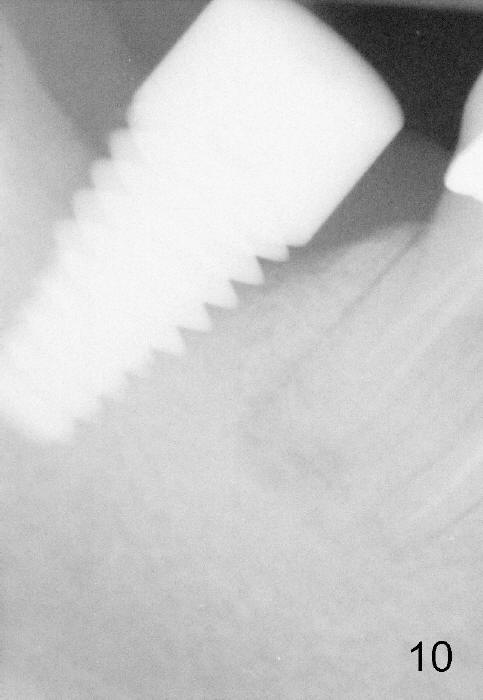
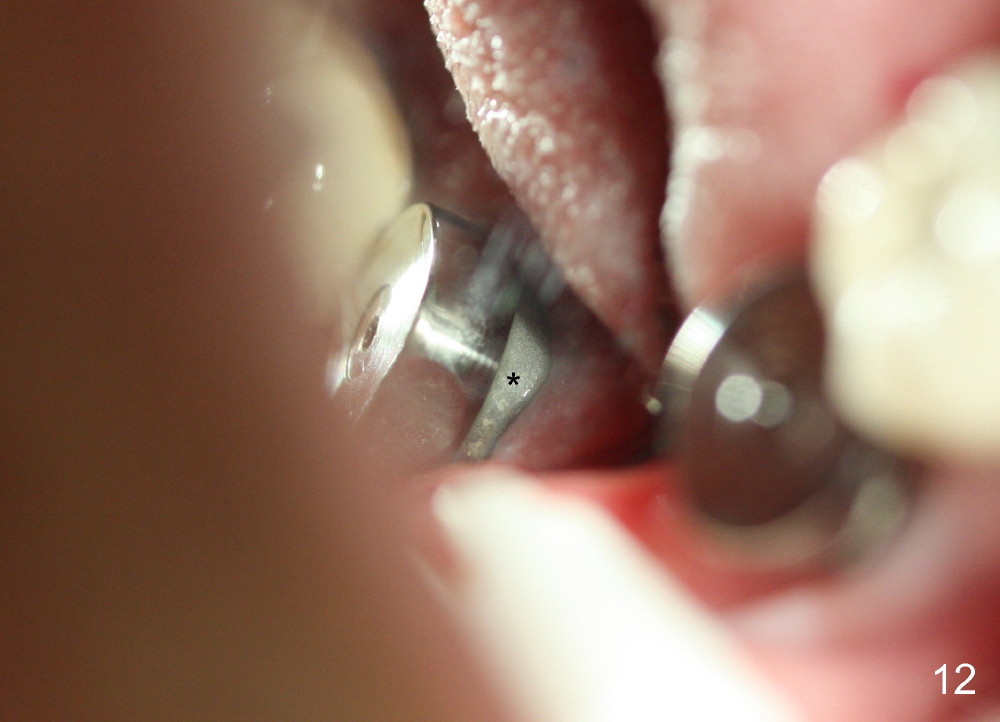
After the tooth #32 is extracted with intraligamental injection, a 8x17 mm tissue level implant is being placed. Block anesthesia has to be administered to finish the placement with insertion torque > 60 Ncm without pinching IAC (Fig.5). Collagen plug is placed in #32 socket, while allograft and Synthetic bone mixture is placed around the implant (mainly distally). Collagen membrane is placed on the top of the graft, sutures are placed (Fig.6). The wound is covered by perio dressing (Fig.7). The perio dressing is dislodged partially 8 days postop; when it is removed in the office, the gingiva heals around the implant except distal (Fig.8 *). Two months postop, bone appears to have approached the upper threads of the implants (Fig.9,10, compare to Fig.5). The implant remains stable. The rough surface of the implant is exposed distobuccally (Fig.11 *) and distally (Fig.12 *). Ultimately bone graft is required to cover the exposed threads.
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 09/30/2014, last revision 03/20/2015