



|
|
|
|
|
|
|
|
|
|
|
Challenges of Placing Implant at Lower 2nd Molar
There are several challenges to place implant at the lower 2nd molar: difficult access, gag reflex, blurred X-ray image and close to the inferior alveolar nerve (IAN). How close is it? How can we avoid injury to IAN?
A 62-year-old lady has an advanced endo-perio disease associated with the tooth #31 (Fig.1). IAN is not distinct in the preop PA. IAN is assumed far away from implant area. The implant is planned to be placed along the long axis of the tooth for the best restorative result (Fig.2). The tissue-level implant is placed ~ 3 mm above the distal crest so that implant threads may be less likely exposed postop. Is it a good treatment plan?
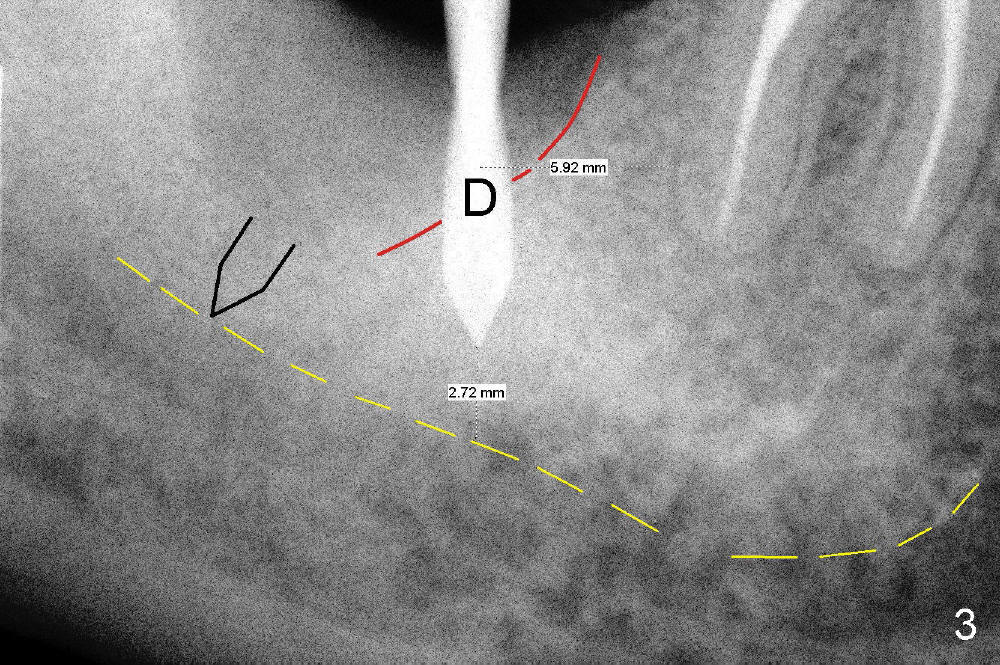
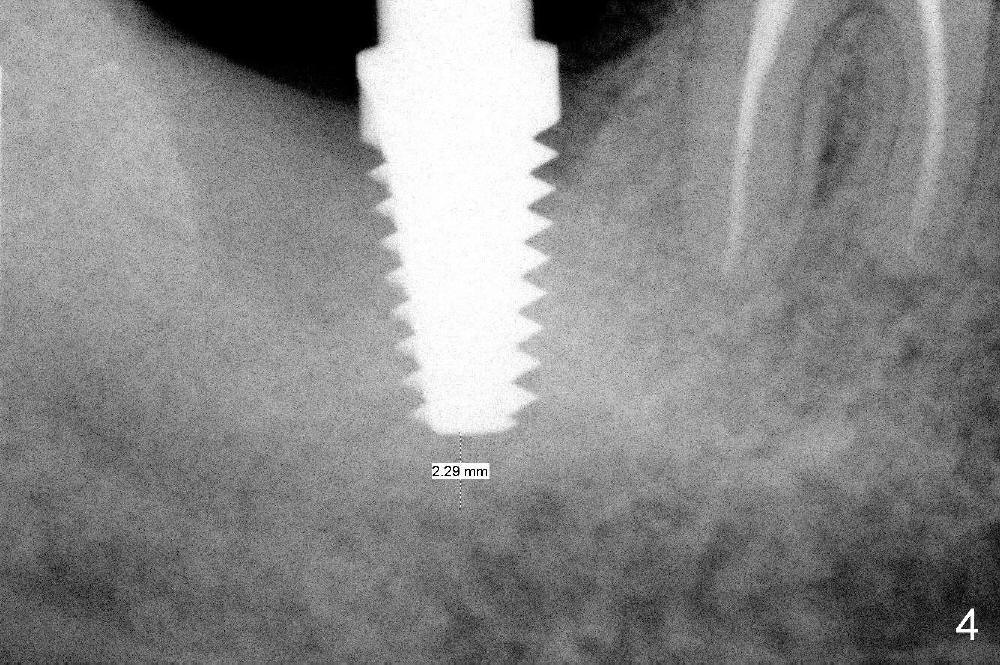
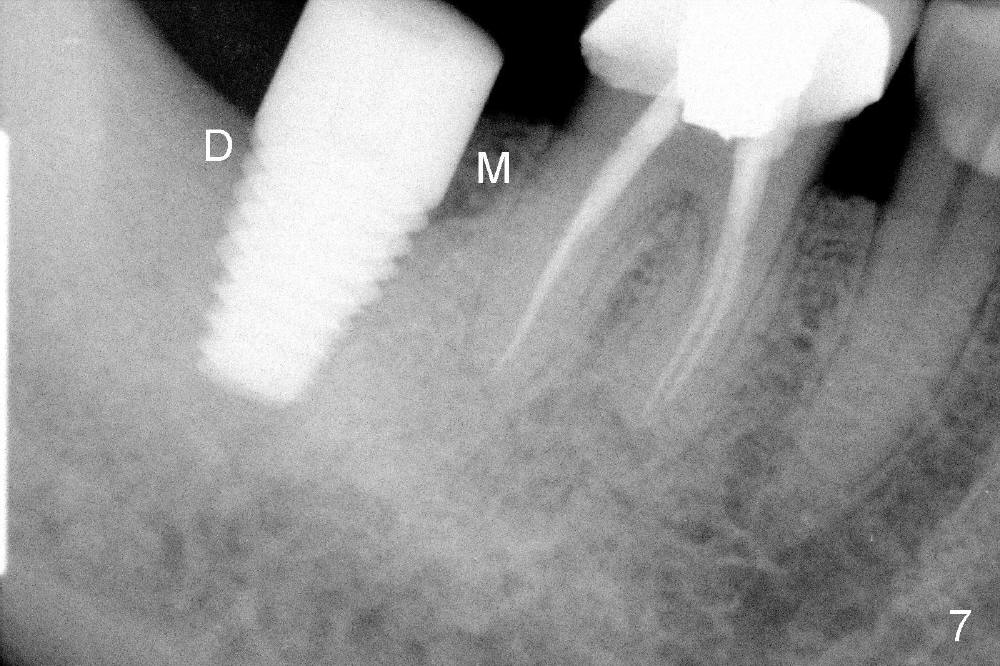
No. First at all, CT should be taken when 2D image does not show IAN. Fortunately, the surgery happens to be executed better than the plan. Clindamycin is used for socket soaking for 5 minutes. The initial osteotomy should be not exceeded 6 mm from the distal surface of the first molar (Fig.3: 5.92 mm). The 2 mm pilot drill (D) penetrates the mesial slope of the socket (red line) for 3-4 mm. There is 2.72 mm from IAN (yellow line: upper border of IAN canal). If the implant is placed along the long axis of the tooth, the initial osteotomy should start at the apex of the socket. The same pilot drill (black outline) penetrates the nascent bone for the same distance (3-4 mm) for primary stability, IAN may be invaded! The patient is a severe gagger. She manages to allow us to take this PA (Fig.3) and the next one (Fig.4 with 6x14 mm tap in place, primary stability having been achieved). To close the socket, a 7x14 mm implant is placed. Immediately postop PA is taken twice without success. The socket is closed with 2 sutures and heals around the implant 8 days postop (Fig.5,6). PA is taken 2 months postop (Fig.7). The implant is not placed as deep as planned. It is stable without paresthesia of the lower lip. An abutment is placed (Fig.8: A) nearly 3.5 months postop.
The 2nd indication to take CT is gag reflex. Do not place an implant at the lower 2nd molar without seeing IAN, even intraop. If not sure, place a shorter implant as long as primary stability is achieved. To gain more bone, place the implant in the mesial slope of the socket, not in the center of the socket.
The last challenge to place implant at the lower 2nd molar will be found in the later stage of treatment.
Return to Lower Molar Immediate Implant, Periimplantitis
Xin Wei, DDS, PhD, MS 1st edition 02/04/2014, last revision 03/04/2018