|
|
|
|
|
|
|
|
Design is Precursor to Success of Immediate Implant
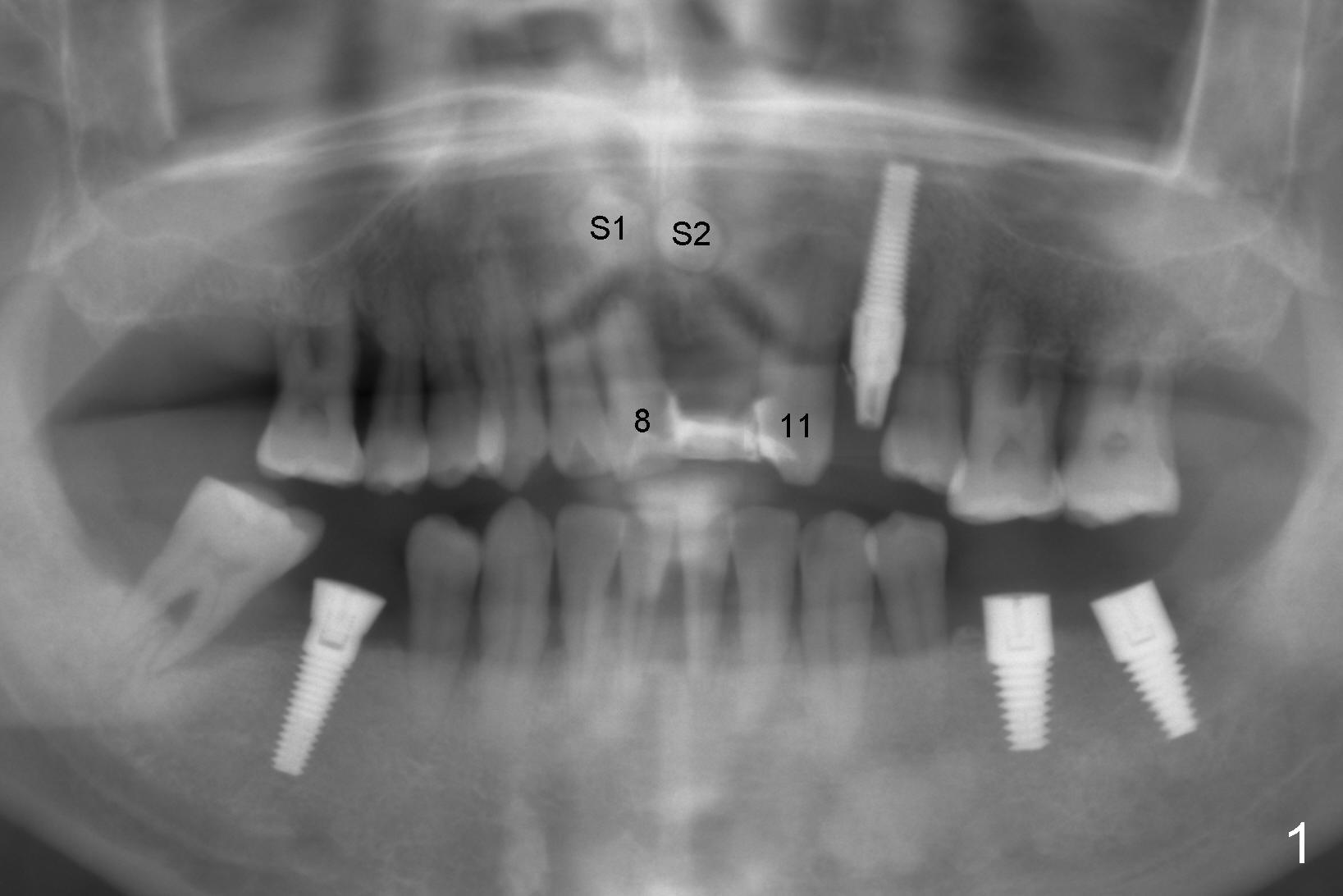
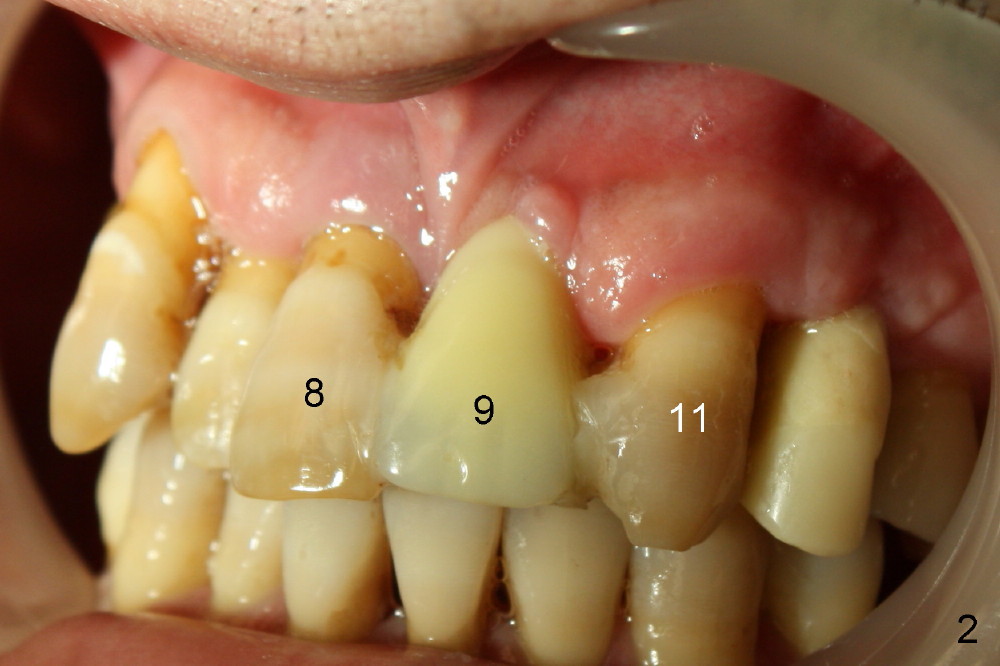
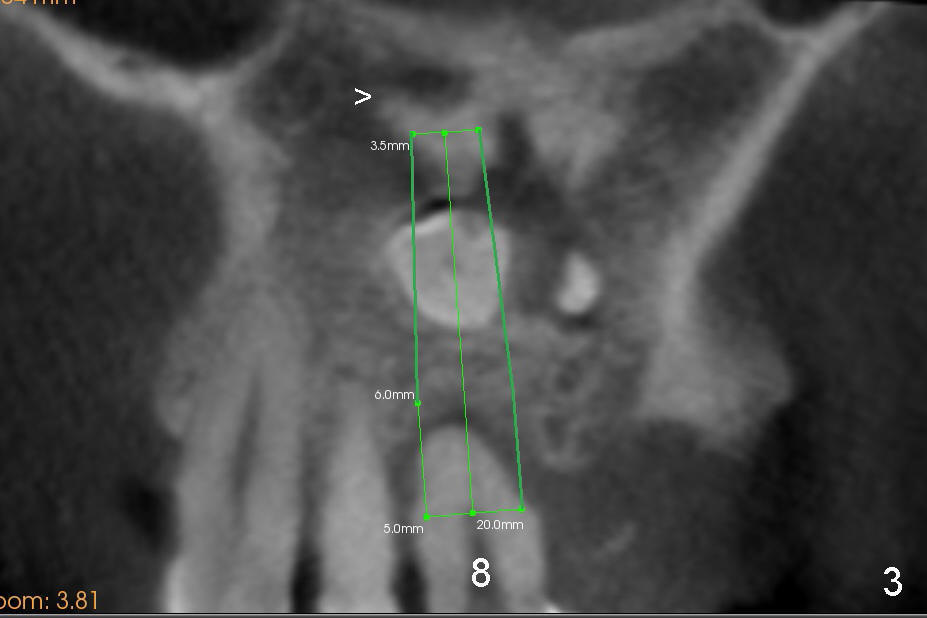
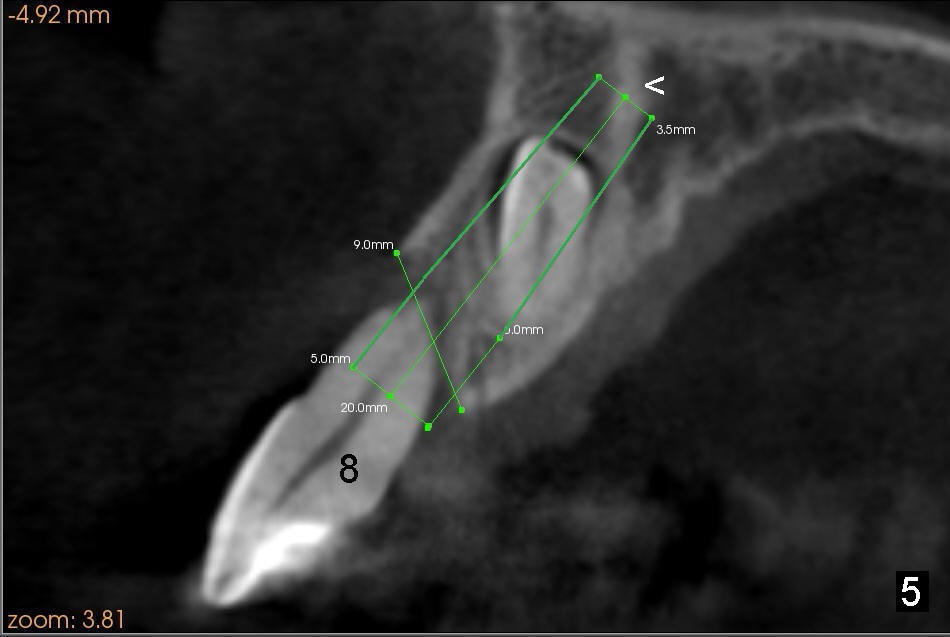
A 41-year-old man has poor dentition (Fig.1: #12 immediate provisional). It appears that #10 is congenitally missing. A temporary bridge is fabricated (Fig.1: #8-11) when #9 is reportedly extracted. Recently bonding between #9 pontic and #11 detaches. The bridge is loose (Fig.2). The tooth #8 is periodontally compromised (Fig.3,5: CT sagittal and coronal sections, respectively).
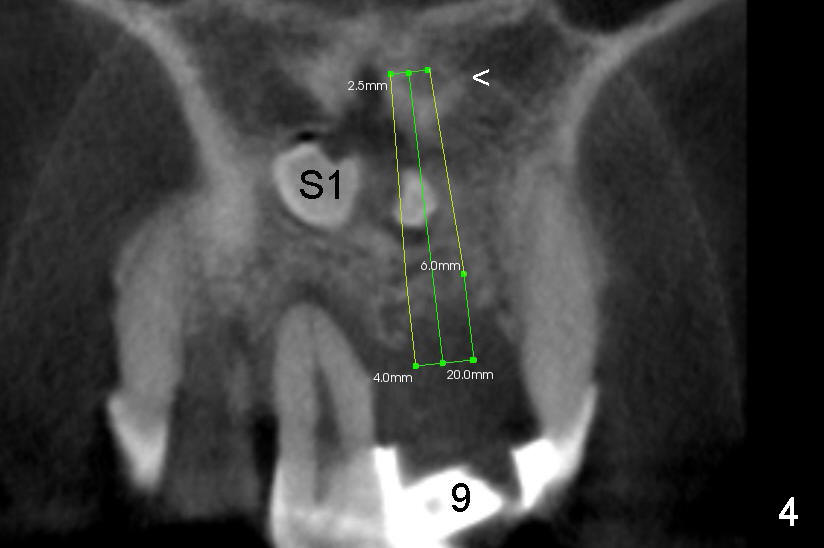
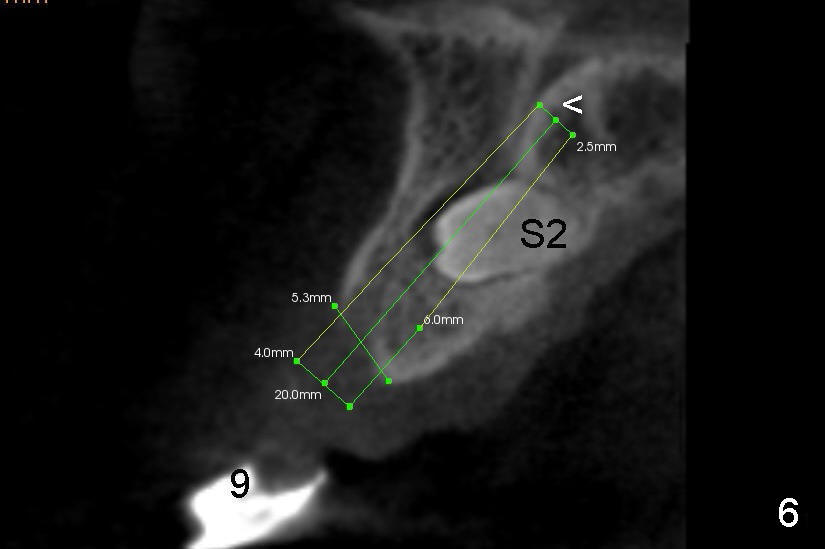
Treatment plan is to extract two supernumerary teeth (S1,S2) and #8, bone graft (mainly S1,2 sockets, and #8 buccal for cosmetics) and place immediate implants at the sites of #8 and 9. Long implants (20 mm) are to be used to engage into the two bone segments, coronal and apical to the S1,2 sockets (Fig.5,6). Since the bone segment apical S1,2 sockets is mainly cortical (arrowheads in Fig.3-6; lamina dura and nasopalatine canal), the two implants are expected to be stable. A palatal incision is going to be made to expose S1,2, as one of them (S2) is more or less palatal (Fig.6). Here is surgery.
Design and Preparation Xin Wei, DDS, PhD, MS 1st edition 01/05/2014, last revision 01/21/2019