|
|
|
|
|
|
|
|
|
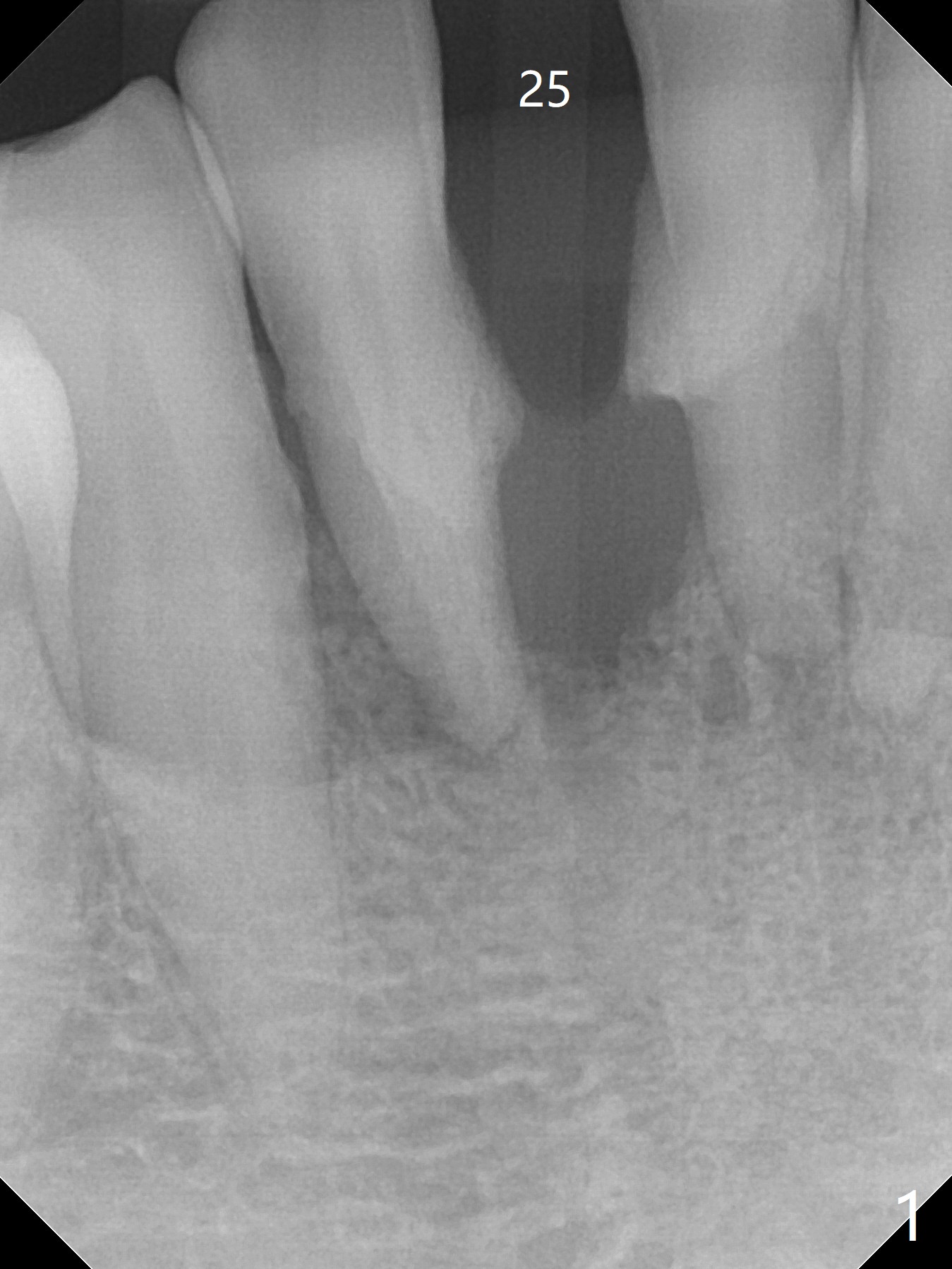
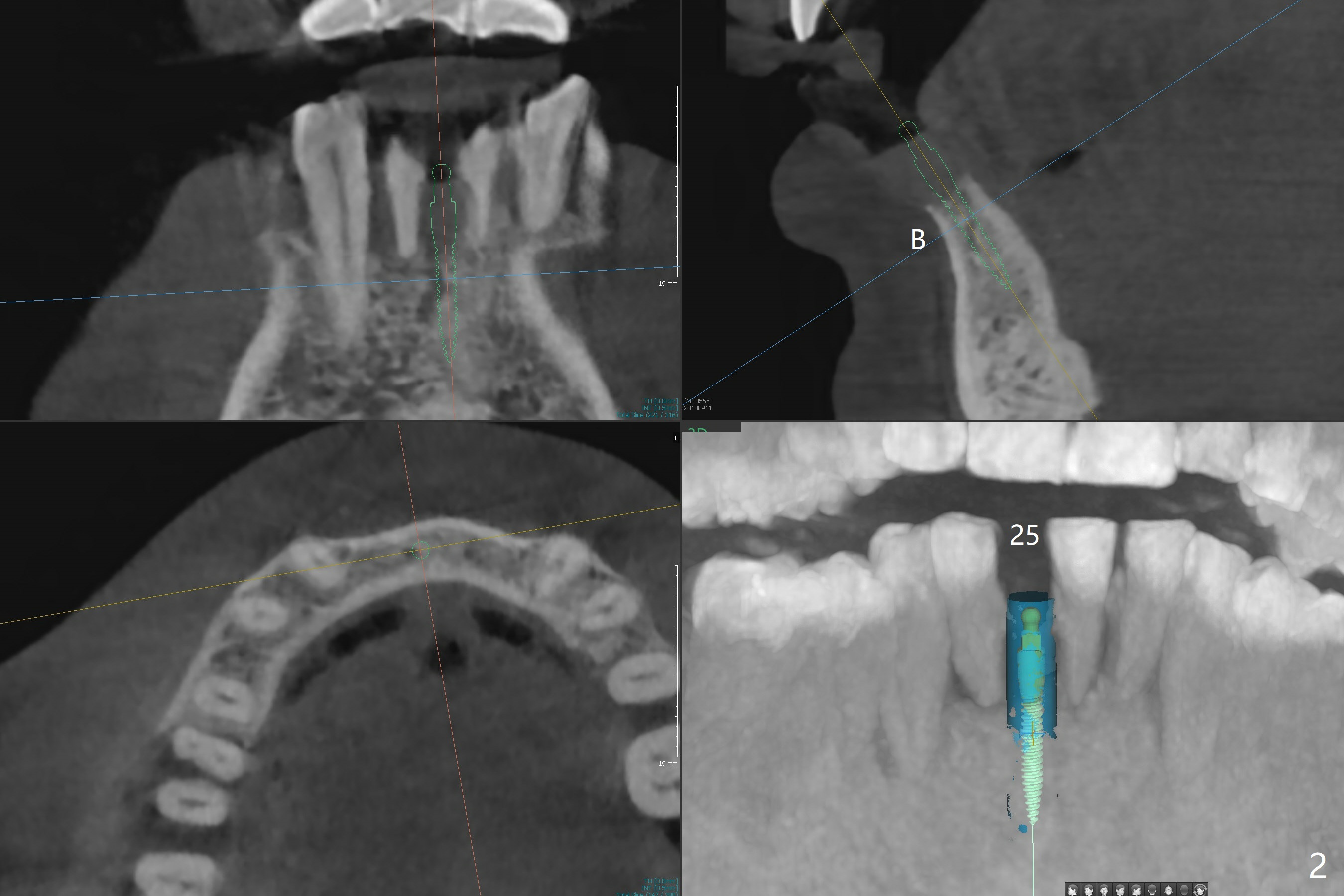
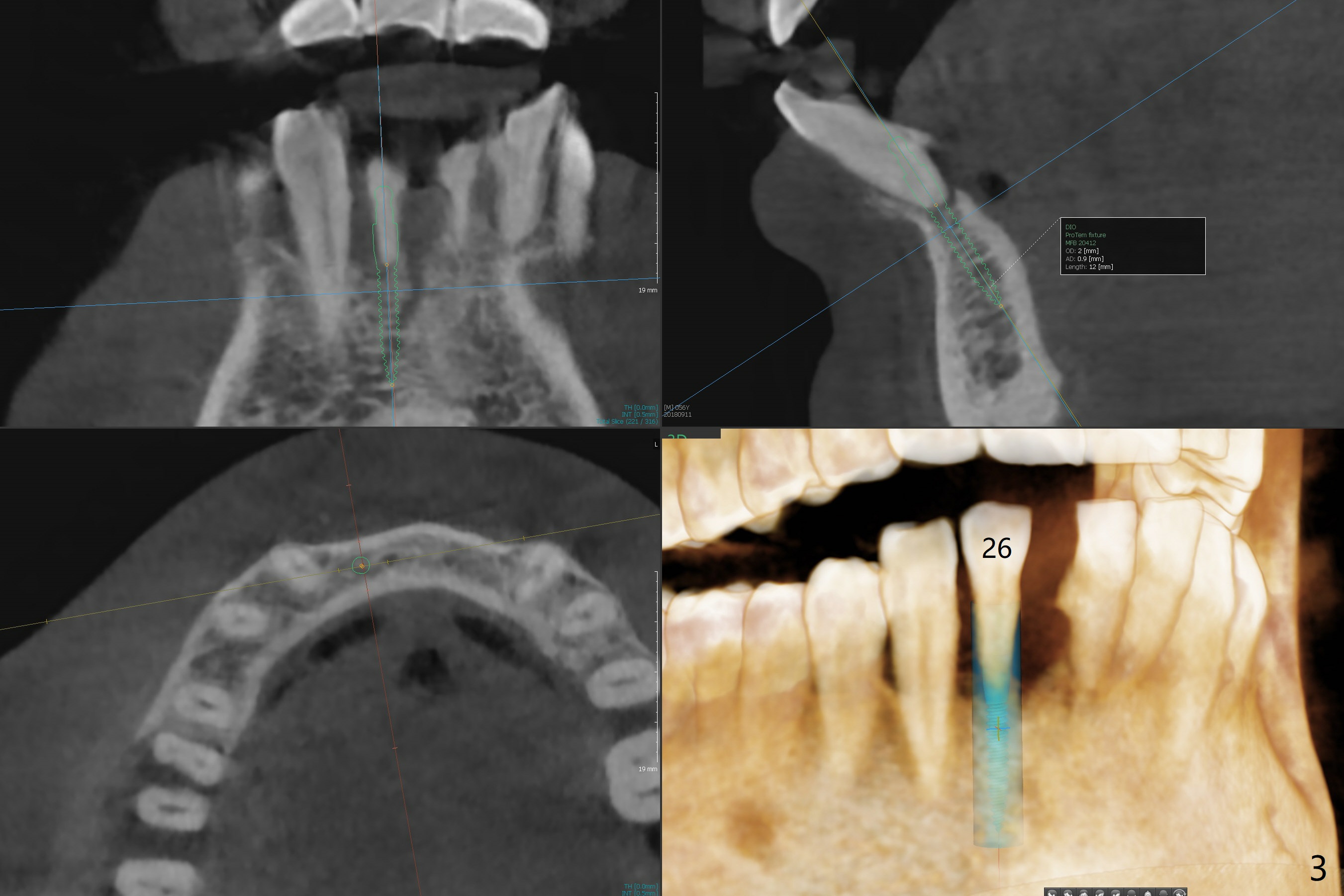
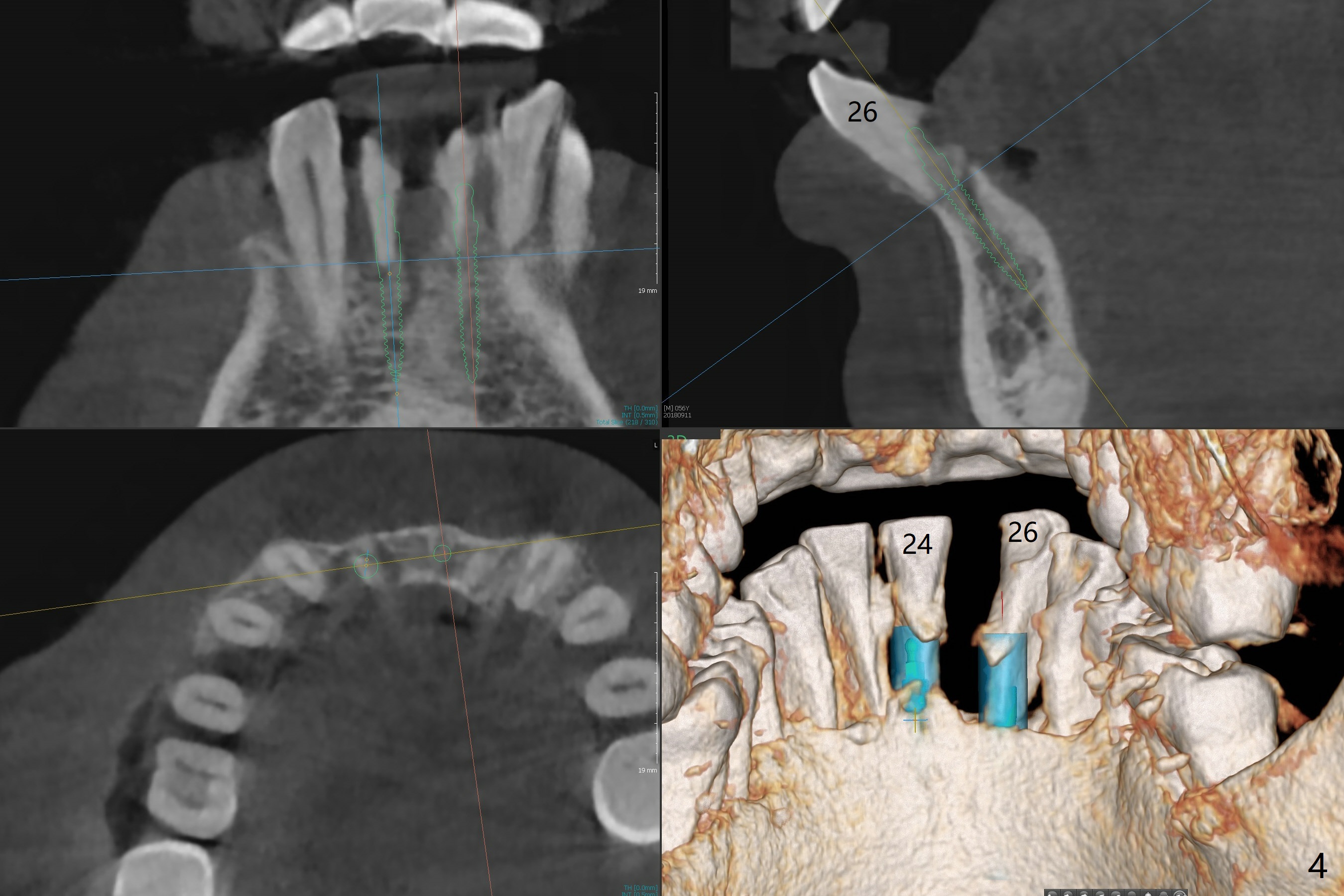
Single or Multiple 1-Piece Implants
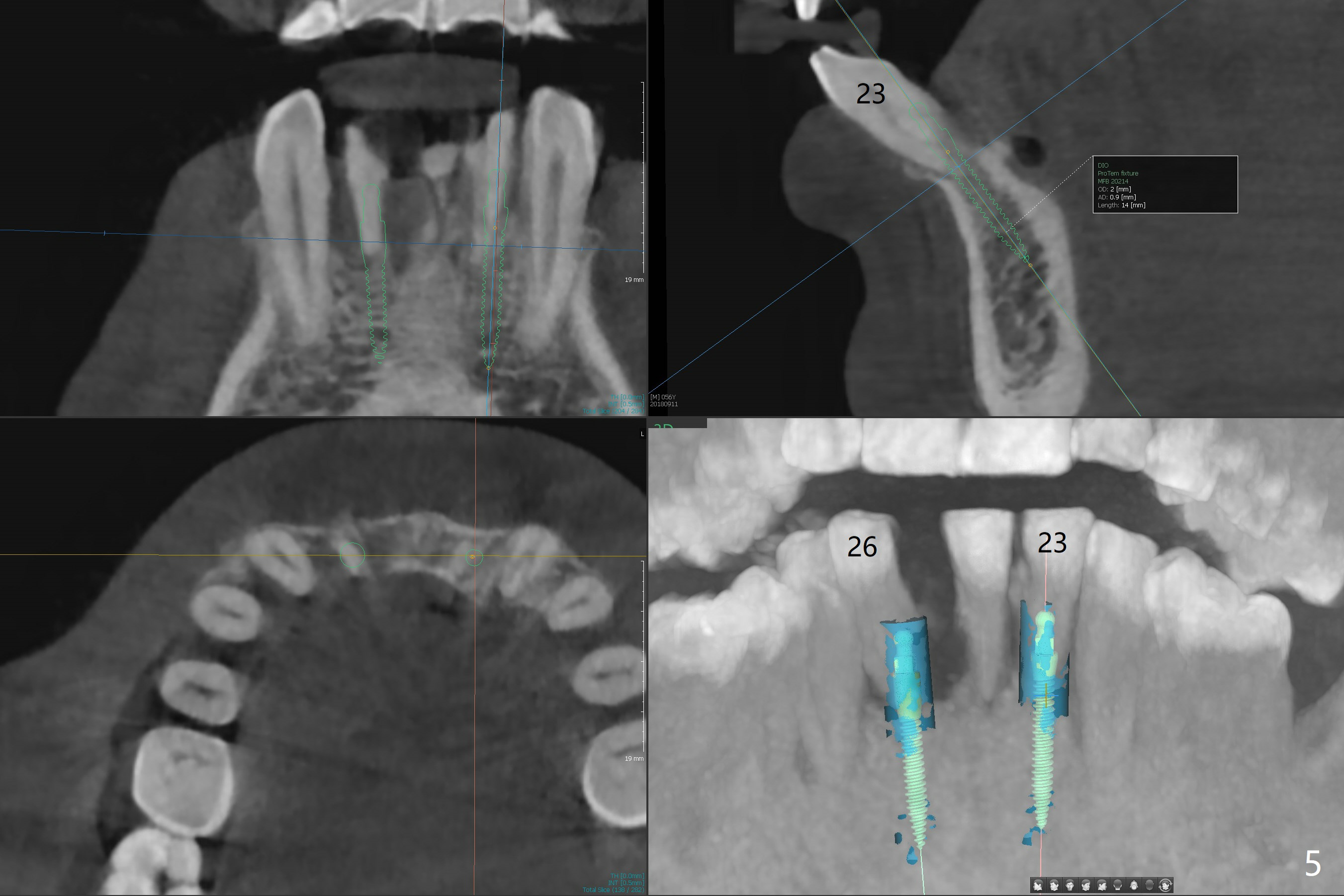
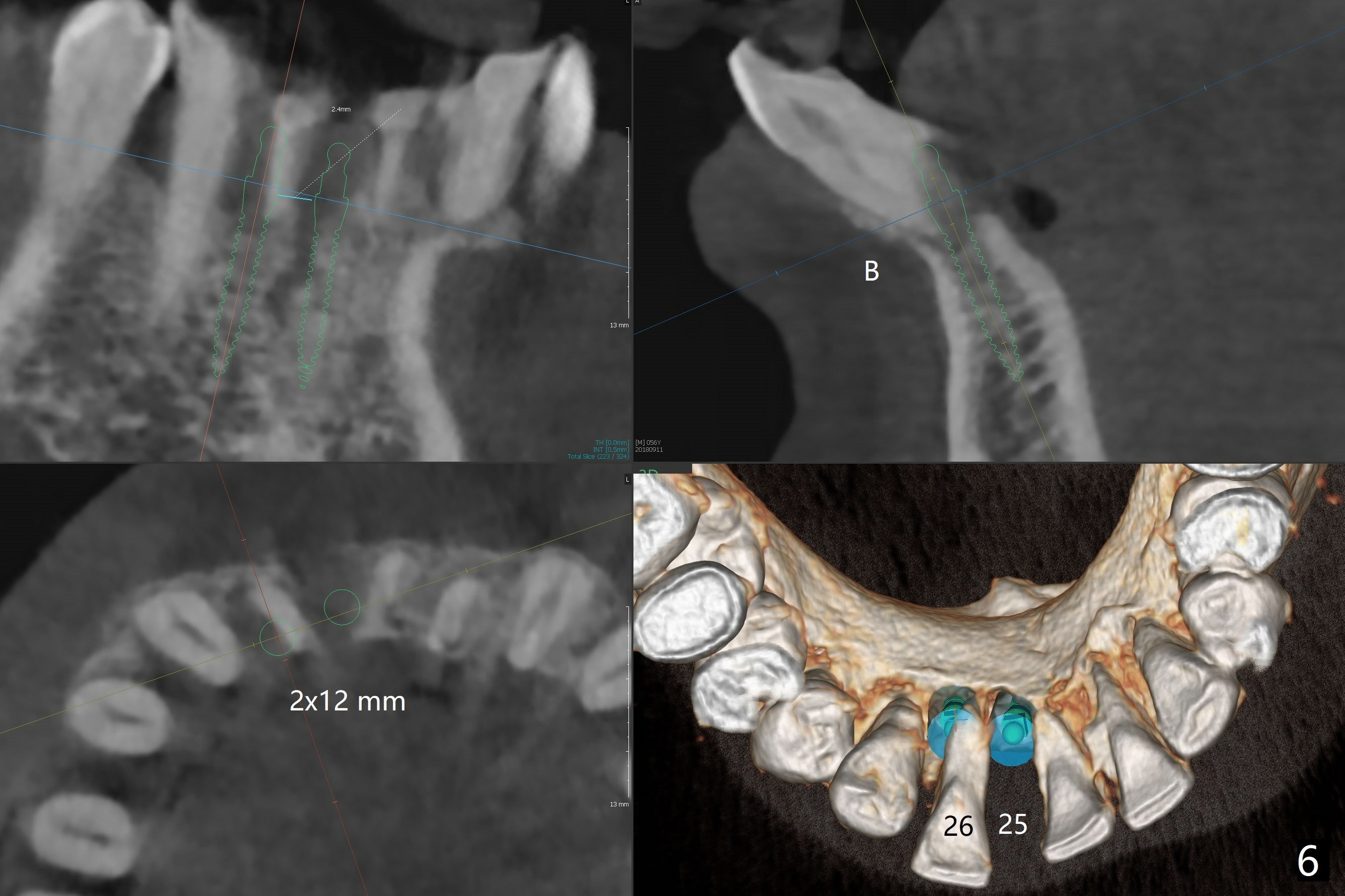
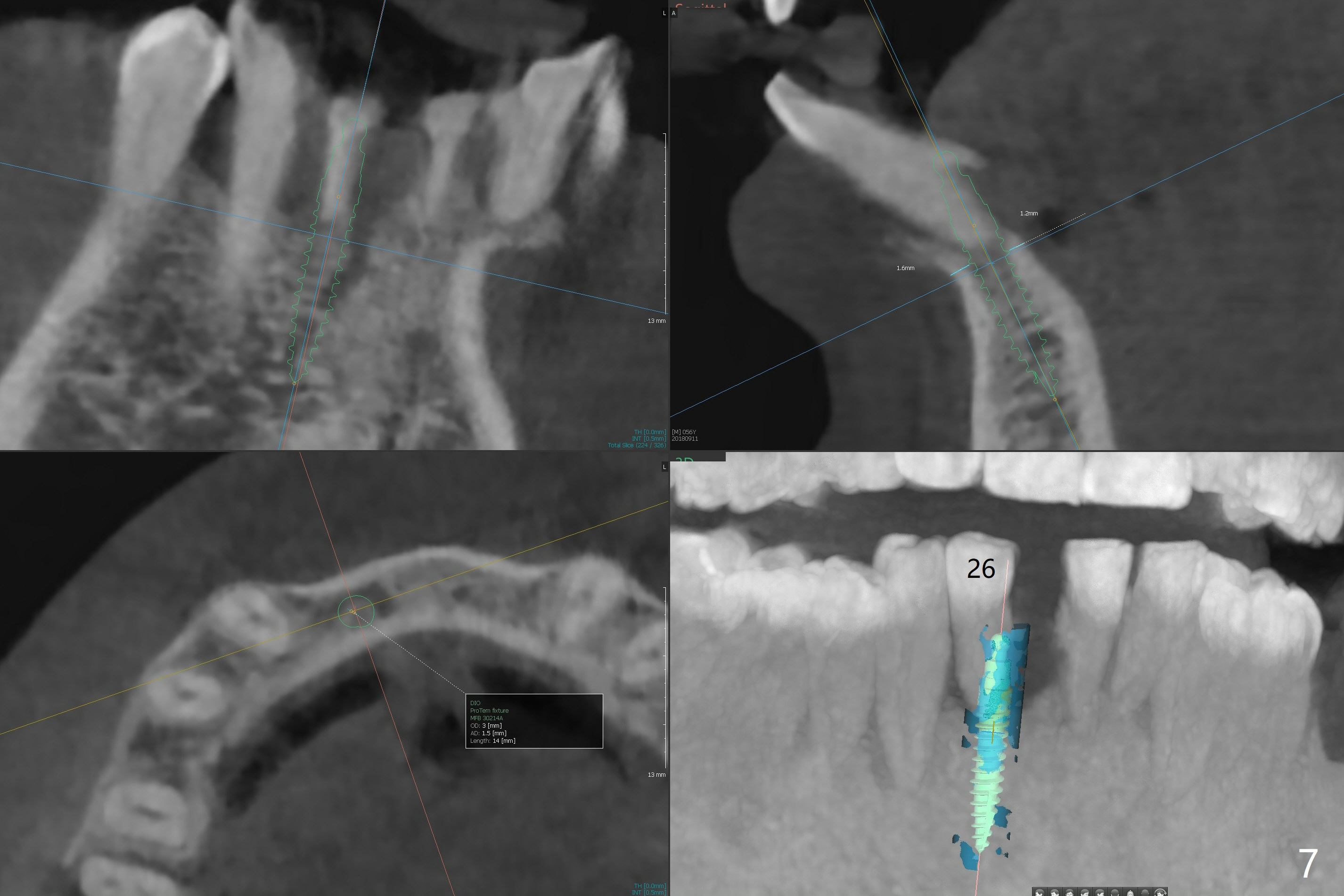
A 56-year-old man is a dental phobic. He finally seeks treatment because of loss of the tooth #25 with air leakage during speech (Fig.1). If the remaining lower incisors are stable after scaling and root planing, a 2.5 or 2.0 mm 1-piece implant will be placed in the narrow edentulous space (Fig.2). The implant driver (green sleeve) may touch the neighboring teeth, which need adjustment. If the worst incisor (#26 tender prior to SRP) is deemed to be non-salvageable, a 2.5 mm implant will be placed with a cantilever 2-unit FPD (Fig.3). If the tooth #23 is a survivor, two of 2.5 or 2.0 implants will be placed at #24 and 26 with a subsequent FPD (Fig.4). If the remaining incisors are all questionable in prognosis, two implants will be placed in the ends with a FPD (Fig.5). After SRP, the tooth #26 is less tender; the patient is ok with its extraction, but insists on saving #23 and 24. If 2 implants are to be placed at #25 and 26, they need to be 2 mm in diameter (Fig.6) with risks of injuring the neighboring teeth. It appears that it is more reasonable to have a single implant, slightly larger (2.5 or 3 mm), at #26, with the coronal end slightly mesial (Fig.7) with a cantilever bridge. If the teeth #23 and 24 fail in the future, a normal one will be easily converted.
Return to Lower Incisor Immediate Implant, Trajectory, Metronidazole Xin Wei, DDS, PhD, MS 1st edition 10/14/2018, last revision 05/30/2019