.jpg)



|
|
|
|
|
|
|
|
|
|
|
|
|||
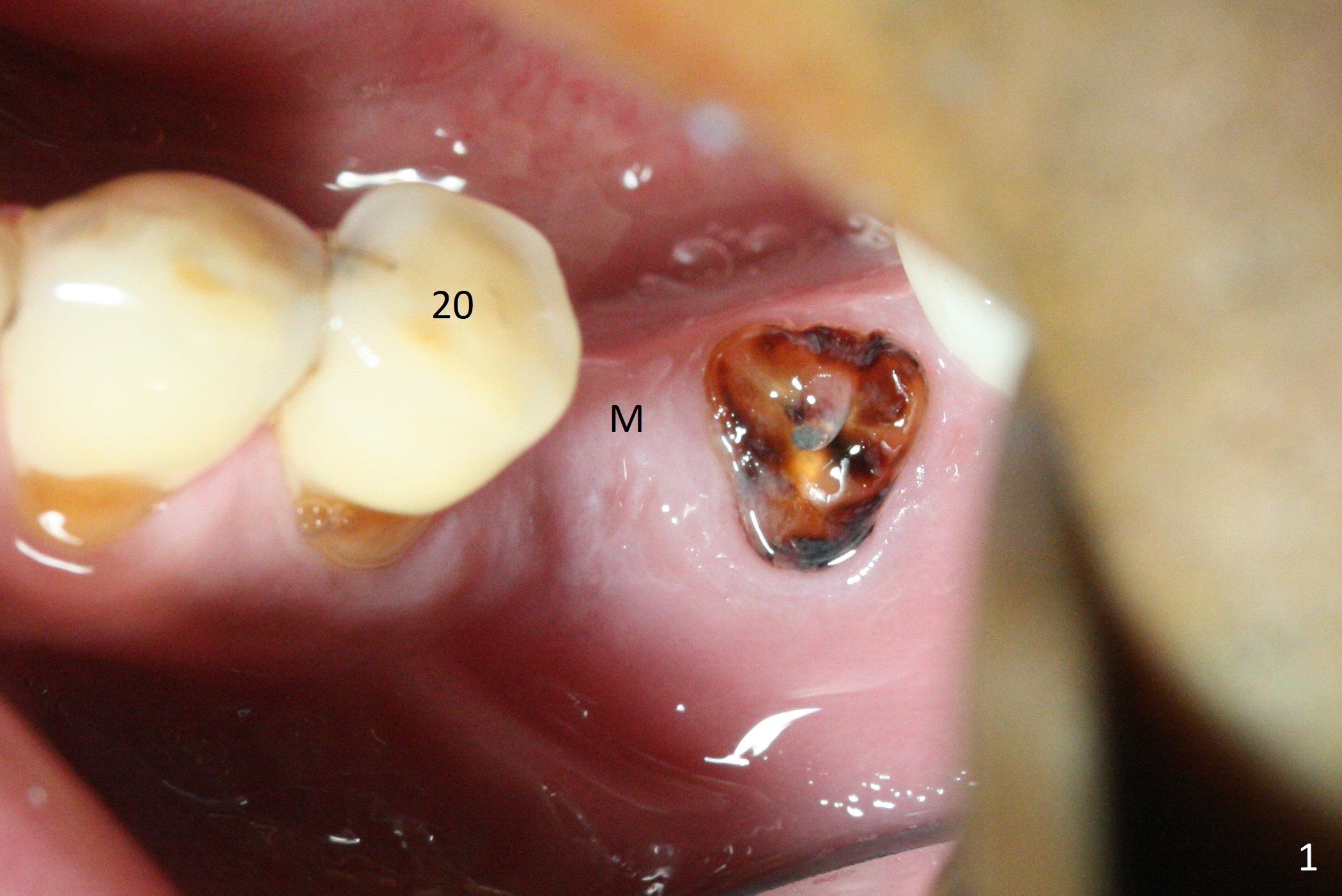
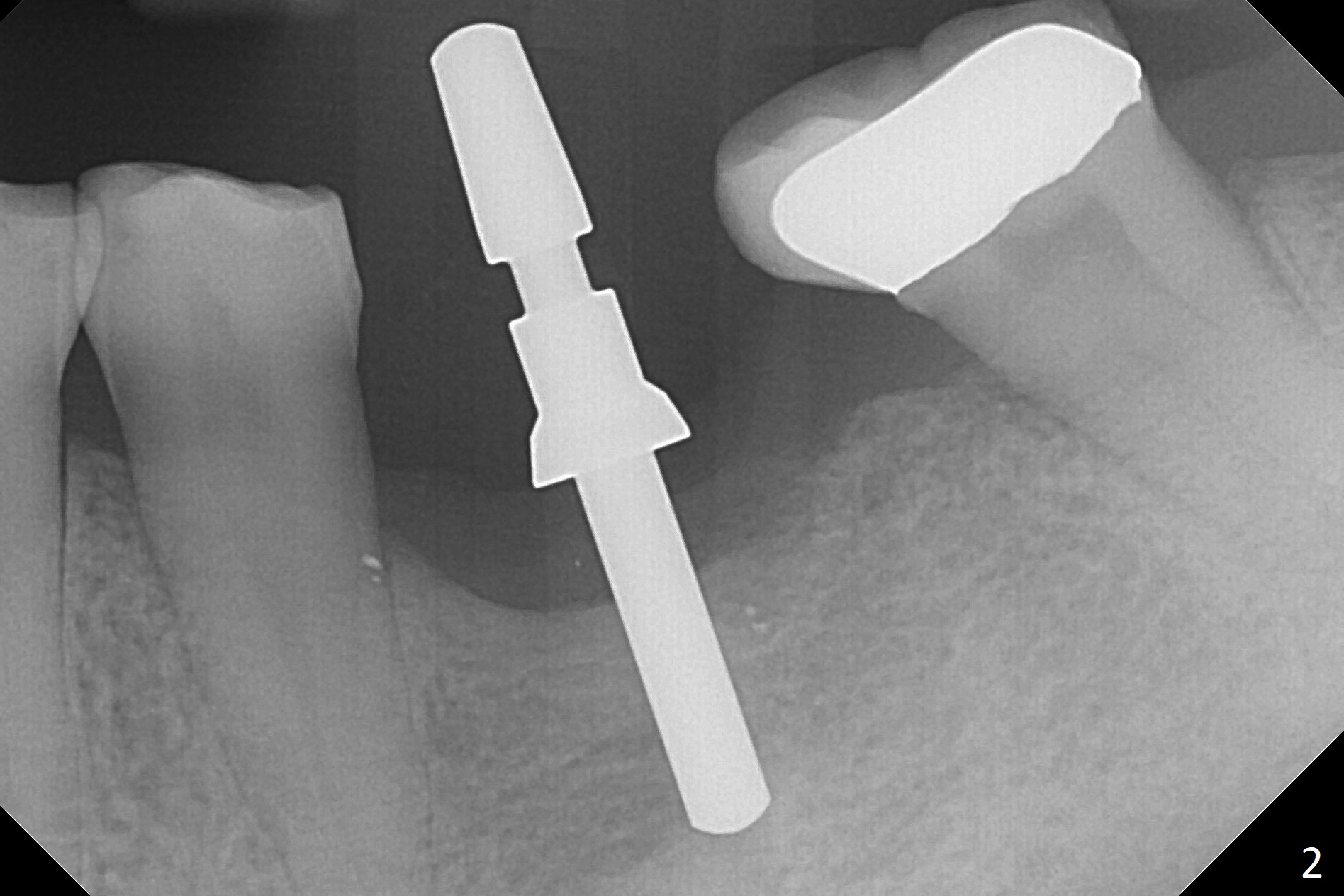
Place Implant at Buccal Crest
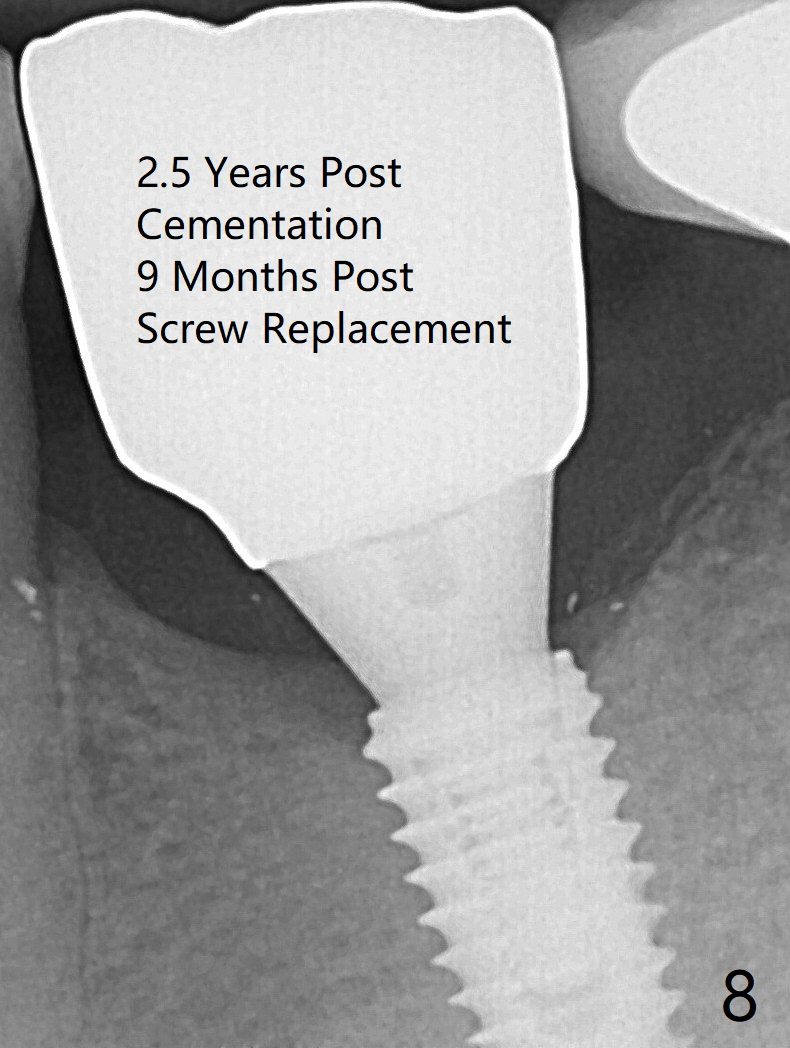
After extraction of the distal residual root at #19 (Fig.1), osteotomy is initiated in the mesial (M) aspect of the distal socket (Fig.2). Magic Split proves dense bone. When a 4.5x10 mm dummy implant is placed with stability, there is an apical space (Fig.3 <); the dummy abutment is 5.7x5.5(2). With the final implant (4.5x10 mm, Fig.4) being placed deeper to close the apical space, the cuff of the final abutment increases by 1 mm. Autogenous bone is used to pack around the implant distobuccally (*). Although the implant seems to be placed significantly apical to the lingual crest (^), it is at the buccal crest. There seems to be no bone loss 3 months postop; impression is taken (Fig.5). The crown/abutment at #30 is retightened 22 days post cementation (5 months postop), probably related to unilateral mastication. In fact, #30 is the only functioning molar on the right side (with unfavorable crown/implant ratio (long cuff 4 mm, vs. 3 mm at #19); #2 severely decayed); the crown at #19 is cemented at the same appointment (Fig.6). The crowns/abutments at #19 and 30 are loose 7 months later. When the crown/abutment at #30 is loose 2nd time 1 year 7 months post cementation, the screw at #19 fractures (Fig.7 taken post retightening). The tooth #2 needs a crown. The patient cannot use the anterior teeth, since the teeth #8 and 9 have root fracture. Can extraction and bone graft increase bone height? The abutment remains incompletely seated 9 months post screw replacement. It should be fixed soon. Return to Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), Armaments Screw Xin Wei, DDS, PhD, MS 1st edition 12/22/2017, last revision 02/24/2021