.jpg)
,%204.5%20m%20postop.jpg)

|
|
|
|
|
|
Guide and Flap Surgery
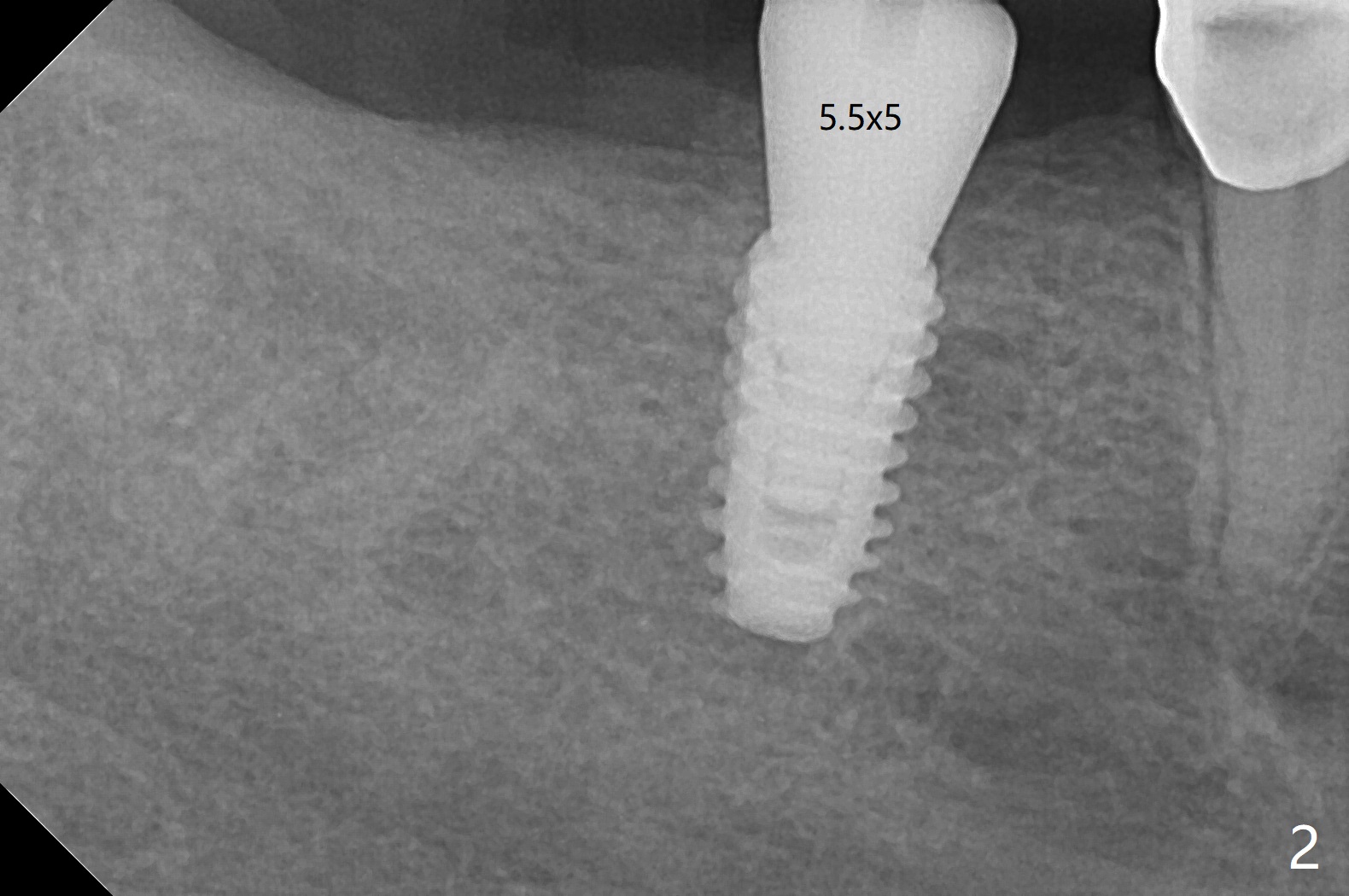
When the guide is seated for #30 implant, it appears that the tissue punch may remove all of the buccal keratinized gingiva. Therefore incision is made with flap reflection. The bigger advantage of flap surgery is that as the implant is placed, the lingual crest is found to be the lowest (which is the most likely to be neglected with flapless approach) so that bone graft can be easily placed. In contrast the mesial crest is the highest. For seating of a cemented abutment (Fig.1) and a healing abutment (Fig.2), profile drills (5.5 and 6.0 mm) have to be used, respectively. Following #31 extraction, Vanilla graft (minor portion) and Osteogen Plug (major portion, most likely no implant in the future) are placed, followed by GEM Cap and 4-0 Chromic Gut suture. After removing the healing abutment 4.5 months postop, a 5.5x4(3) mm cemented abutment is seated completely; it appears that the distal crest resorbs substantially (Fig.3 *). The access hole is distal as related to distal end guide (in fact #31 was used as distal stop before extraction) and radiation interference from #29 crown (Fig.4). The uneven mesial and distal crest may be the main reason for the deviation.
Return to No Deviation GEM21S Xin Wei, DDS, PhD, MS 1st edition 06/04/2020, last revision 11/17/2020