

,%20Vanilla.jpg)

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|||||
Free-Hand: Buccal Placement
M
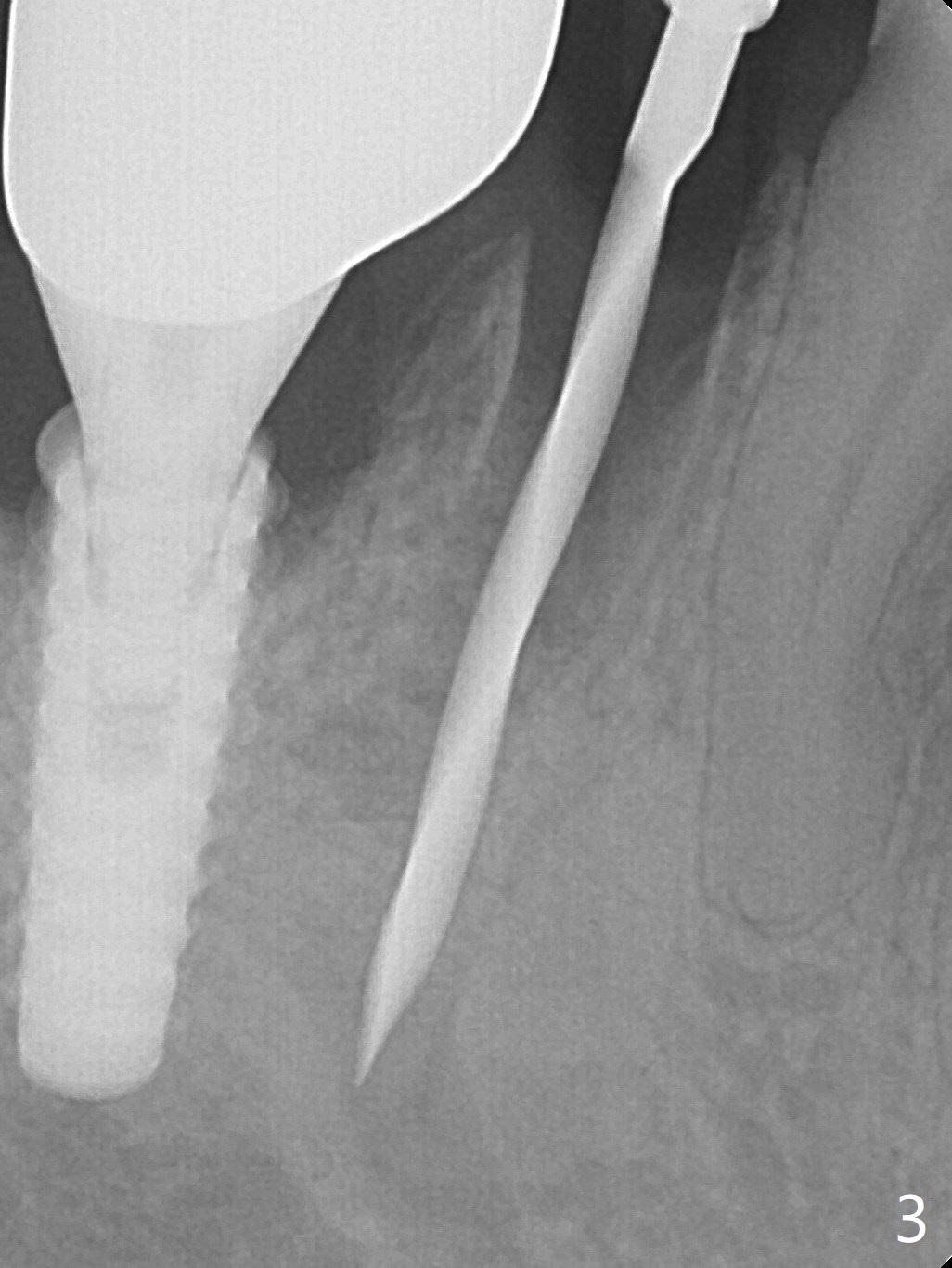
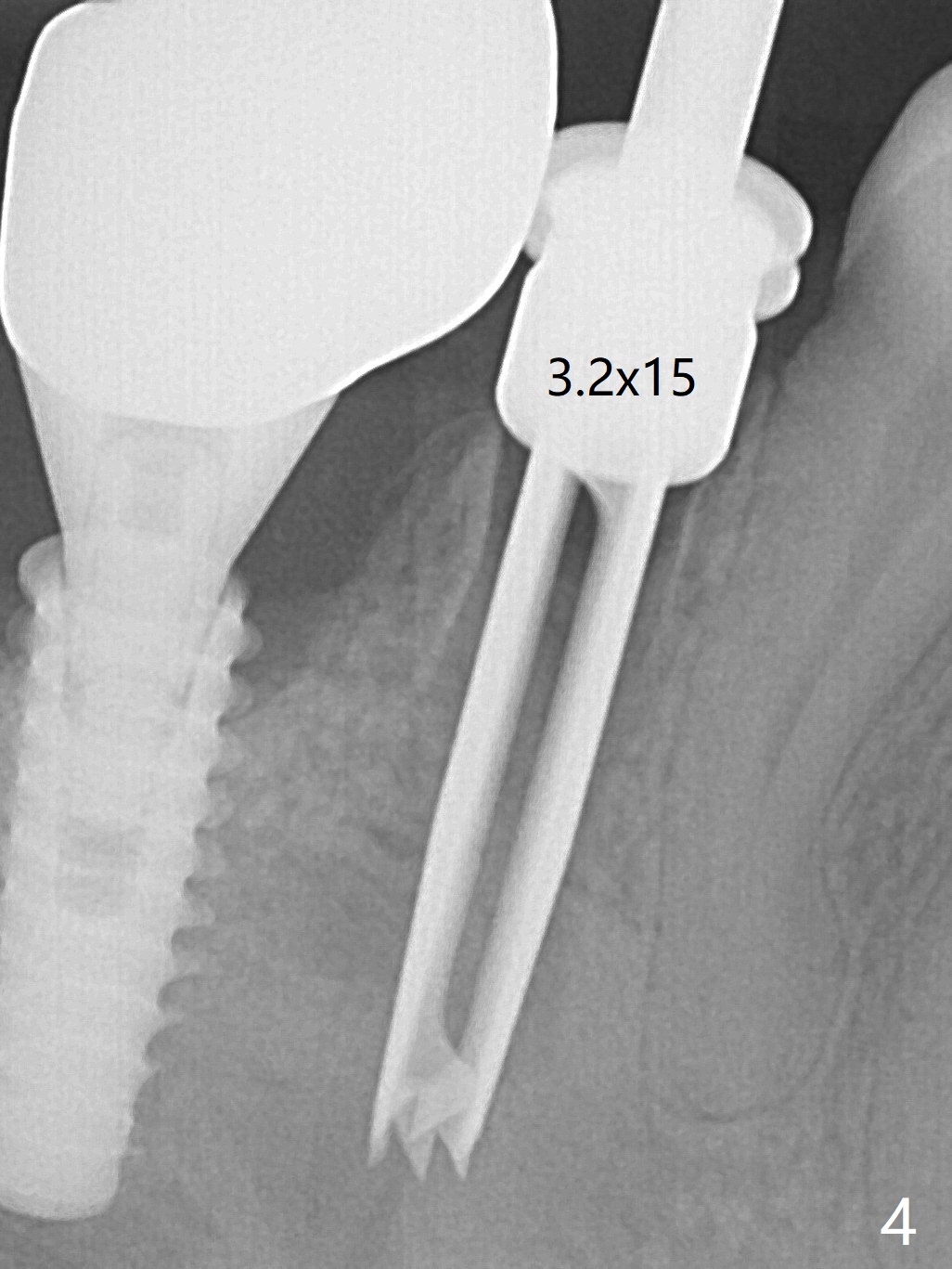
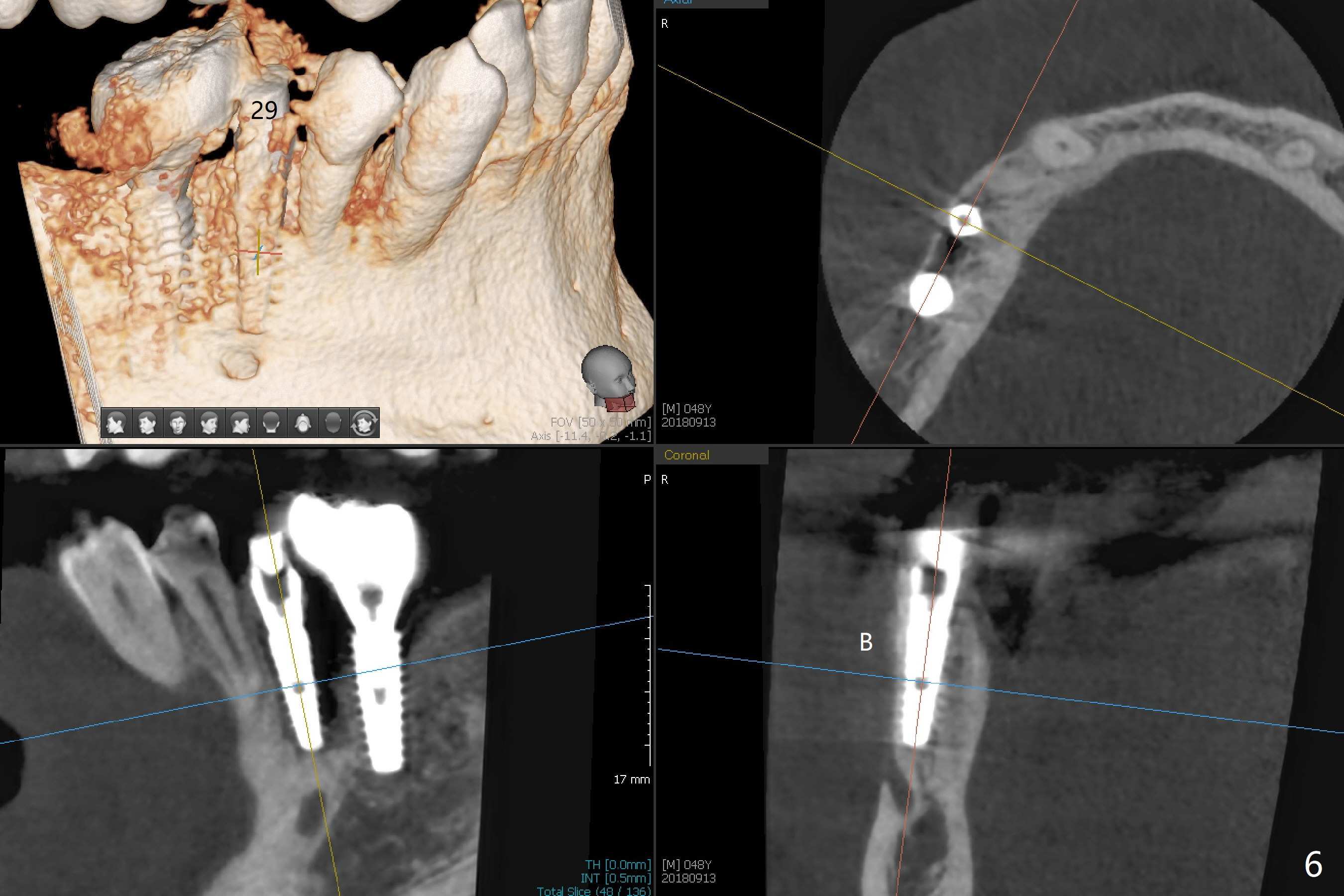
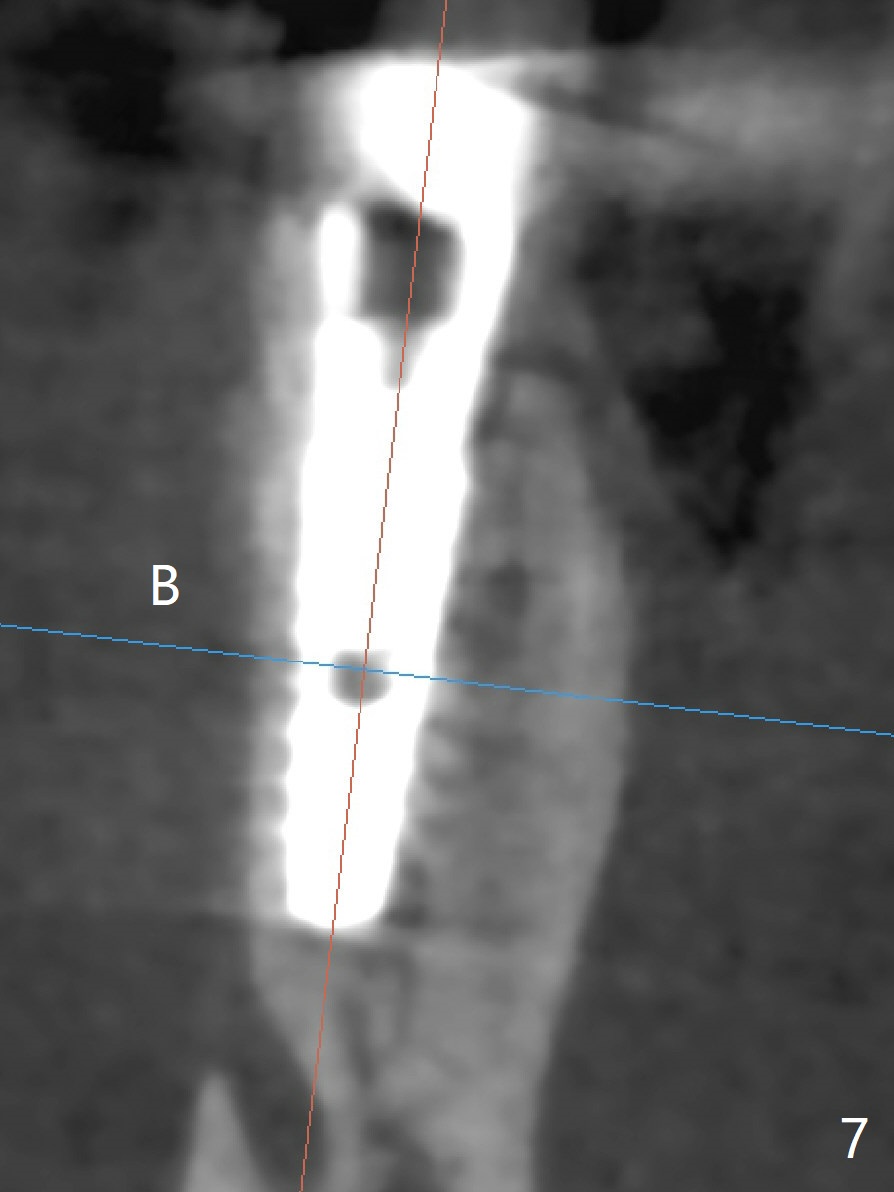
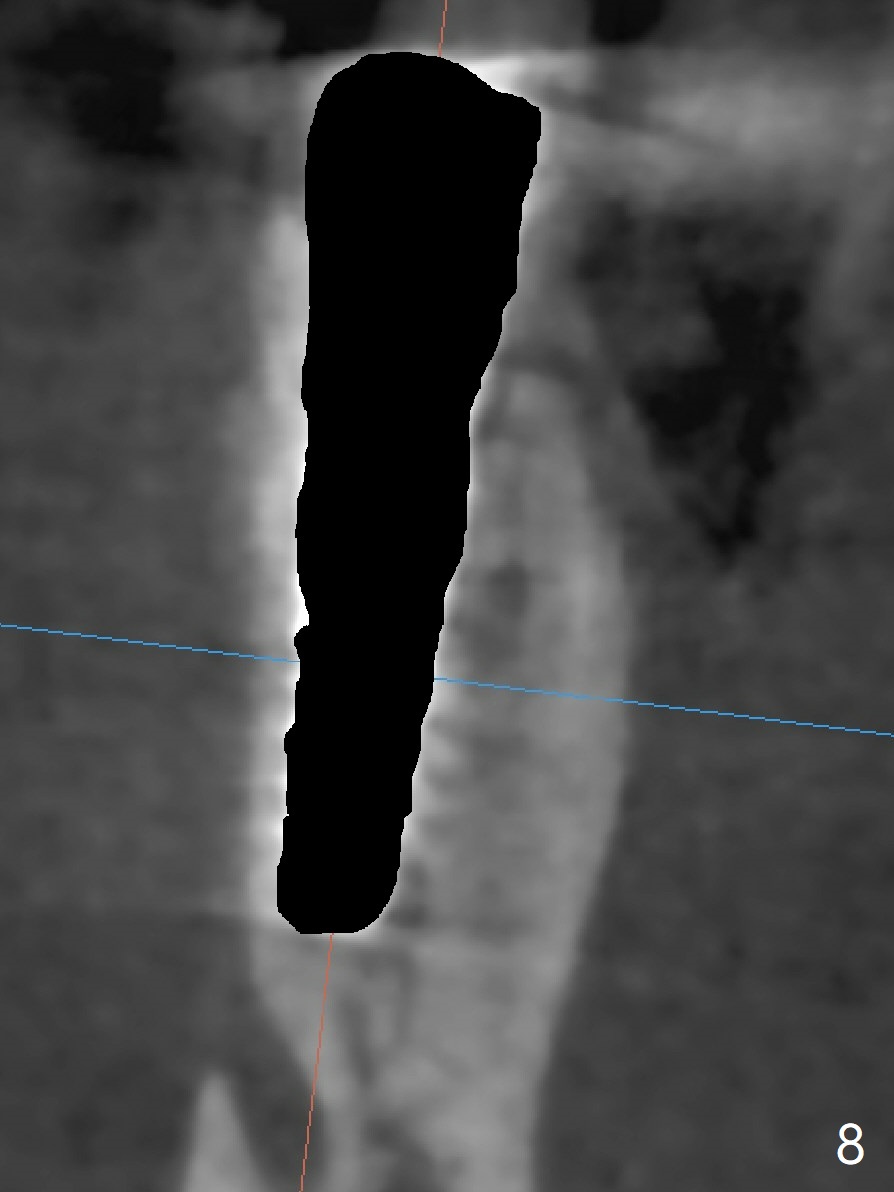
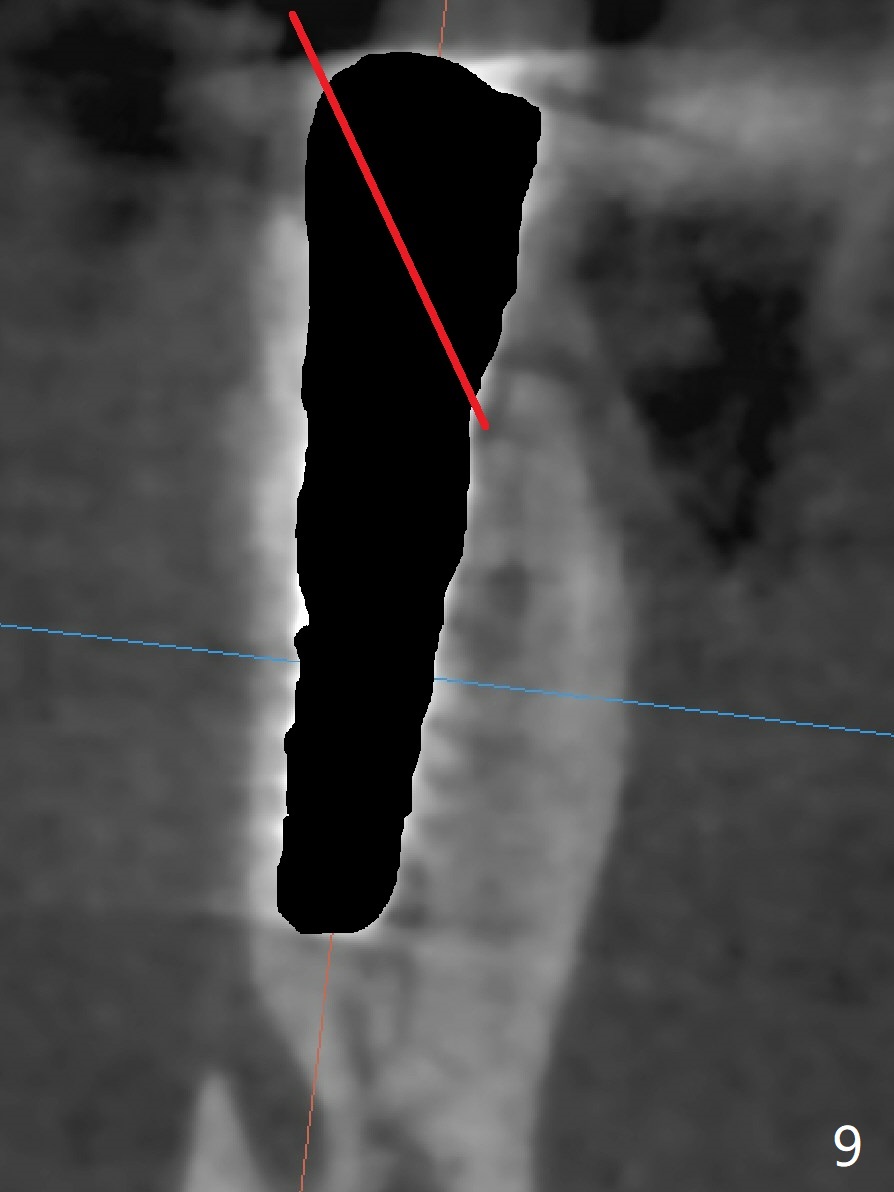
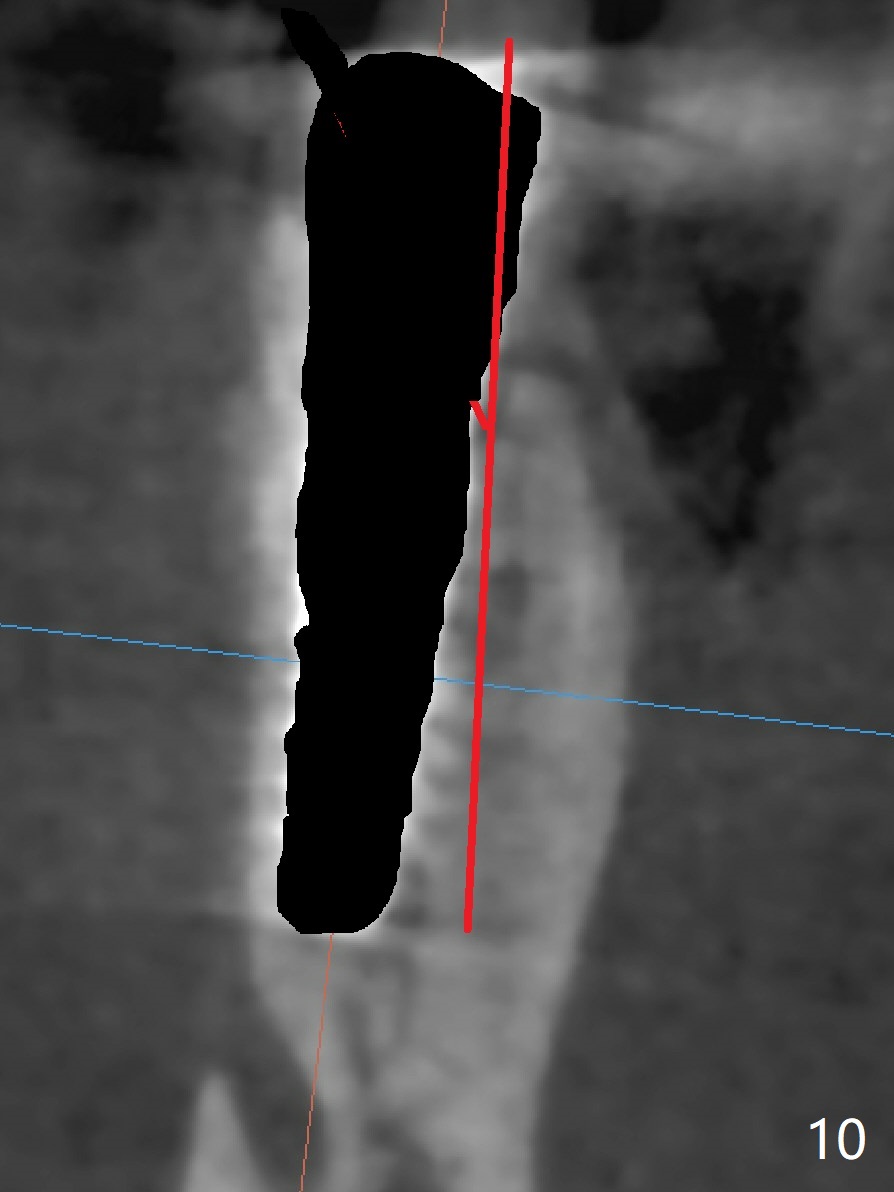
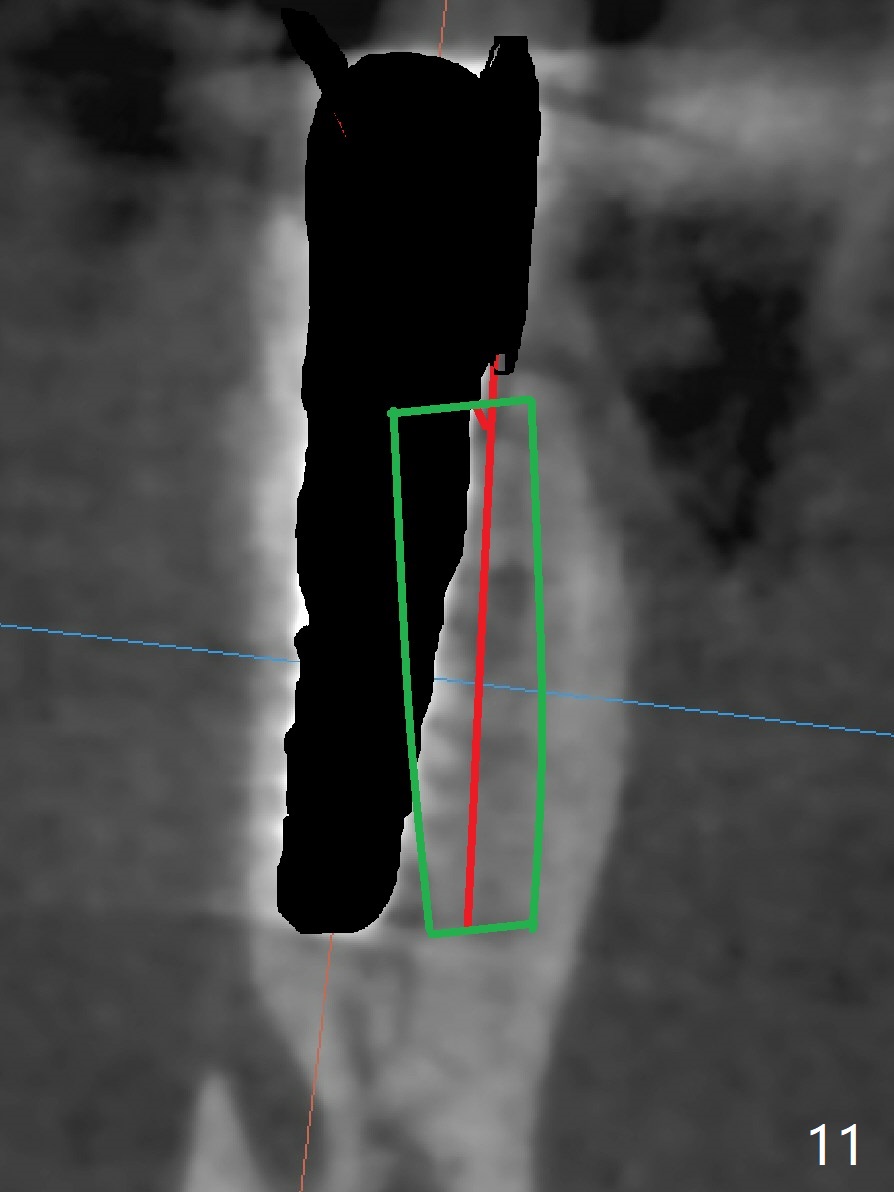
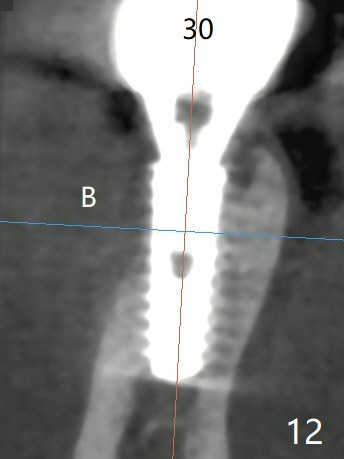
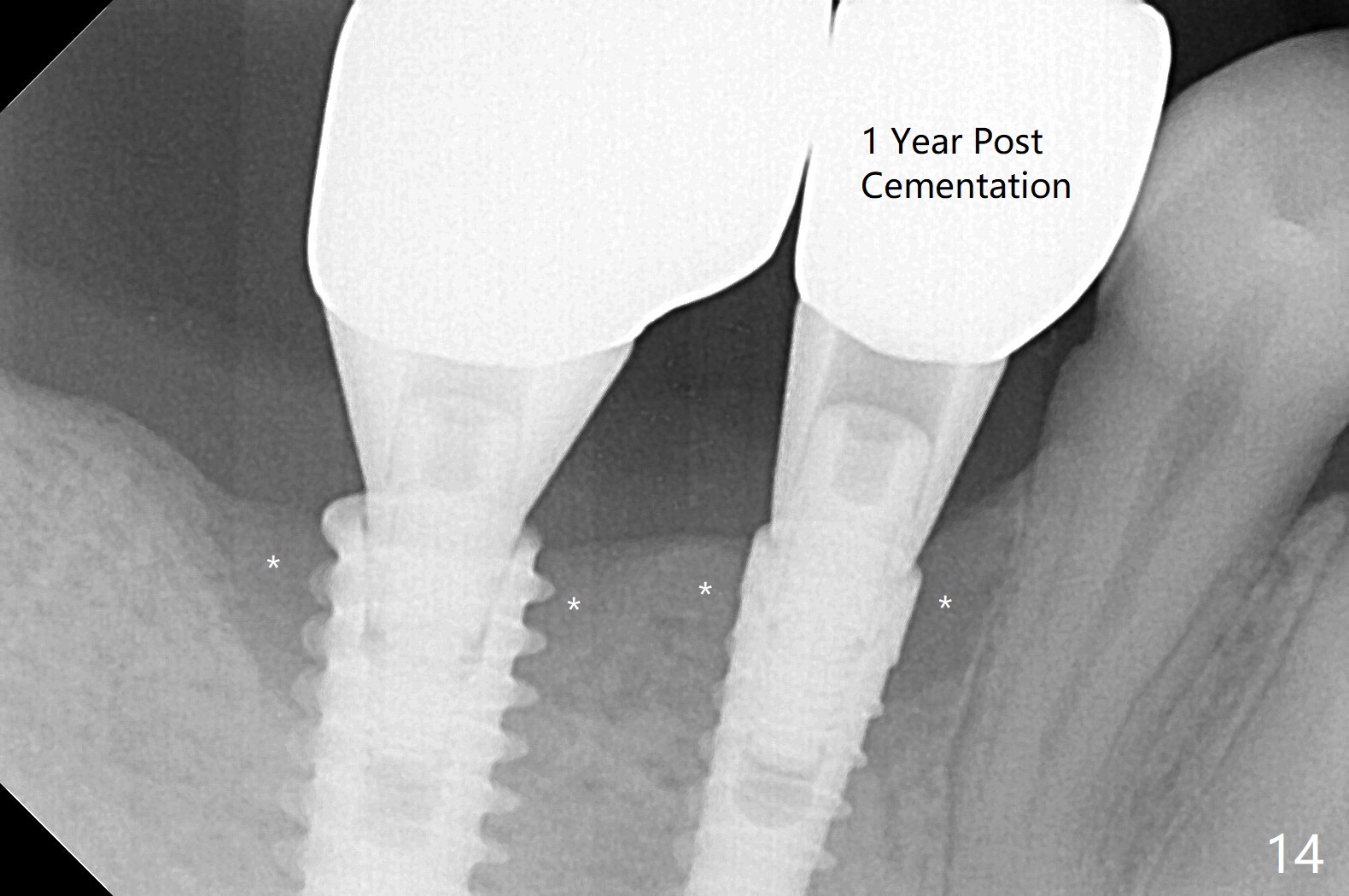
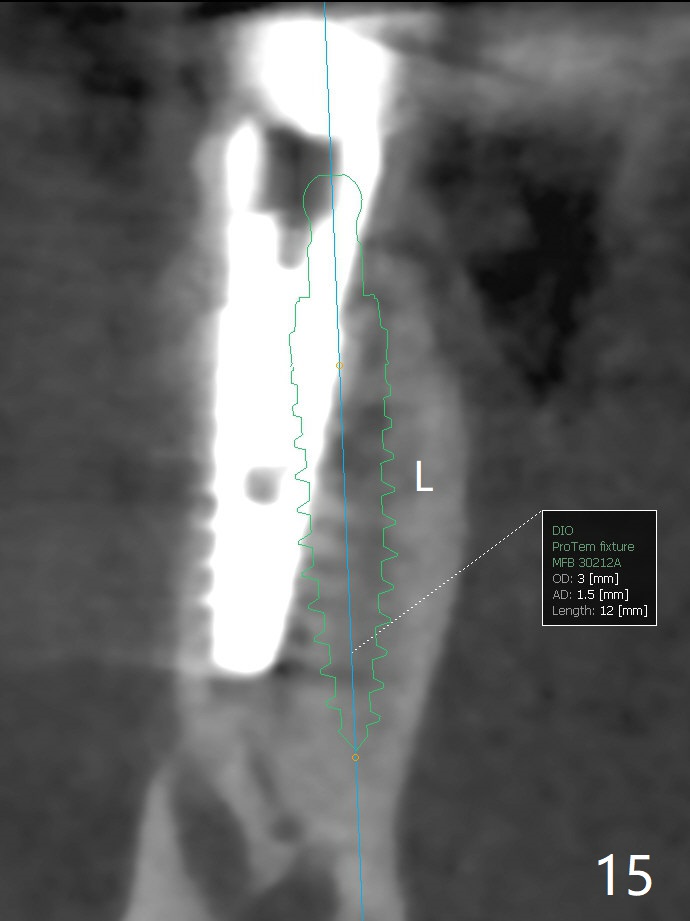
The tooth #29 has mild persistent pain radiating to the temple with mild percussion and mobility I 4.5 months post apicoectomy; the buccal recession is noticeable (Fig.1). Granulation tissue and bone graft are attached to the resected apex of the extracted tooth (Fig.2 <). The initial osteotomy with 1.5 mm drill is distal (Fig.3). After position adjustment with difficulty because of hard bone, osteotomy is finished with 2.8 and 3.2 mm Magic Drills (Fig.4). Following final drill, a 3.5x11 mm IBS implant is placed with insertion torque of 45 Ncm. With placement of a 4.5x4(4) mm abutment, Vanilla graft is placed in the buccal gap (Fig.5). Immediately postop CT shows that the implant is buccally placed (Fig.6,7 B). In fact after extraction (Fig.8), the initial osteotomy should start obliquely and as coronal and lingual as possible (Fig.9 red line). Following the initial penetration, the osteotomy should be straightened (Fig.10) so that the implant could be placed lingually (Fig11 green) to reduce buccal thread exposure. In fact there is also buccal thread exposure at #30 (Fig.12). The bone loss at #29 and 30 is minimal 4 months postop (#29, Fig.13 *)) and severe with periimplantitis at #29 one year post cementation (Fig.14). Incision will be made to exposure buccal threads of #29 and 30. If threads are within bone boundary, bone graft will be done with sticky bone after Titanium brush. If not, remove implant threads and bone graft. The worst scenario will be handled with implant removal (trephine bur 4/5 mm), either with bone graft or implant being placed lingually (IBS 3x11 mm 2-piece, to be buried, if needed (Fig.15)). Take preop photos to show #29 and 30 buccal recession and gingival erythema.
Return to Lower Premolar Immediate Implant, Trajectory, 6th Meeting, No Deviation
Xin Wei, DDS, PhD, MS 1st edition 09/13/2018, last revision 02/18/2020