

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
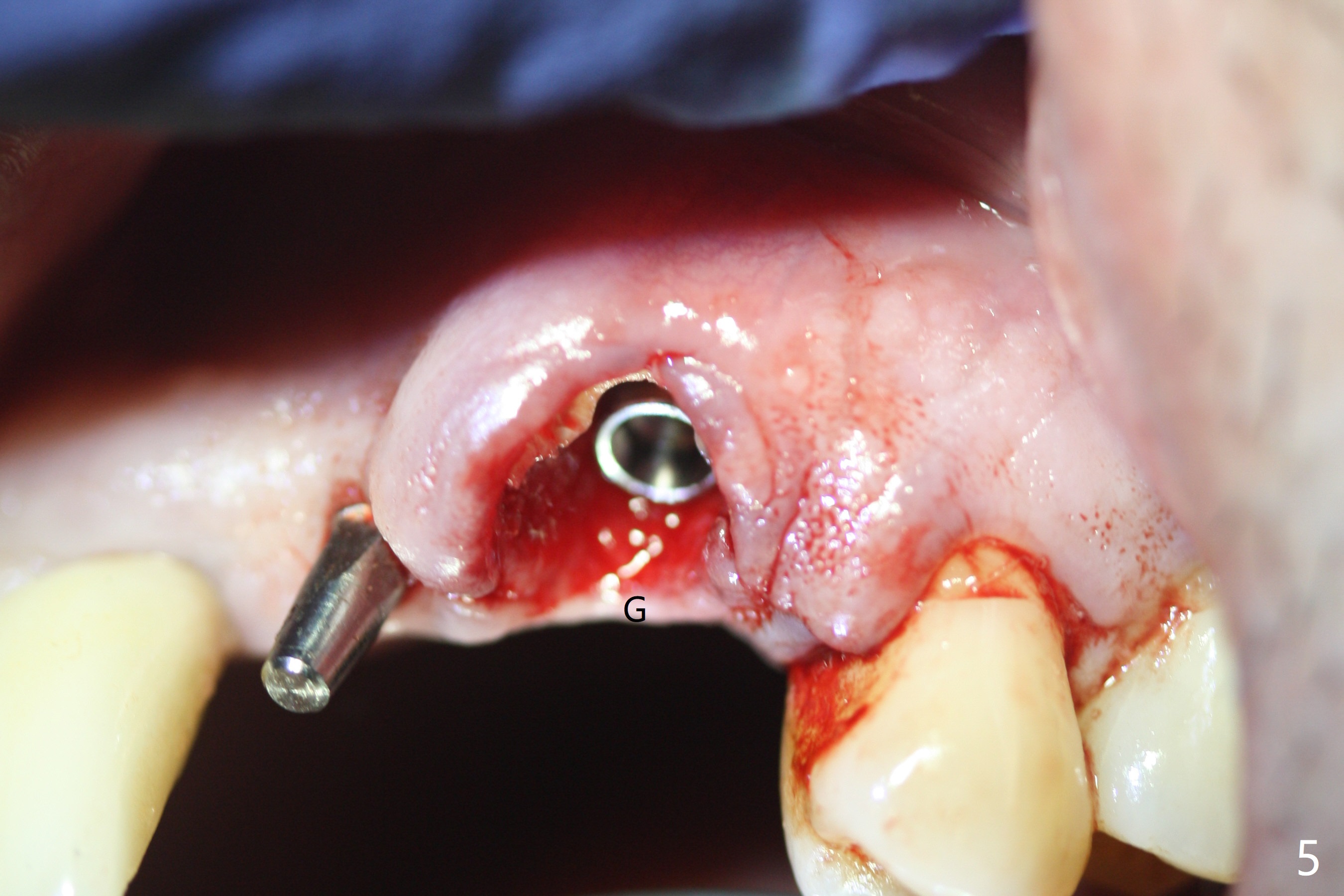
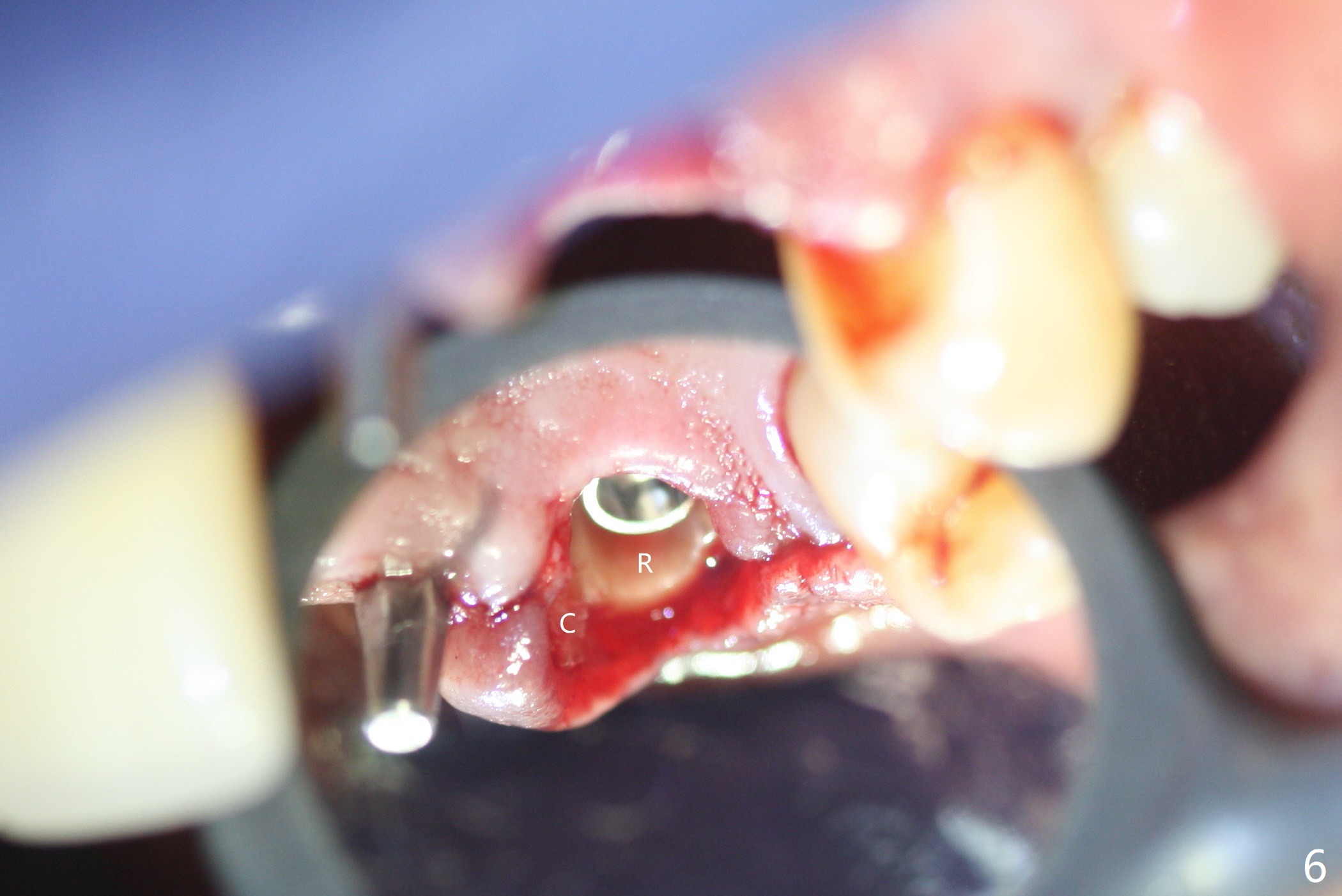
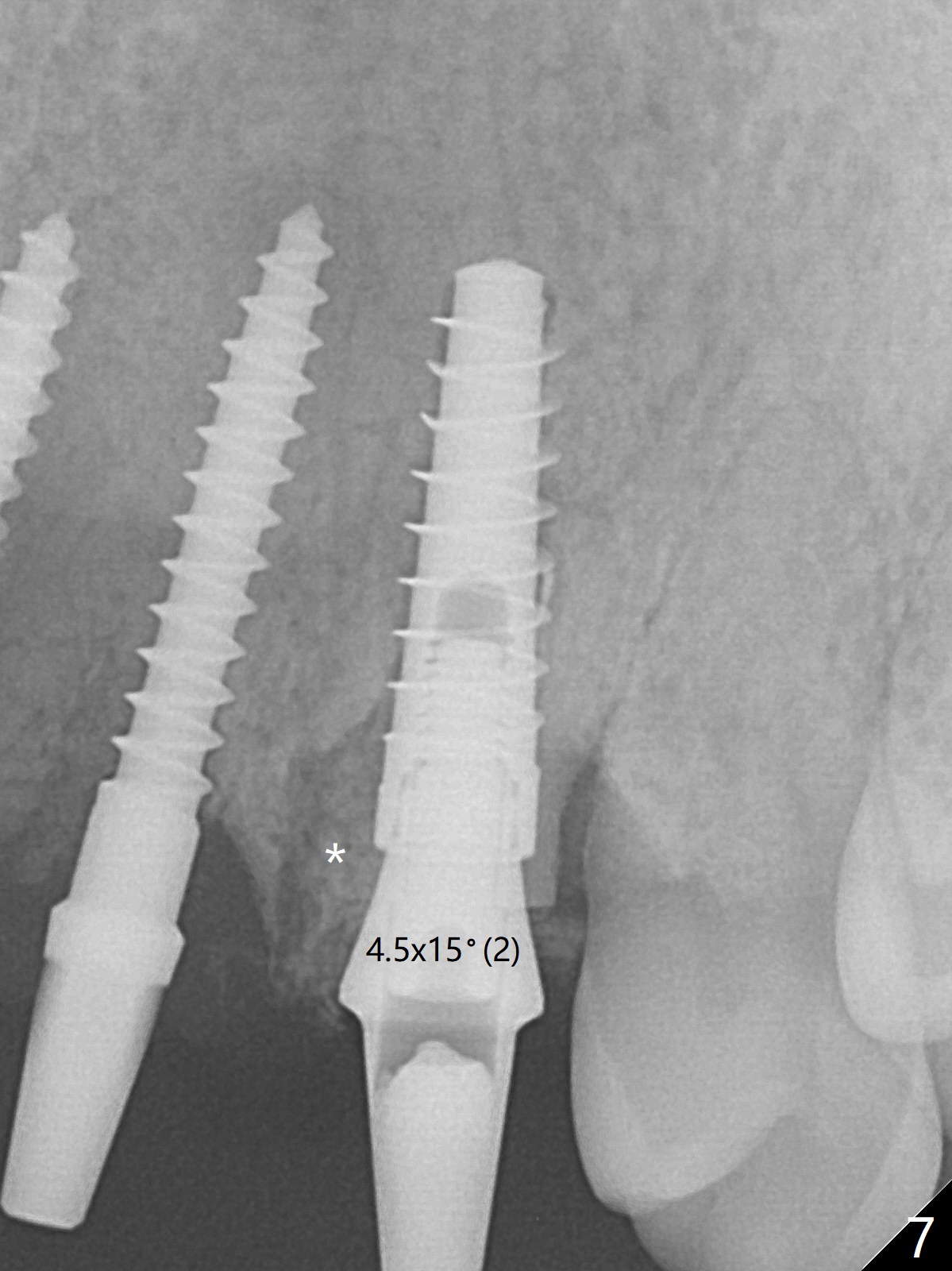
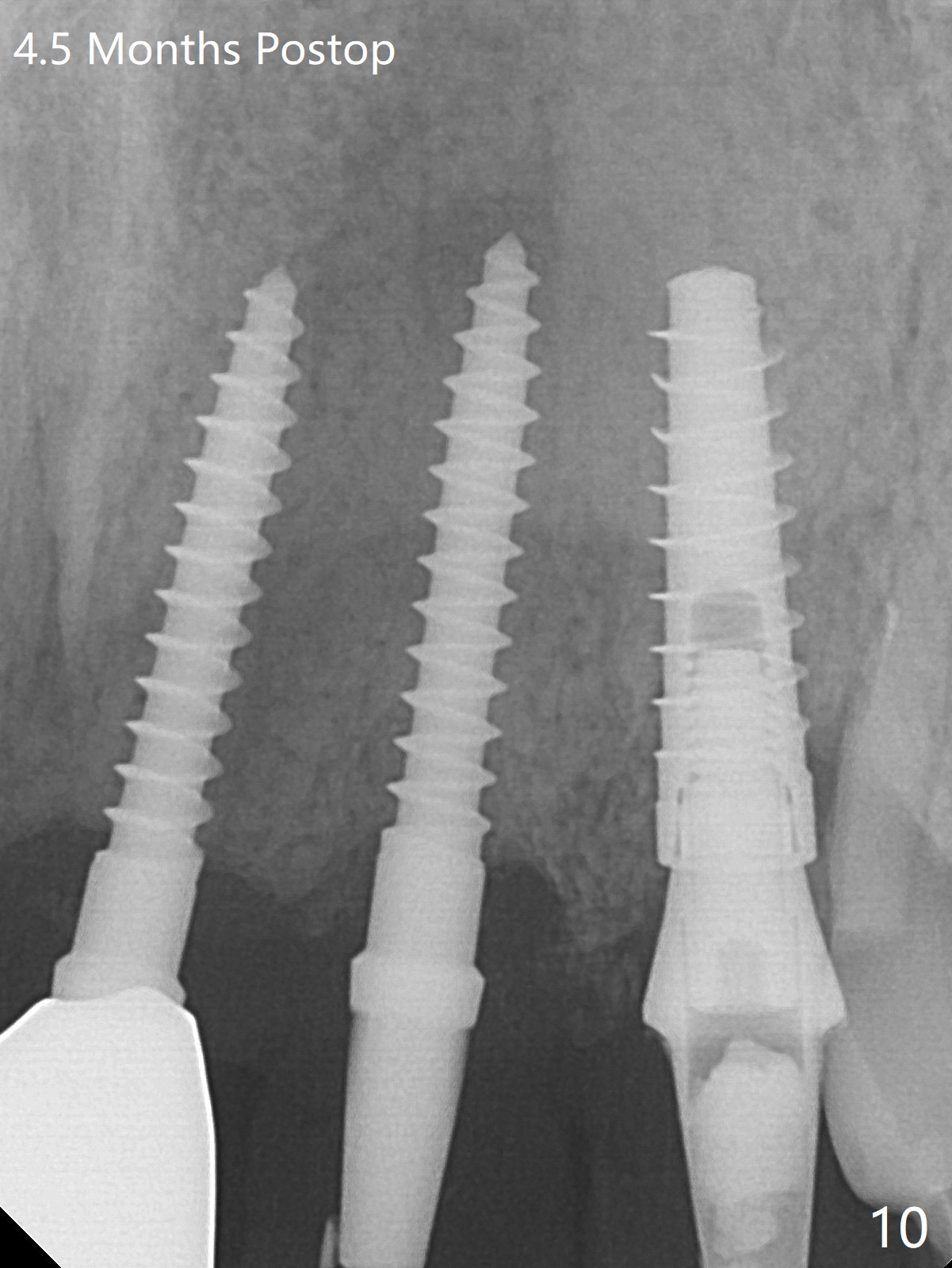
Socket Shield
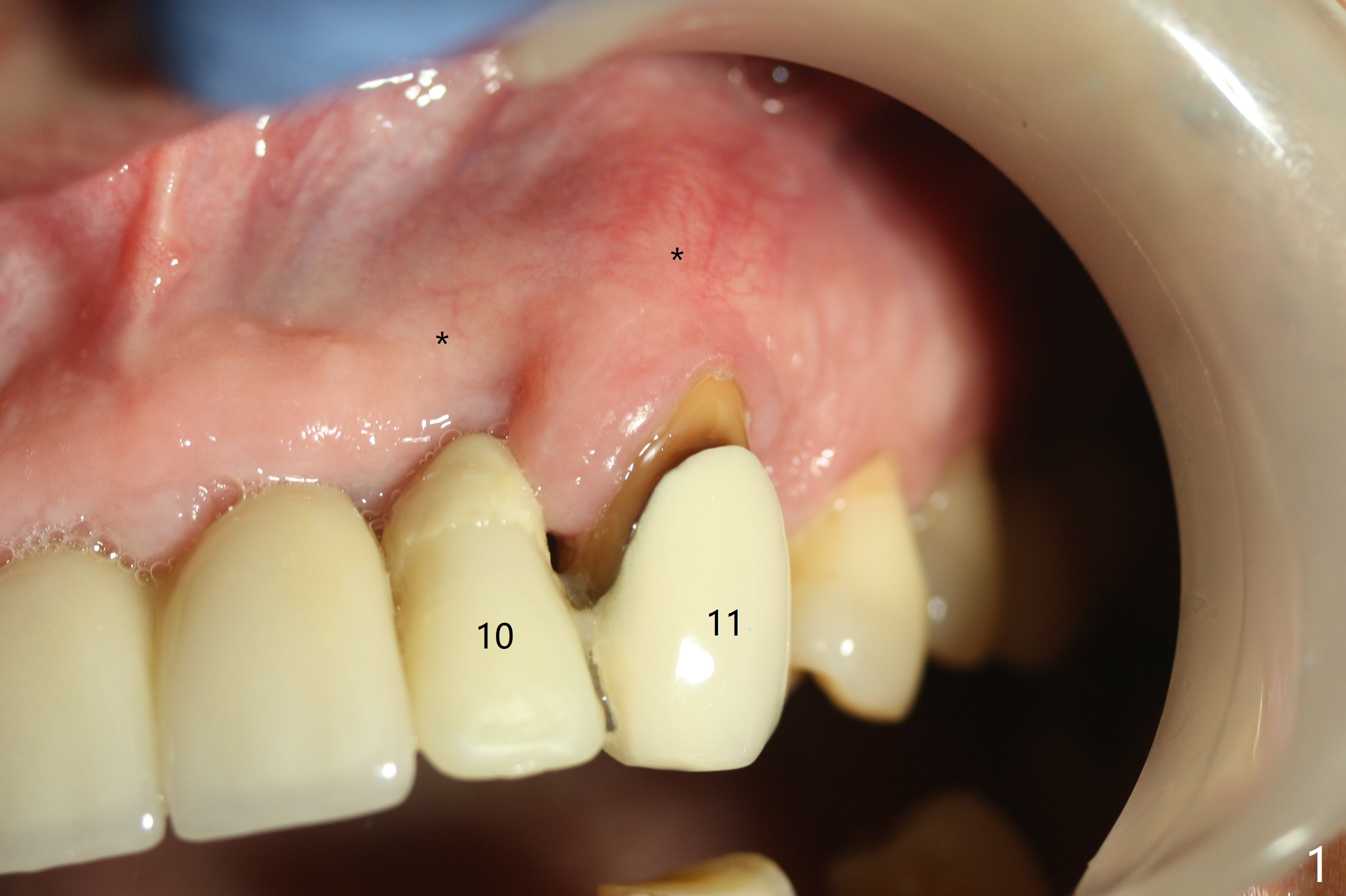
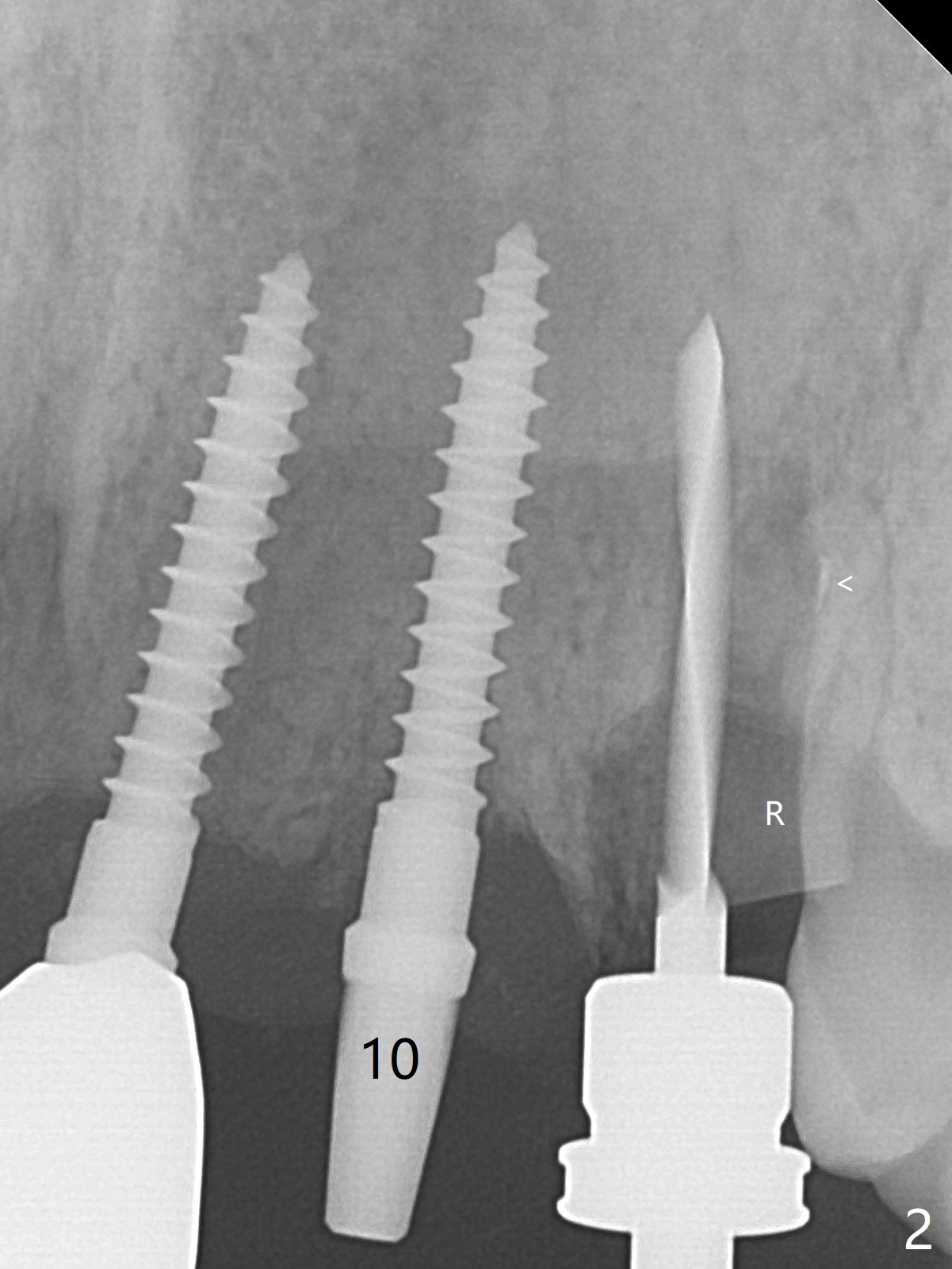
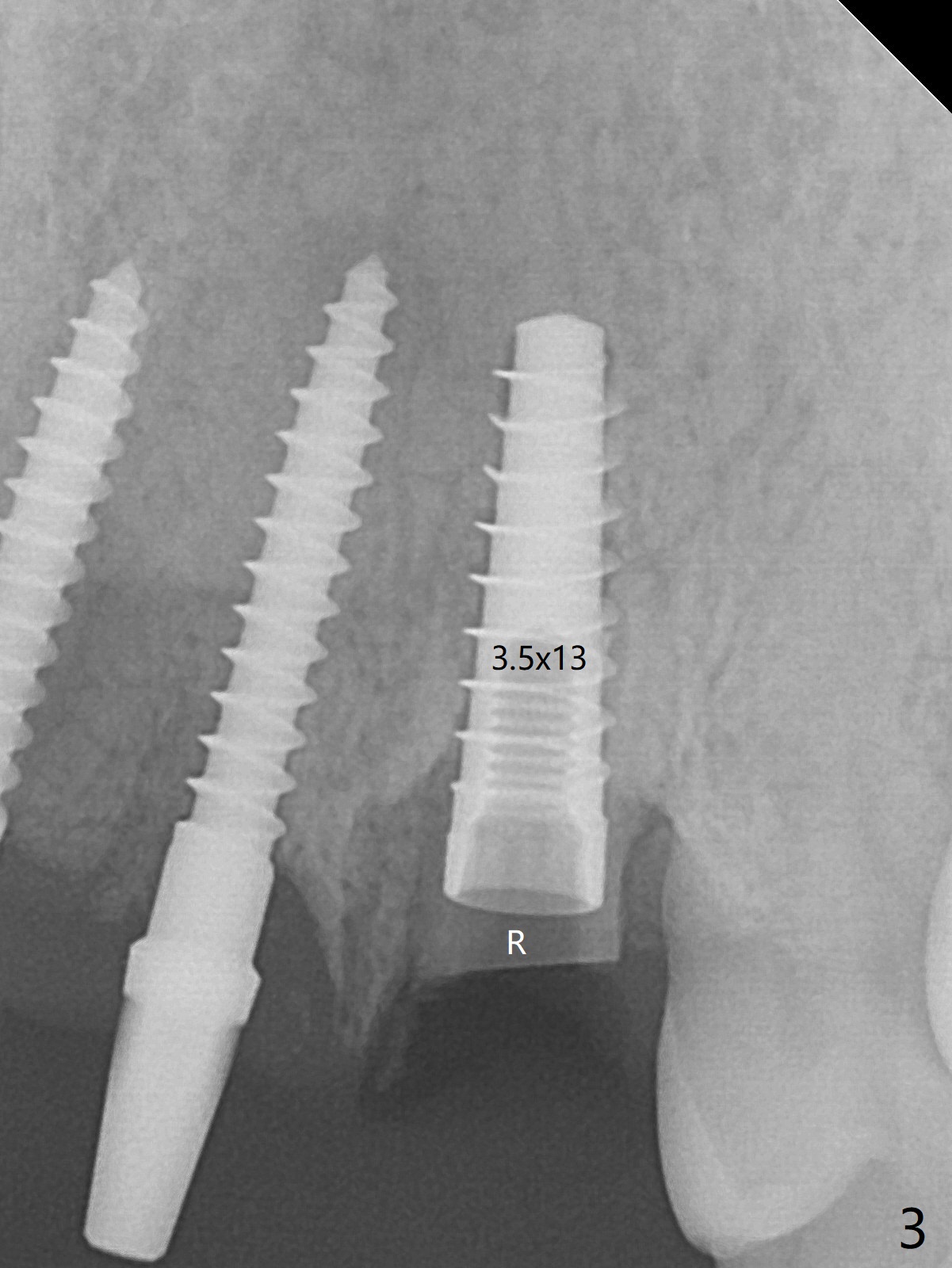
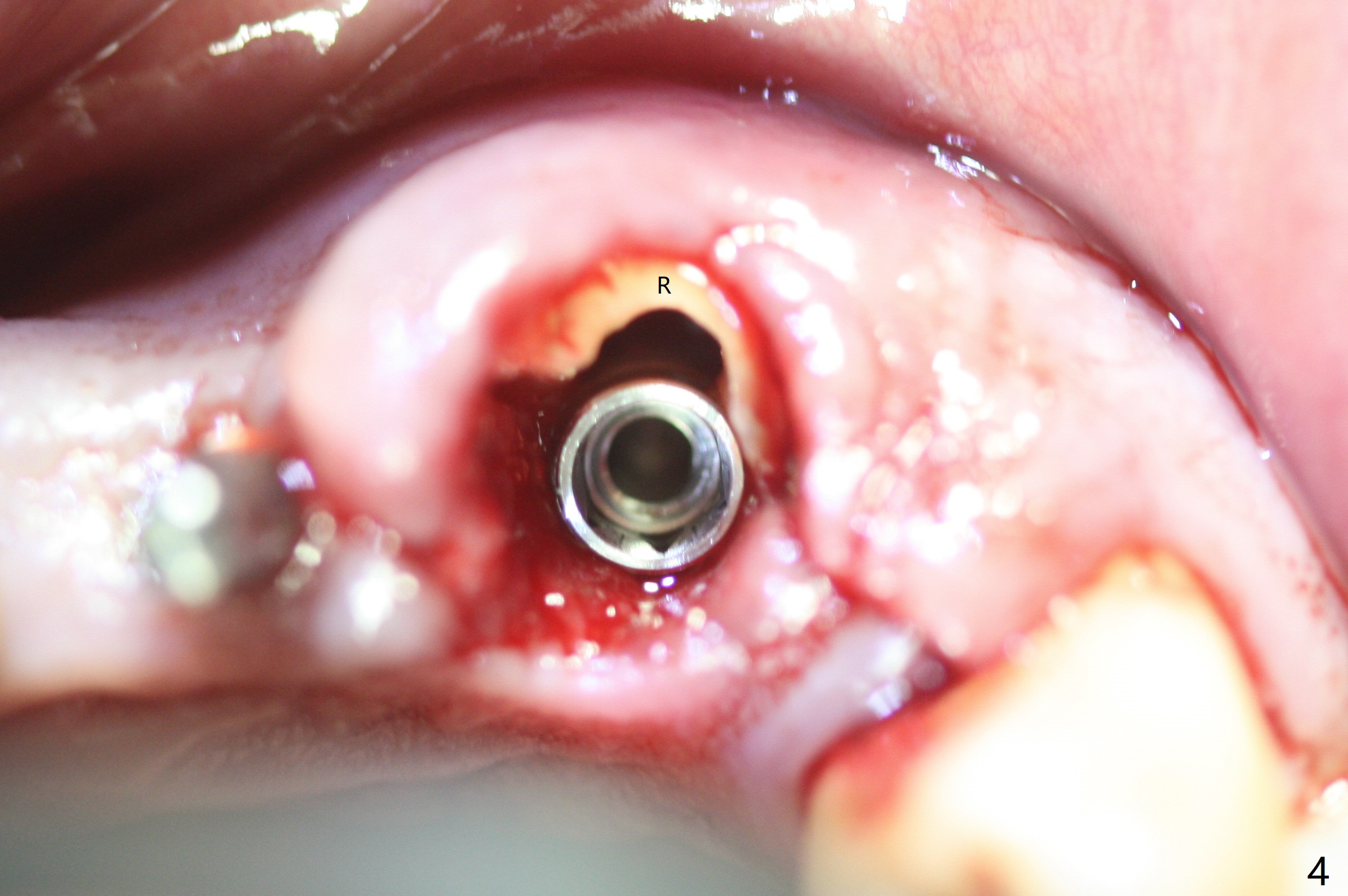
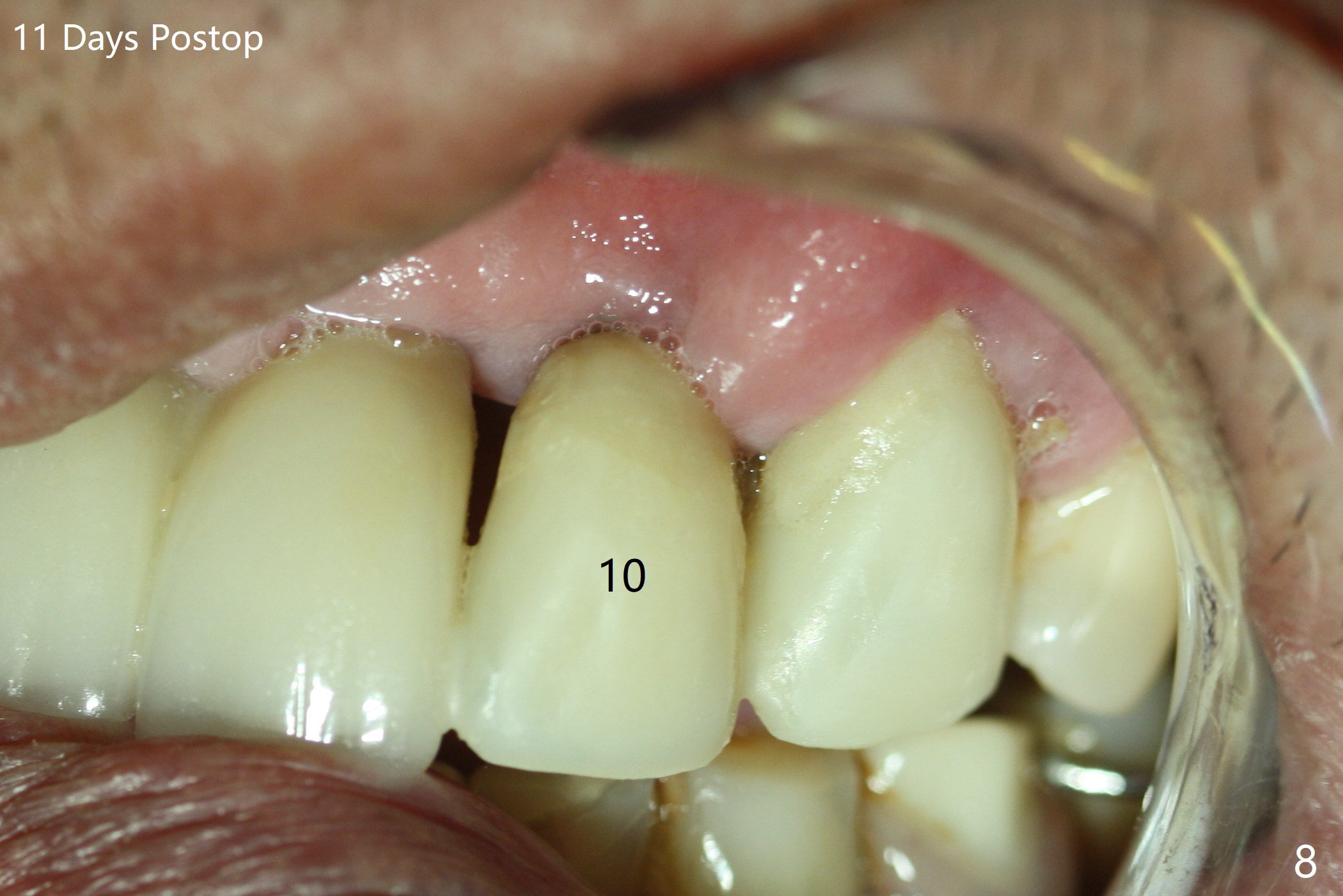
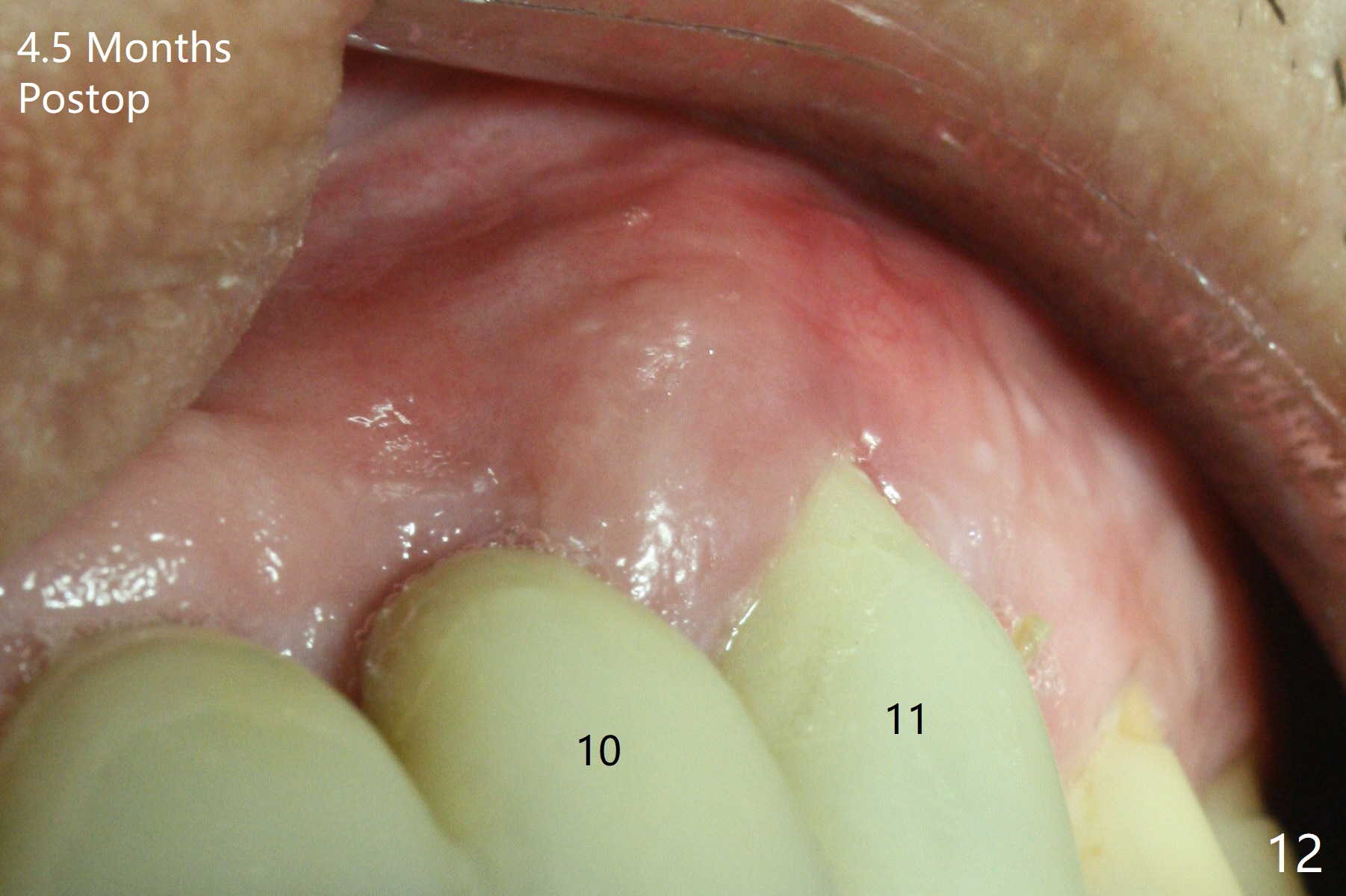
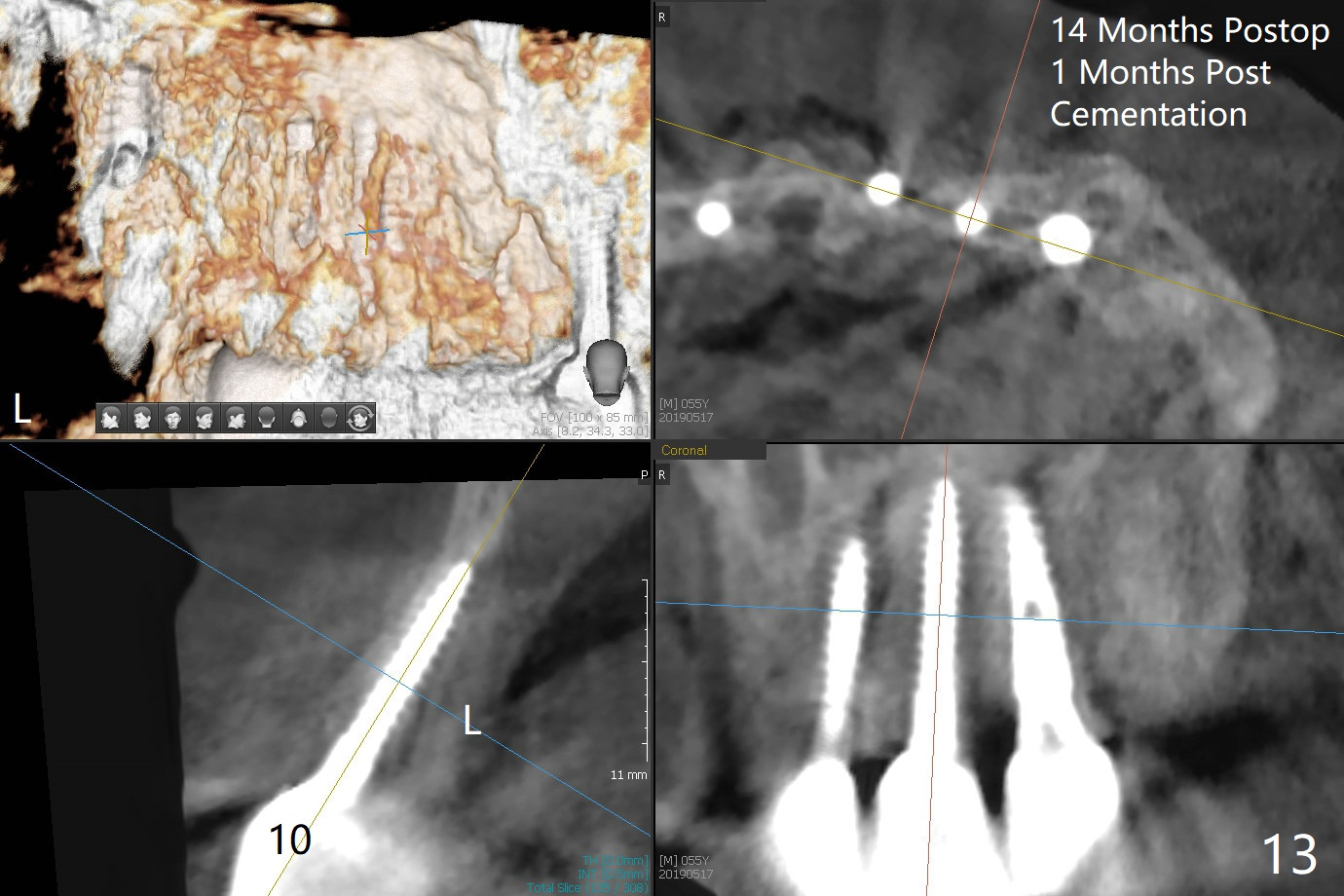
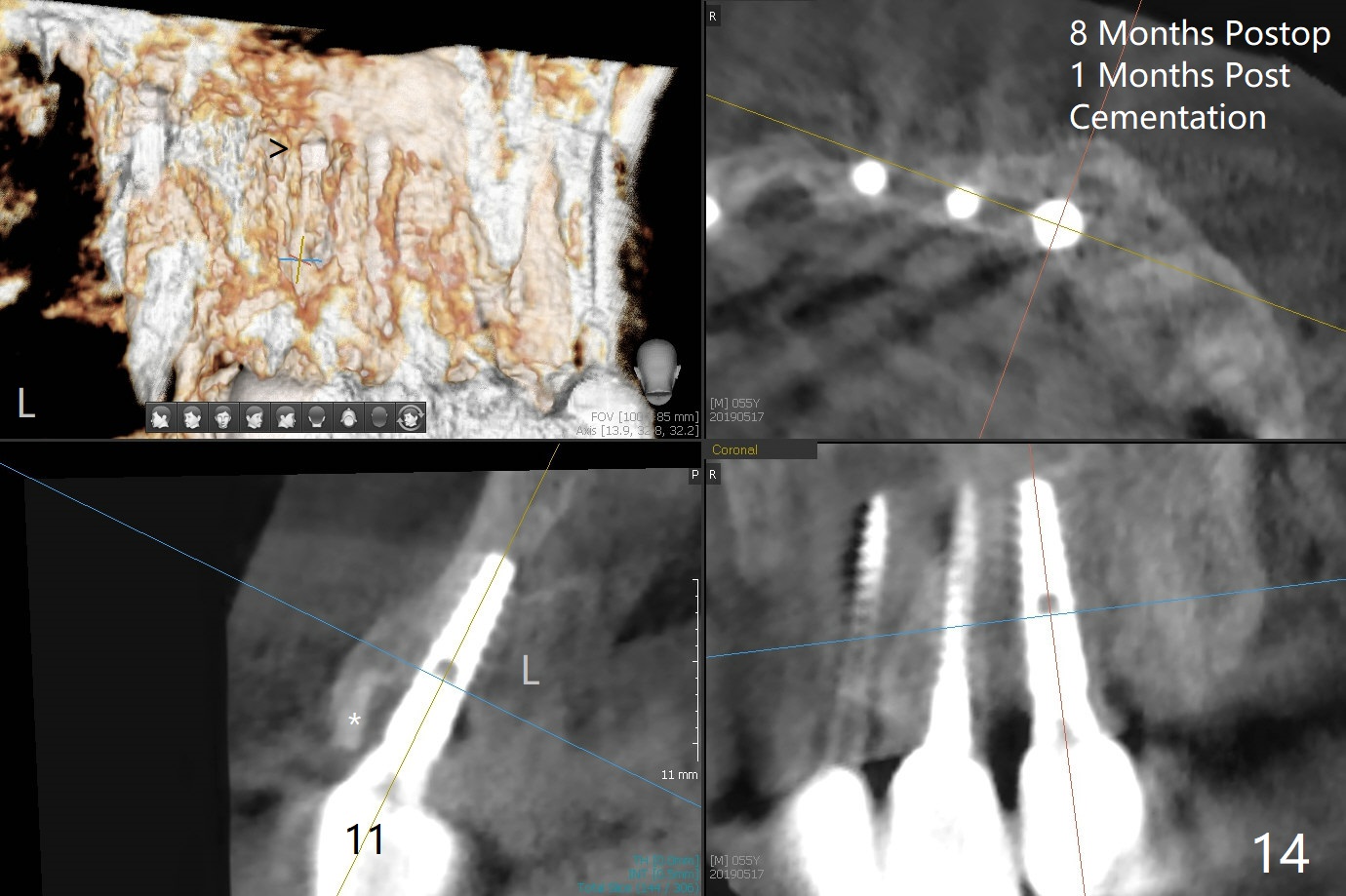
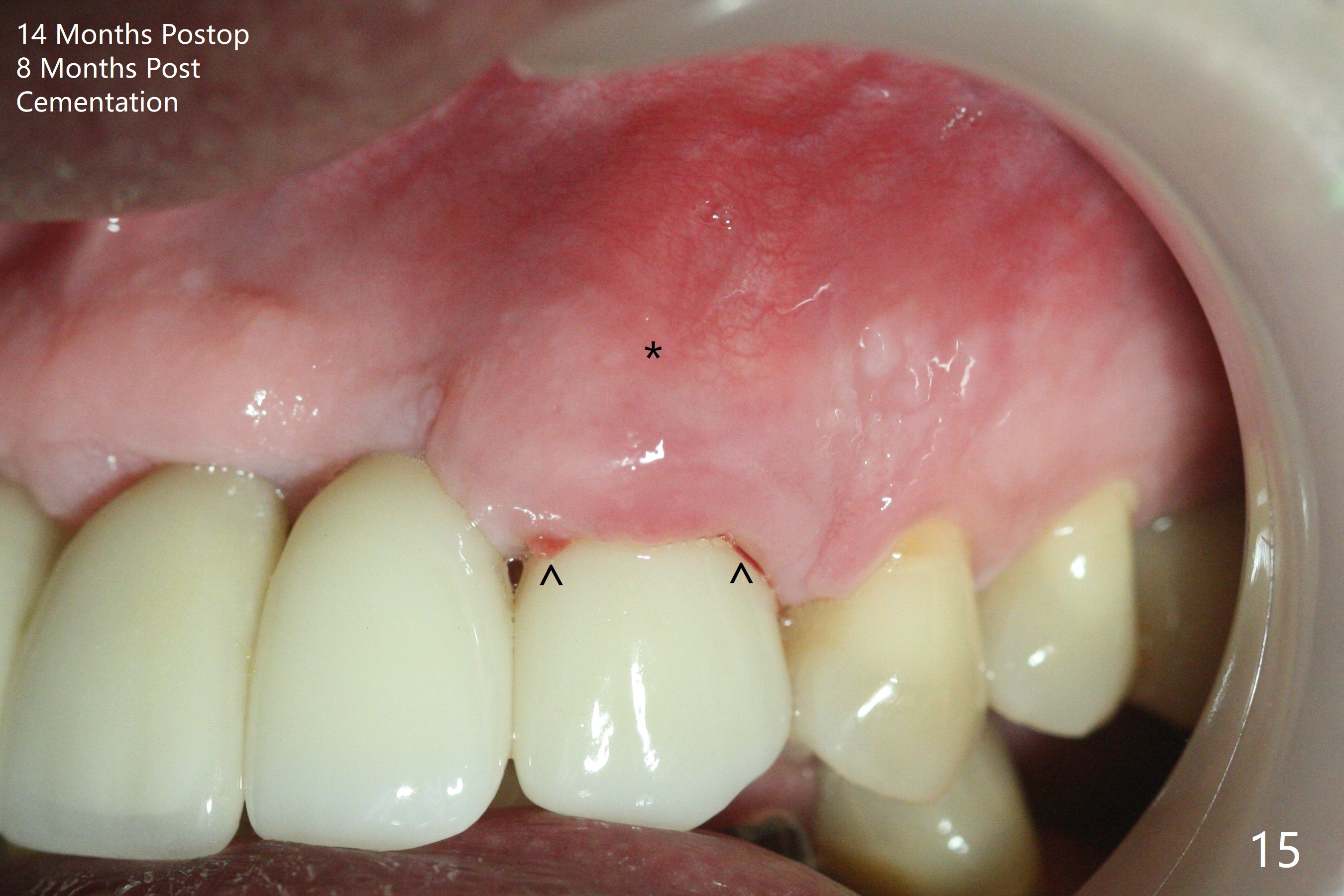
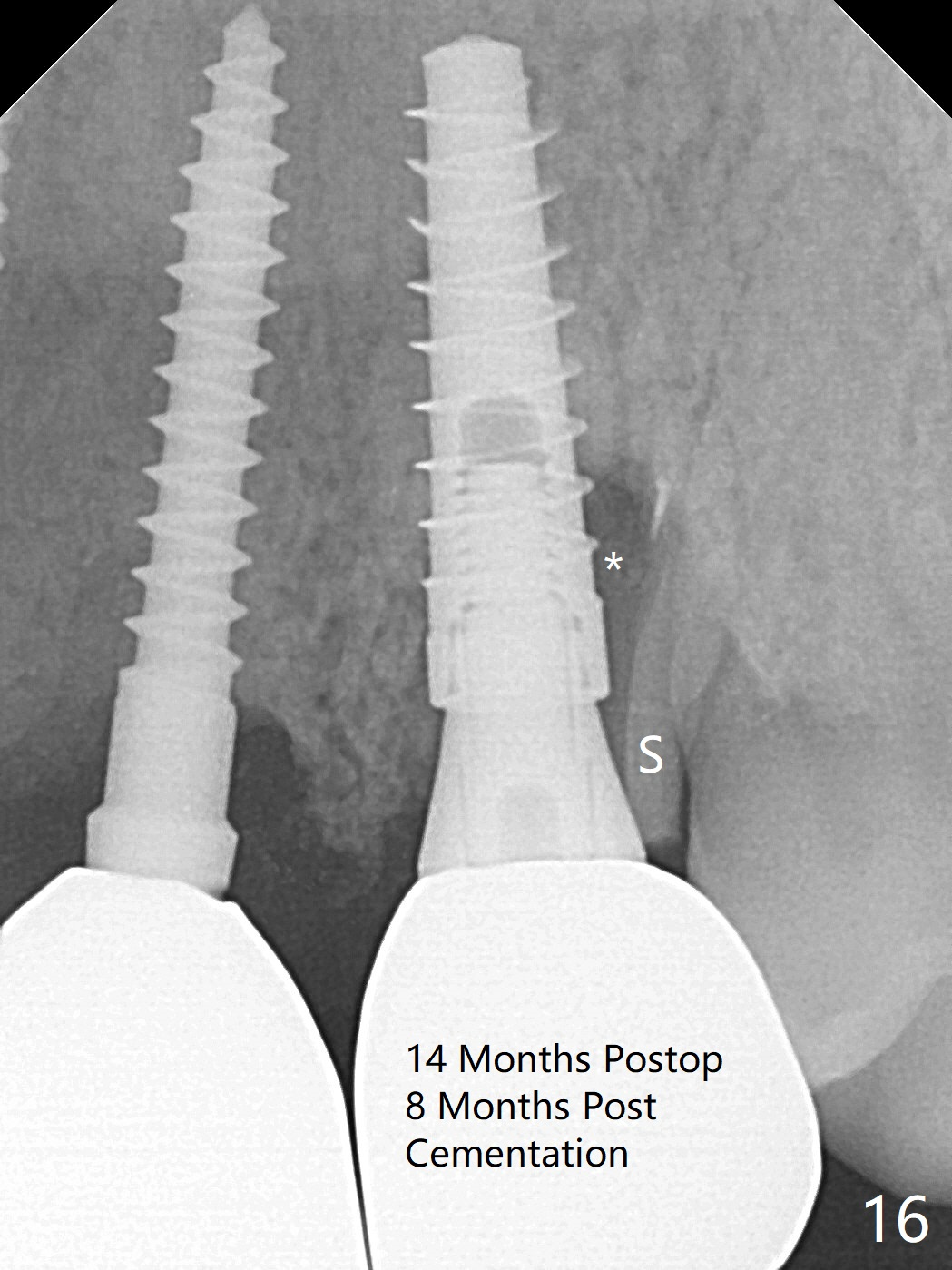
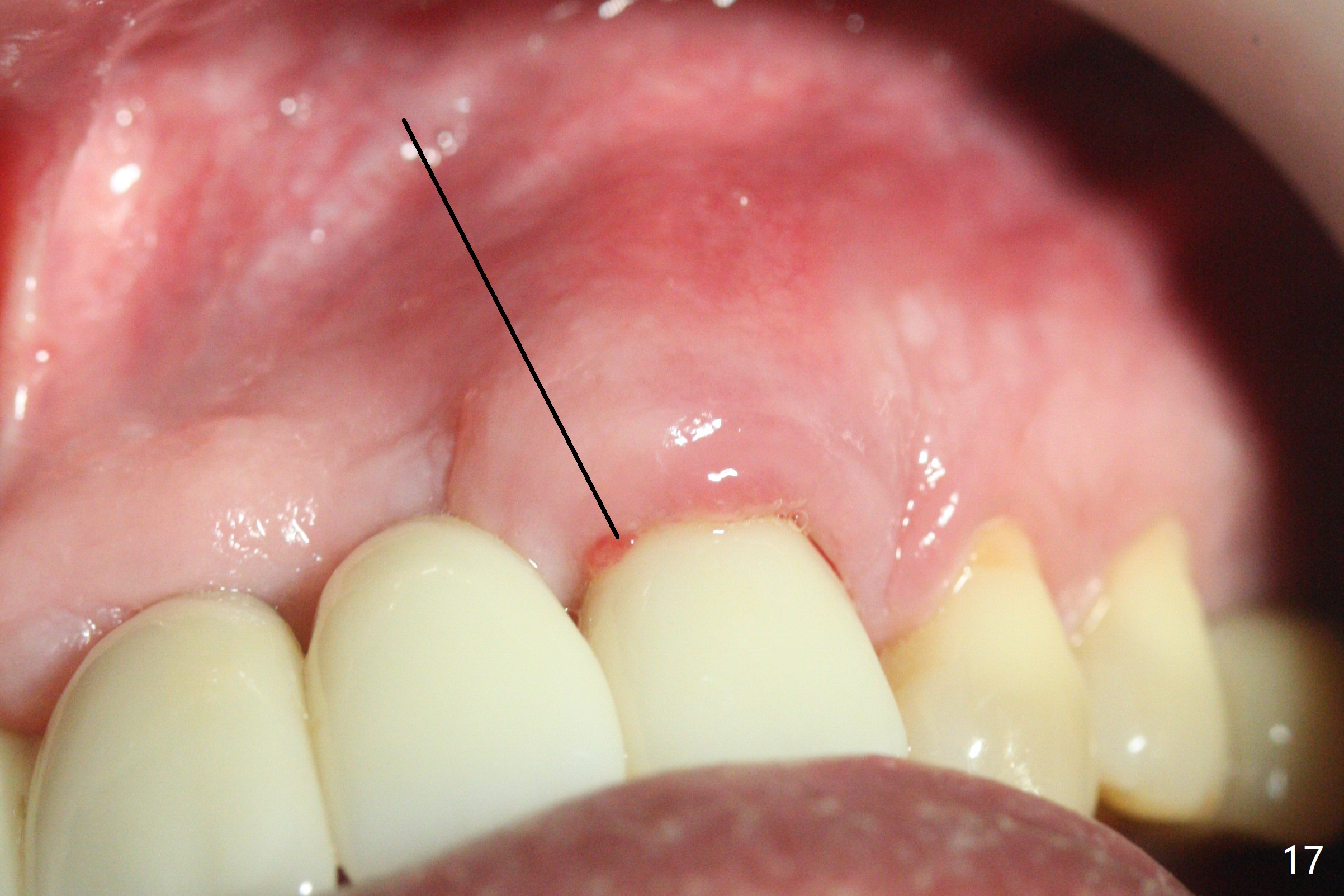
The buccal plate at #10 undergoes atrophy 9 months post immediate implant (Fig.1 *). To prevent the same post-extraction complication at #11, a technique called socket shield is going to be adopted. The buccal portion of the root (Fig.2-6 R, half-moon shaped) remains in place while a 3.5x13 mm implant is placed in the palatal portion of the socket (>50 Ncm). In fact the root is trimmed slightly subcrestal (Fig.6 C). It is assumed that there will be no or minimal bone resorption as long as the periosteum between the buccal plate and the remaining buccal root is not disturbed after tooth removal. After placement of a 4.5x15 degrees A (2mm) angled abutment and Vanilla graft (Fig.7 *), an immediate provisional is fabricated (using a central incisor crown form for #10 because of extra wide space of #11, Fig.8). There is no buccal plate atrophy at the canine 11 days postop (Fig.9). There is smooth transition from the grafted bone to the native bone 4.5 months postop (Fig.10). The buccal plate remains non-atrophic at the canine 4.5 months postop (Fig.11,12). CT taken 1 month post cementation shows that the implants at #10 and 11 are placed somewhat lingually (Fig.13,14 L (*: socket shield)). Gingival swelling is noted (Fig.15 *) with +Bleeding On Probing (^) 8 months post cementation (at the time of #21/24 impression). It appears that the socket shield (Fig.16 S) causes infection and loss of bone graft (*). The shield will be removed with an oblique accessory incision to save the papilla between #10 and 11 (Fig.17 black line). Prepare PRF for sticky bone (x1).
Return to Upper Canine Immediate Implant, Trajectory, No Antibiotic, Socket Shield 14/15 24/25 19/21/30 18/19 Xin Wei, DDS, PhD, MS 1st edition 09/28/2018, last revision 09/13/2020