|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
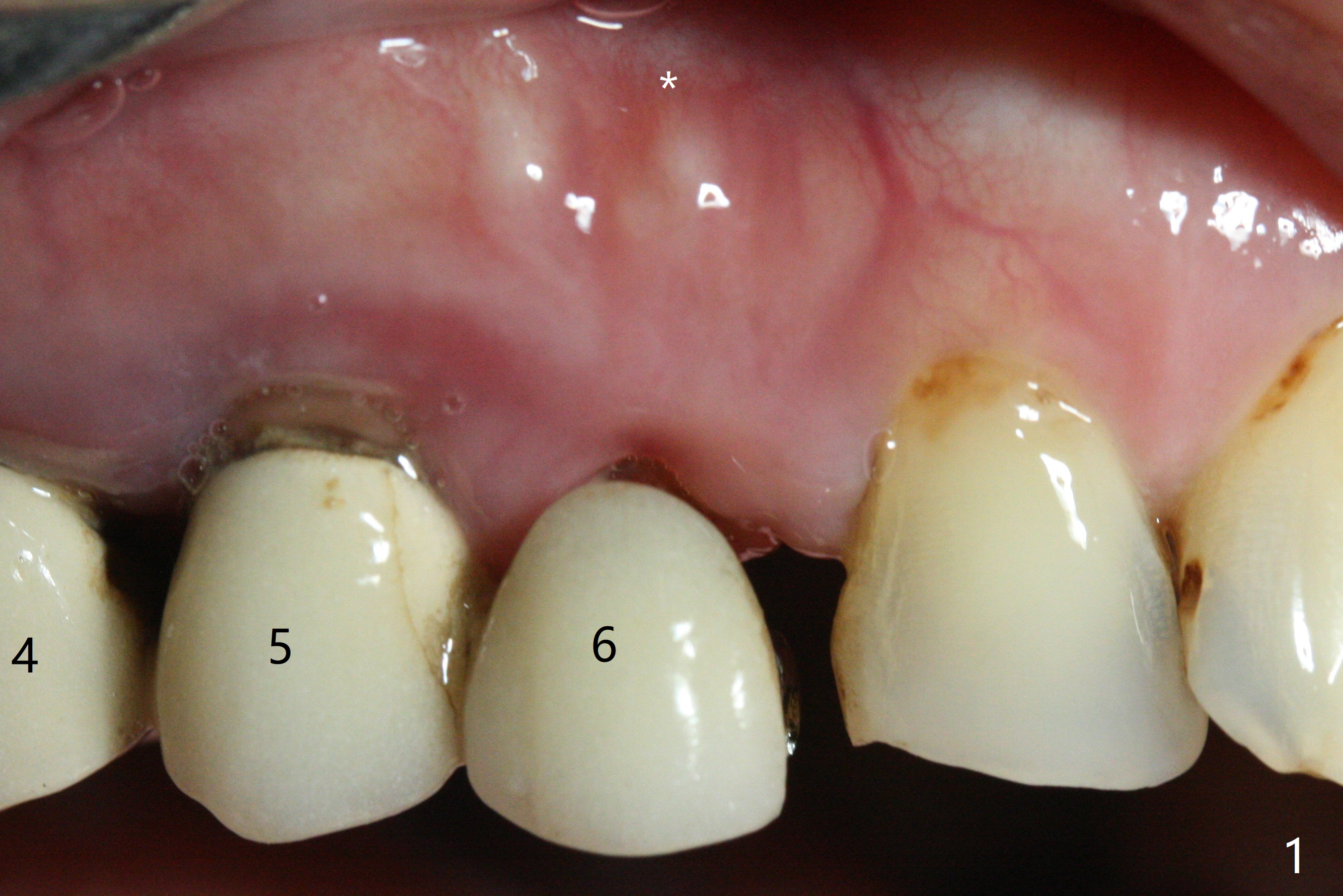
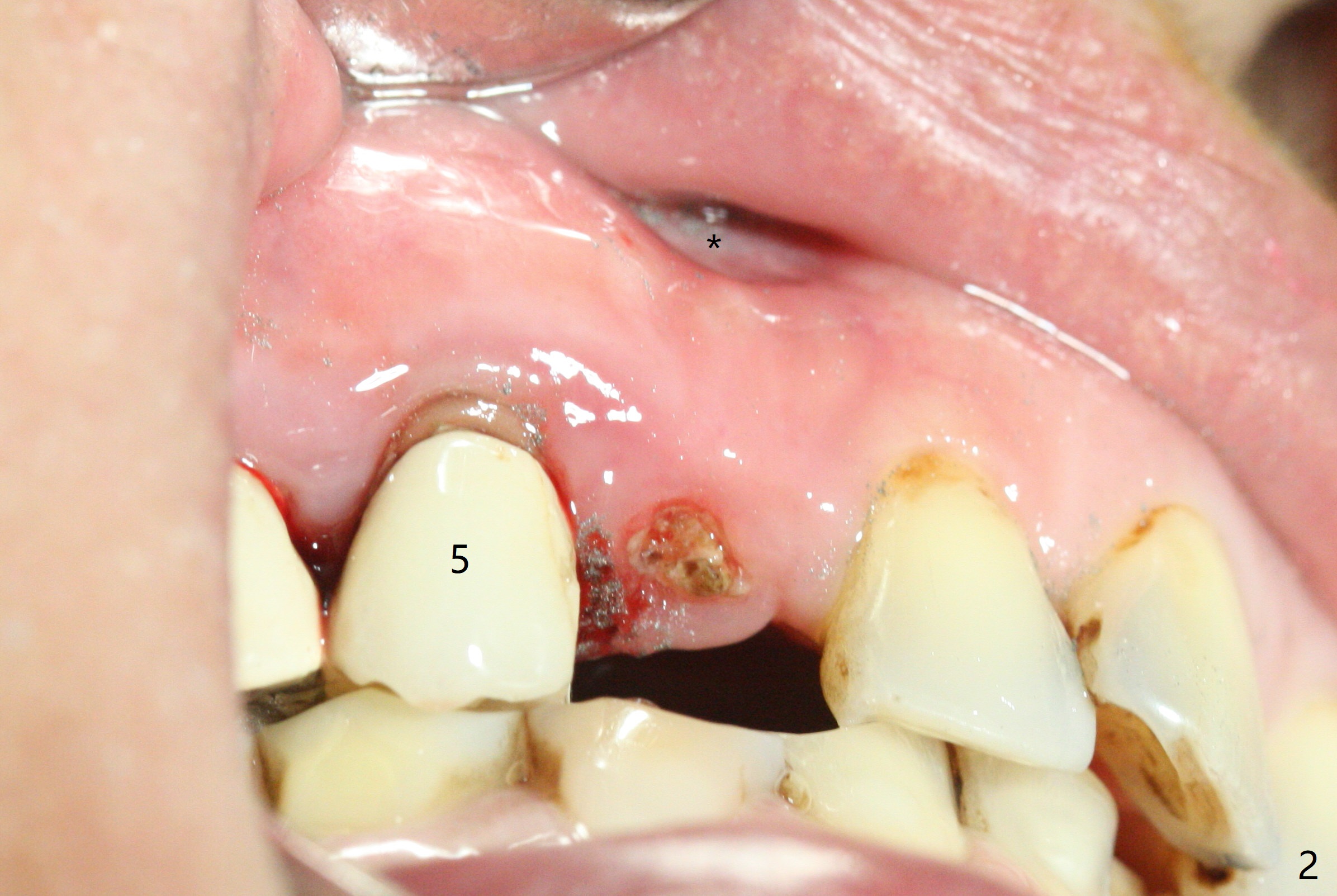
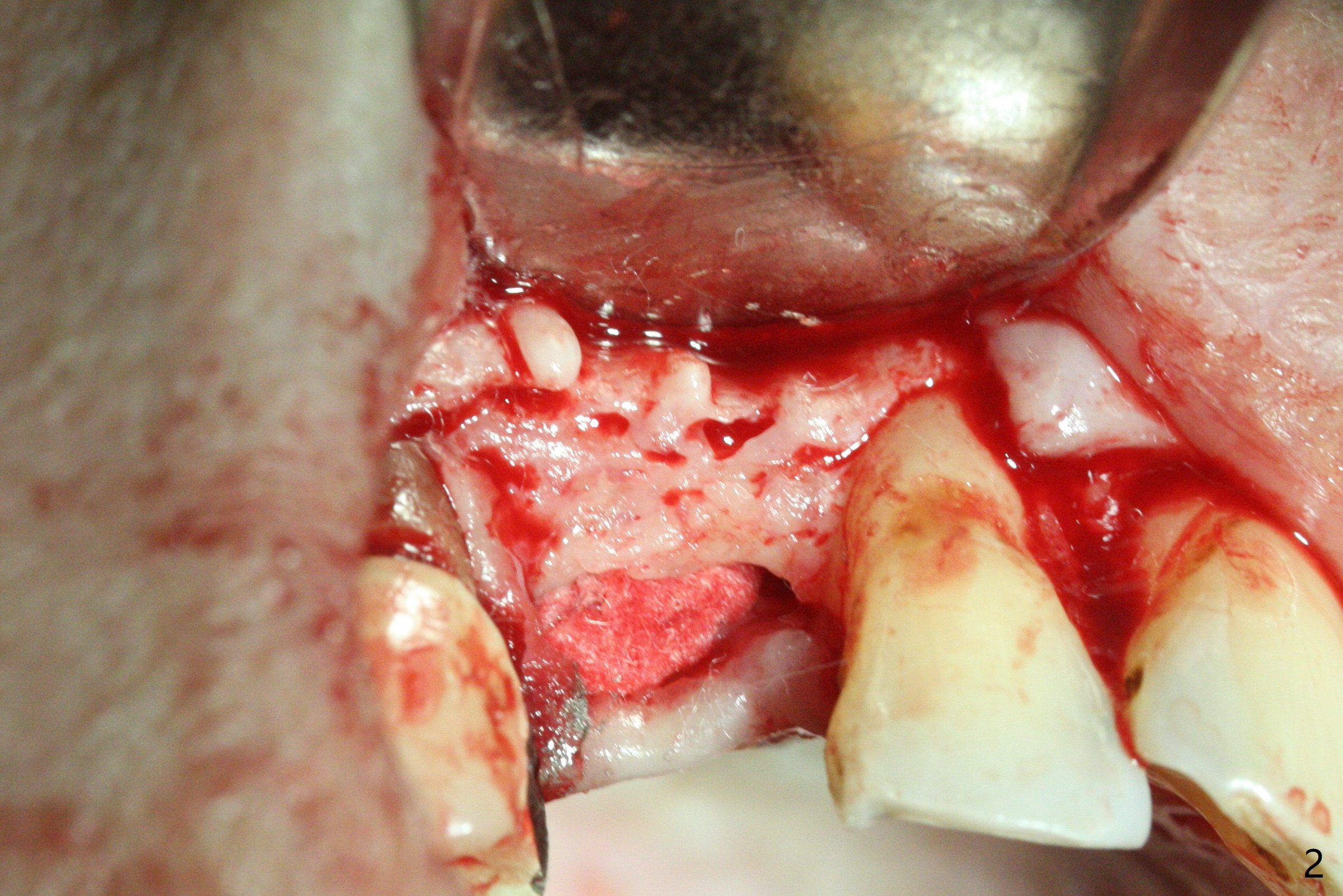
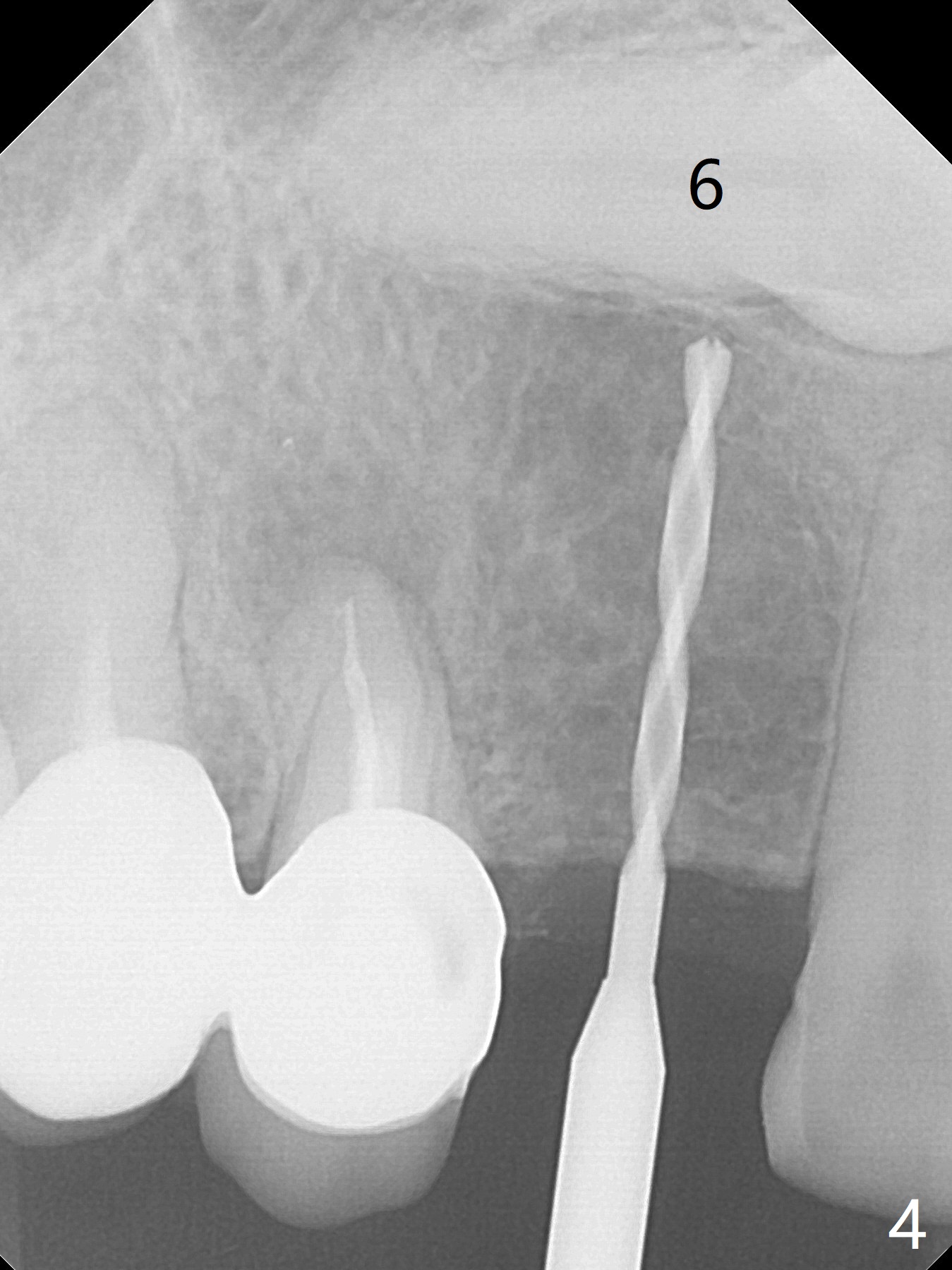
Buccal Concavity
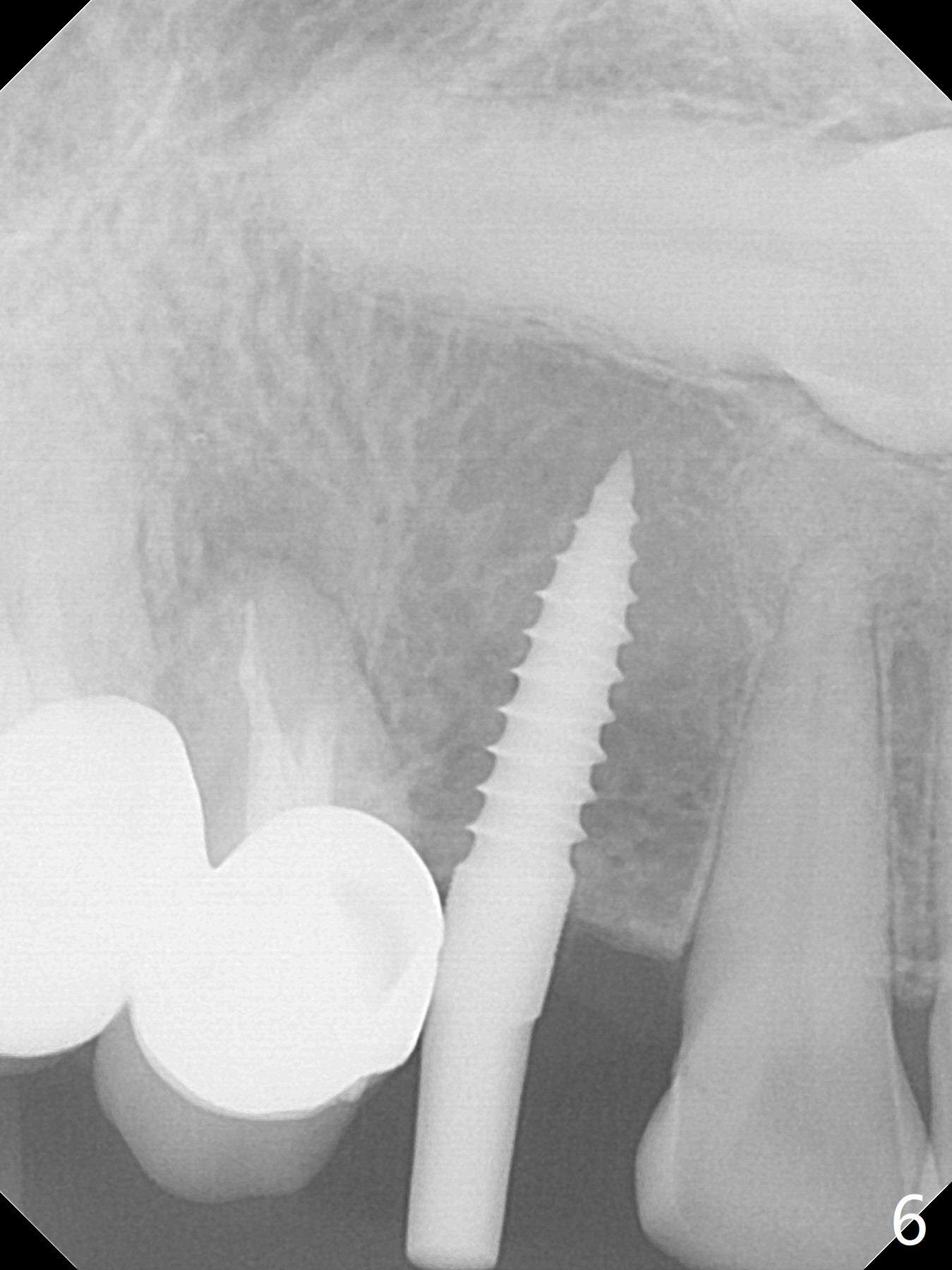
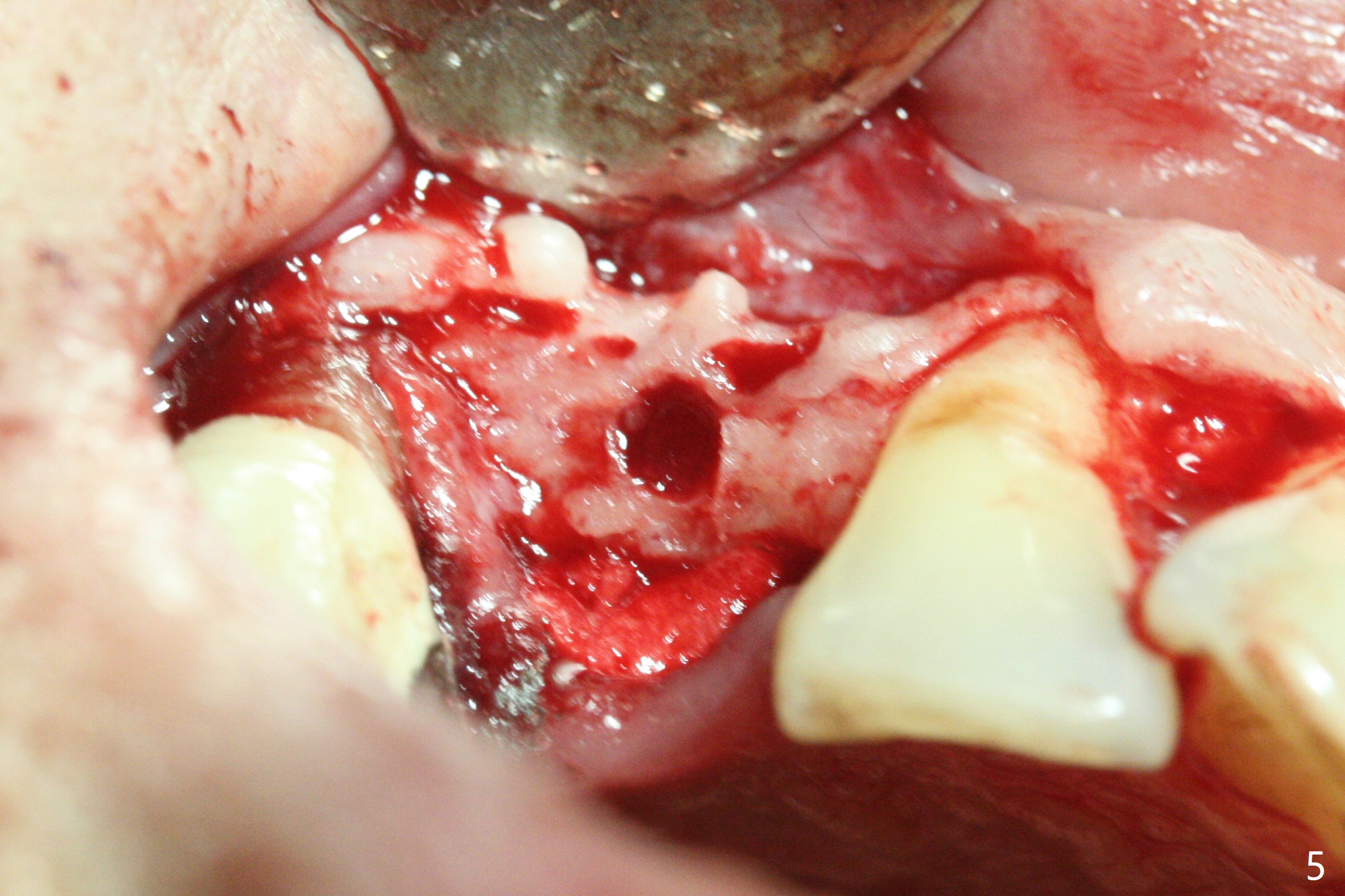
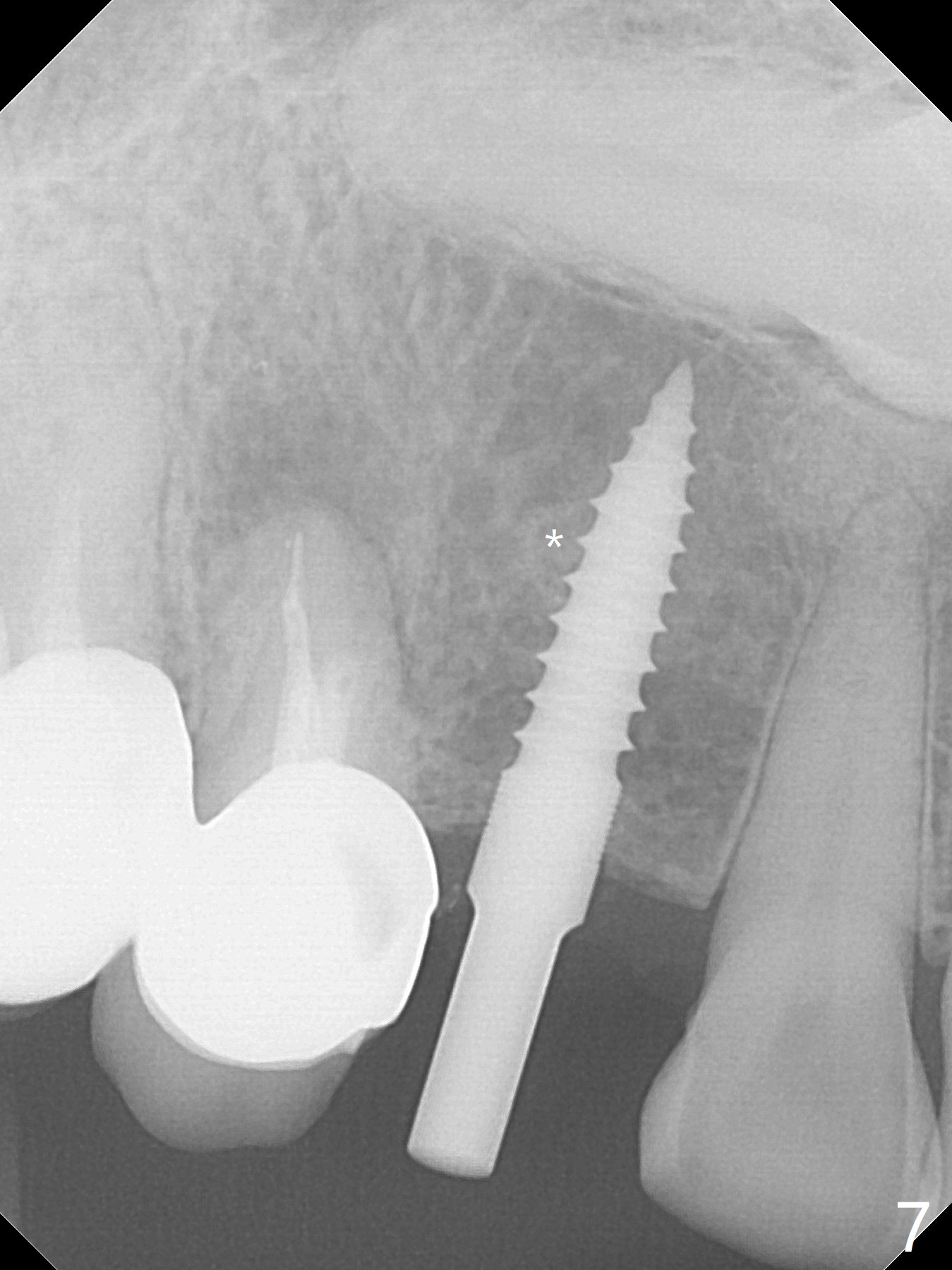
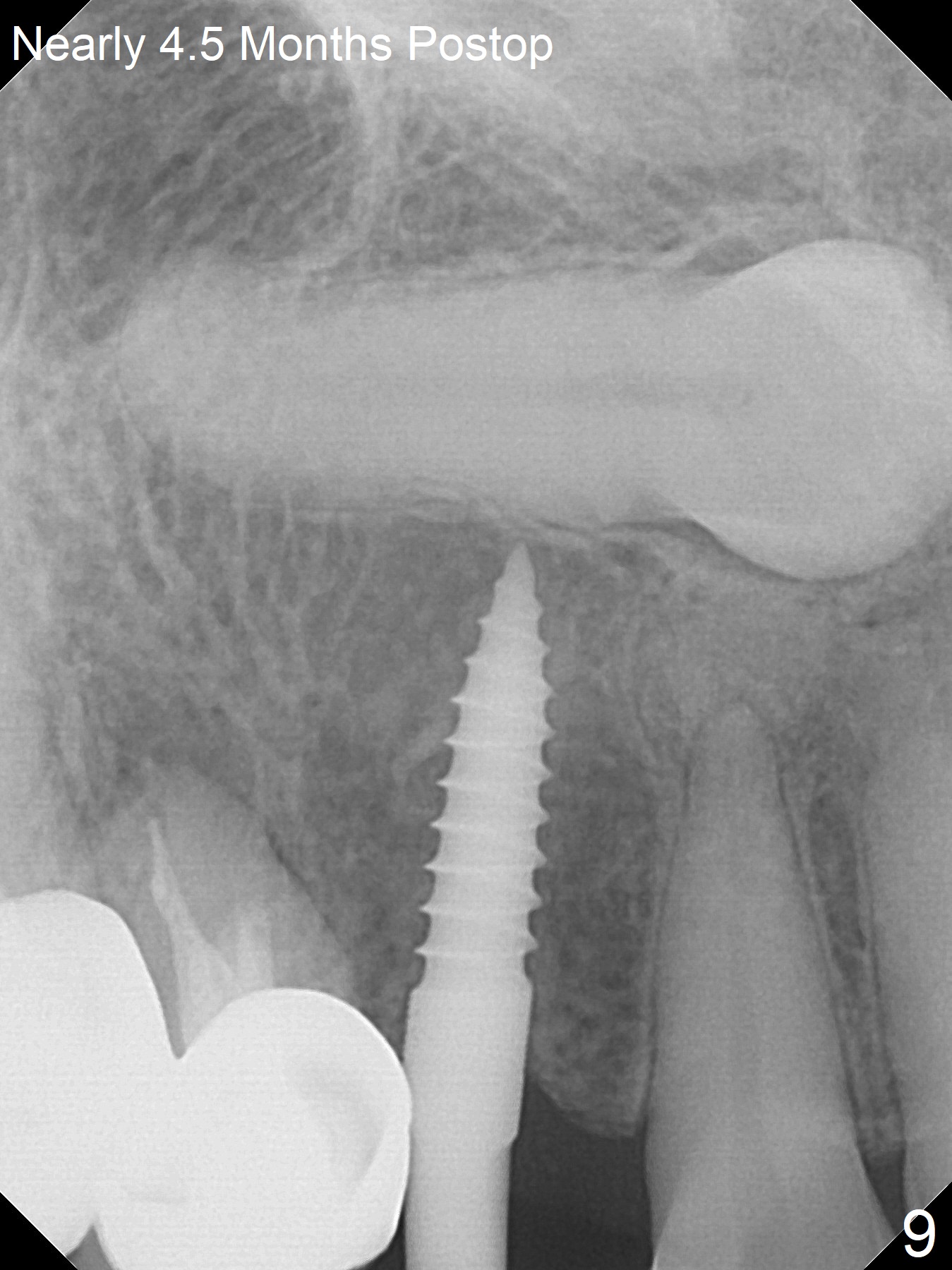
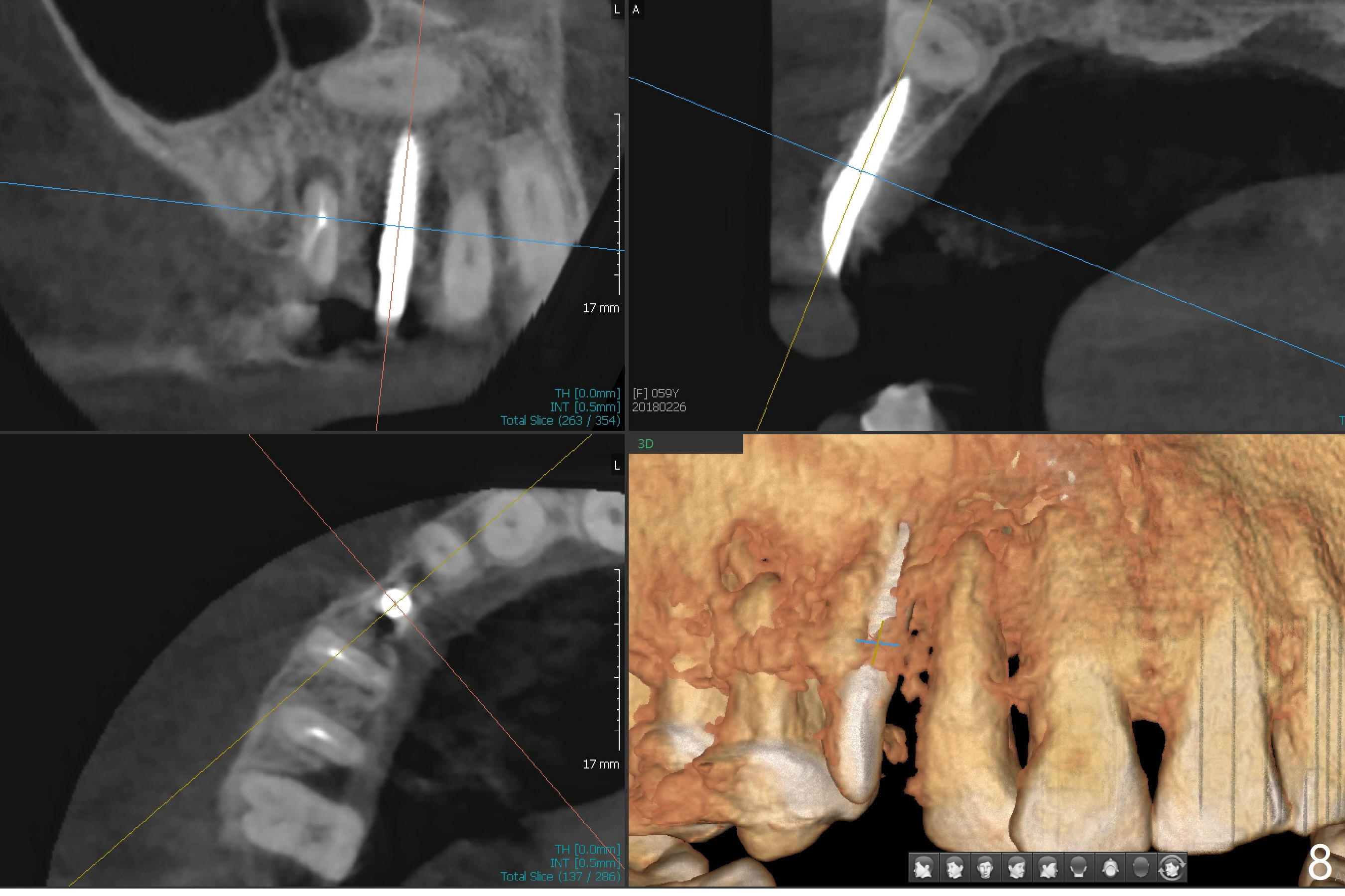
After removal the pontic of a cantilever FPD (Fig.1), a residual root is found at #6 with the buccal concavity (Fig.2 *). The ridge is narrow with flap elevation (Fig.3). PA taken with a 1.2 mm drill for 14 mm shows a horizontally impacted canine (Fig.4: #6). When the osteotomy is finished without apparently buccal perforation (Fig.5), the trajectory is buccal. When a 3x14 mm (12.5 mm in bone) 15 degree angled 1-piece implant is placed with normal trajectory (Fig.6), the buccal plate is perforated. As the implant is redirected so that the apical end of the implant does not stick out buccally, the trajectory returns buccal (Fig.7). The buccal aspect of the abutment is heavily reduced for an immediate provisional. The perforation is repaired with Vanilla Graft and Collagen Dressing before suturing. CT should have been taken preoperatively; the osteotomy should have been initiated as palatal as possible, as compared to that in Fig.5. When the 1st drill is used. it should be checked for restoration. An angled abutment does not help the trajectory substantially. The implant is loose 1.5 months (partially due to mastication); after retightening, CT is taken (Fig.8). The implant is within the bone. If the implant becomes loose again, extract the impacted canine and place the longest implant (22 mm) palatally. The implant is stable nearly 4.5 months postop (Fig.9). The patient is not satisfied with buccally-placed crown. The implant is removed with bone graft 6 months postop.
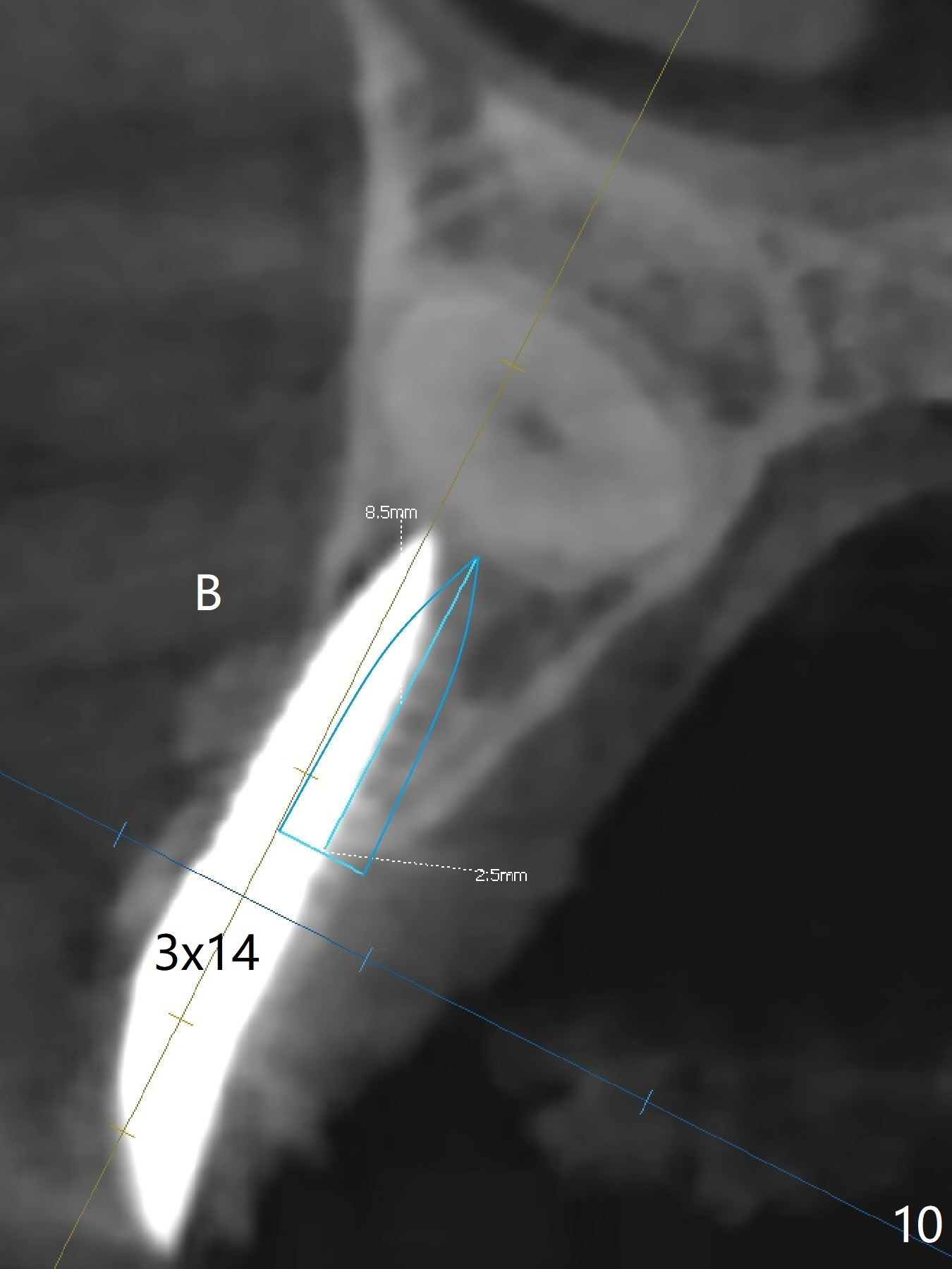
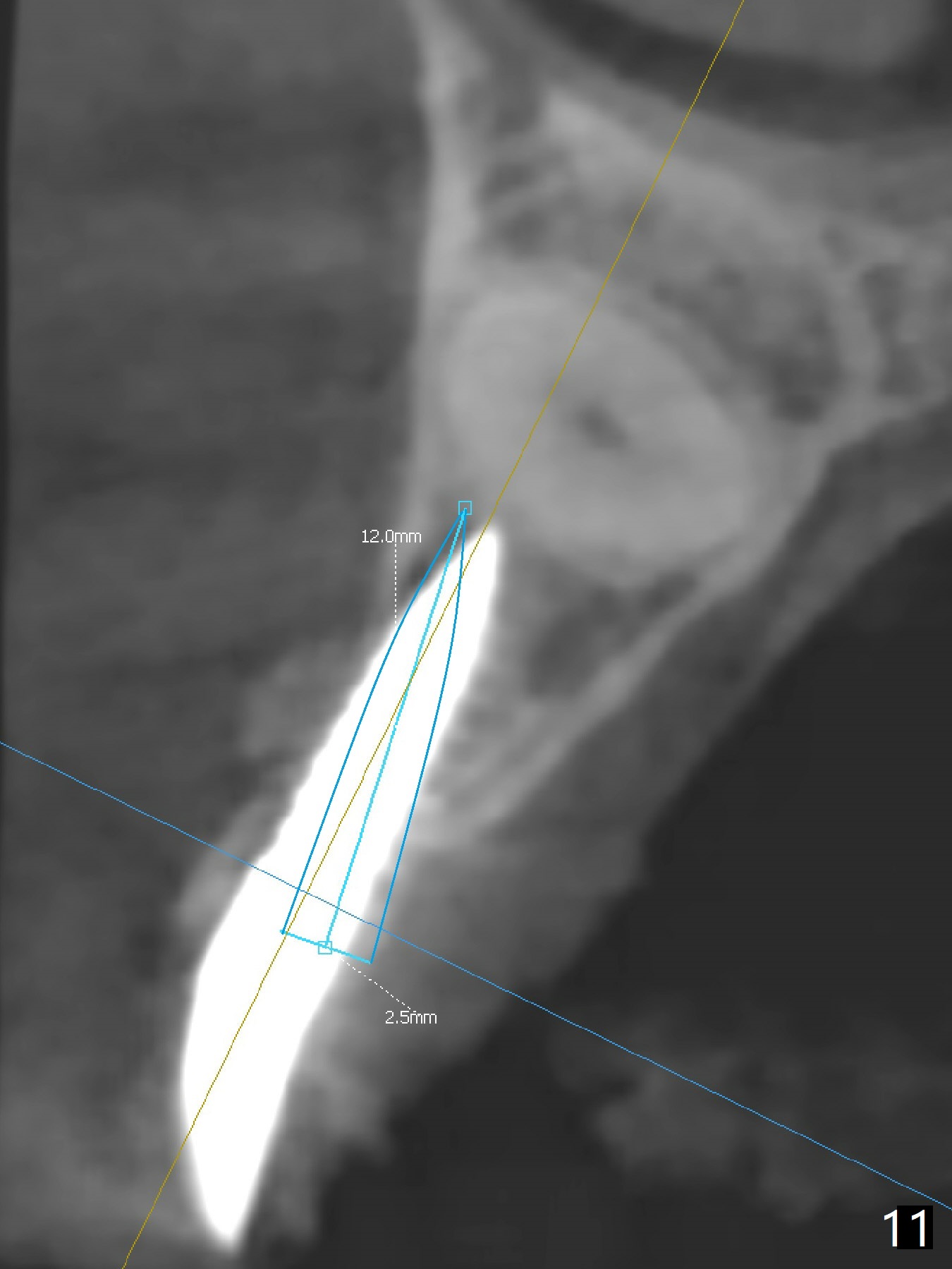
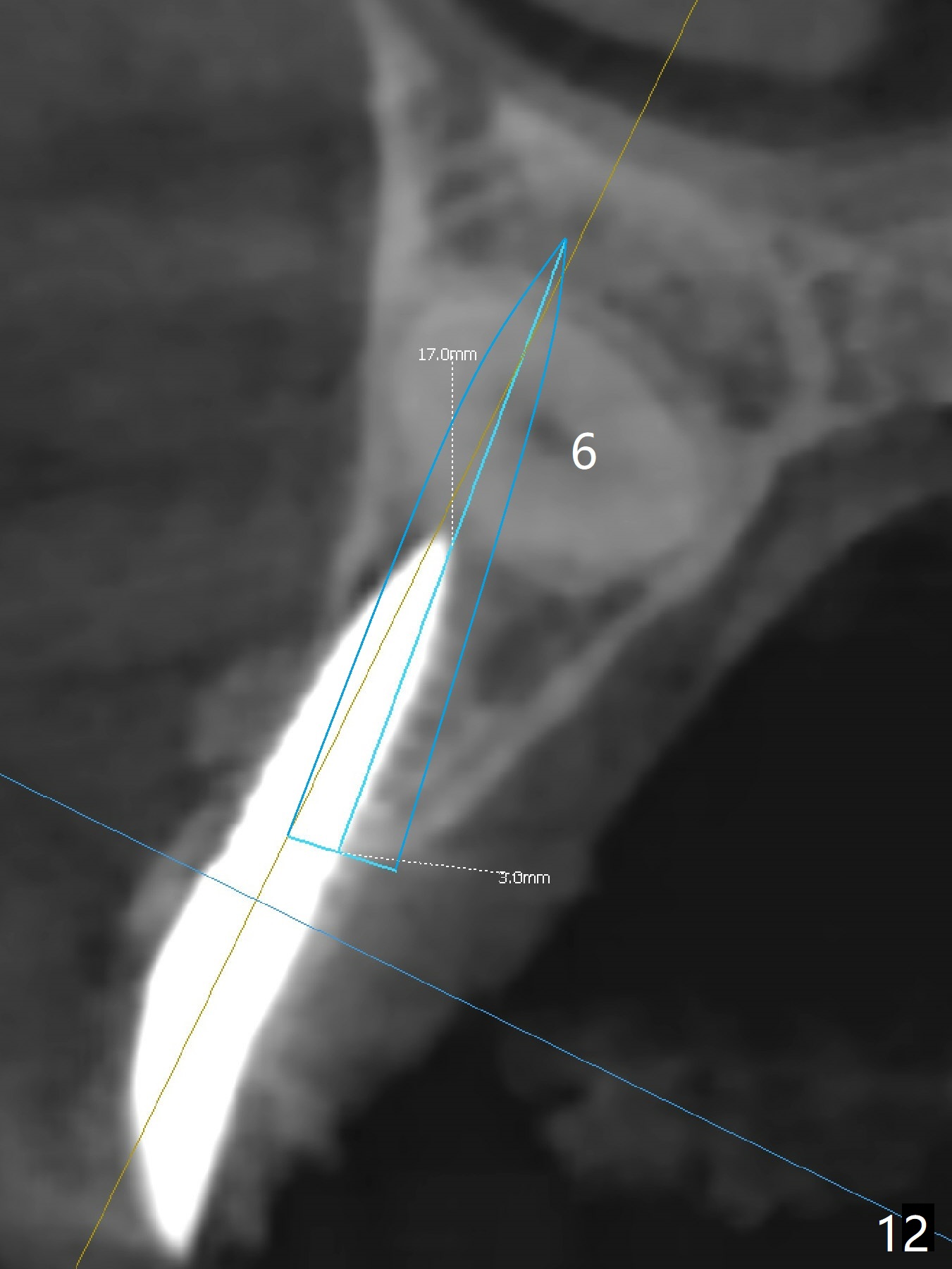
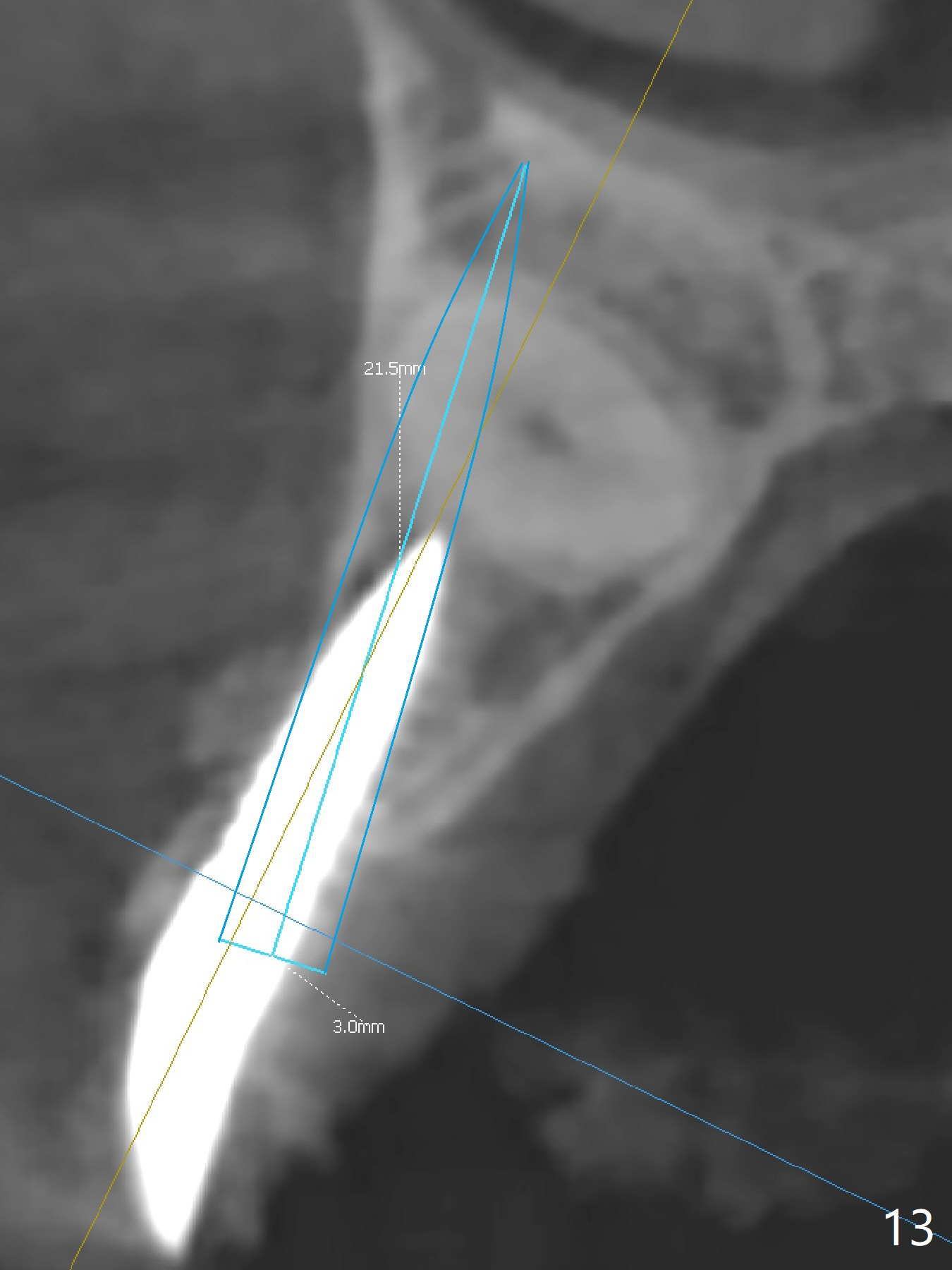
With 4-5 month healing, an implant should be placed as palatal as possible. The crest is ambiguous (compare Fig.10,11), the length of the implant being different. If the patient agrees with #6 extraction, stability will be more secure (Fig.12,13). Take 5x5 CT preop to solve the ambiguous crestal level issue.
Return to Upper Canine Immediate Implant, Armaments #2 修复 Xin Wei, DDS, PhD, MS 1st edition 01/12/2018, last revision 06/16/2021