










|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Limited Ortho with Proximal
Reduction
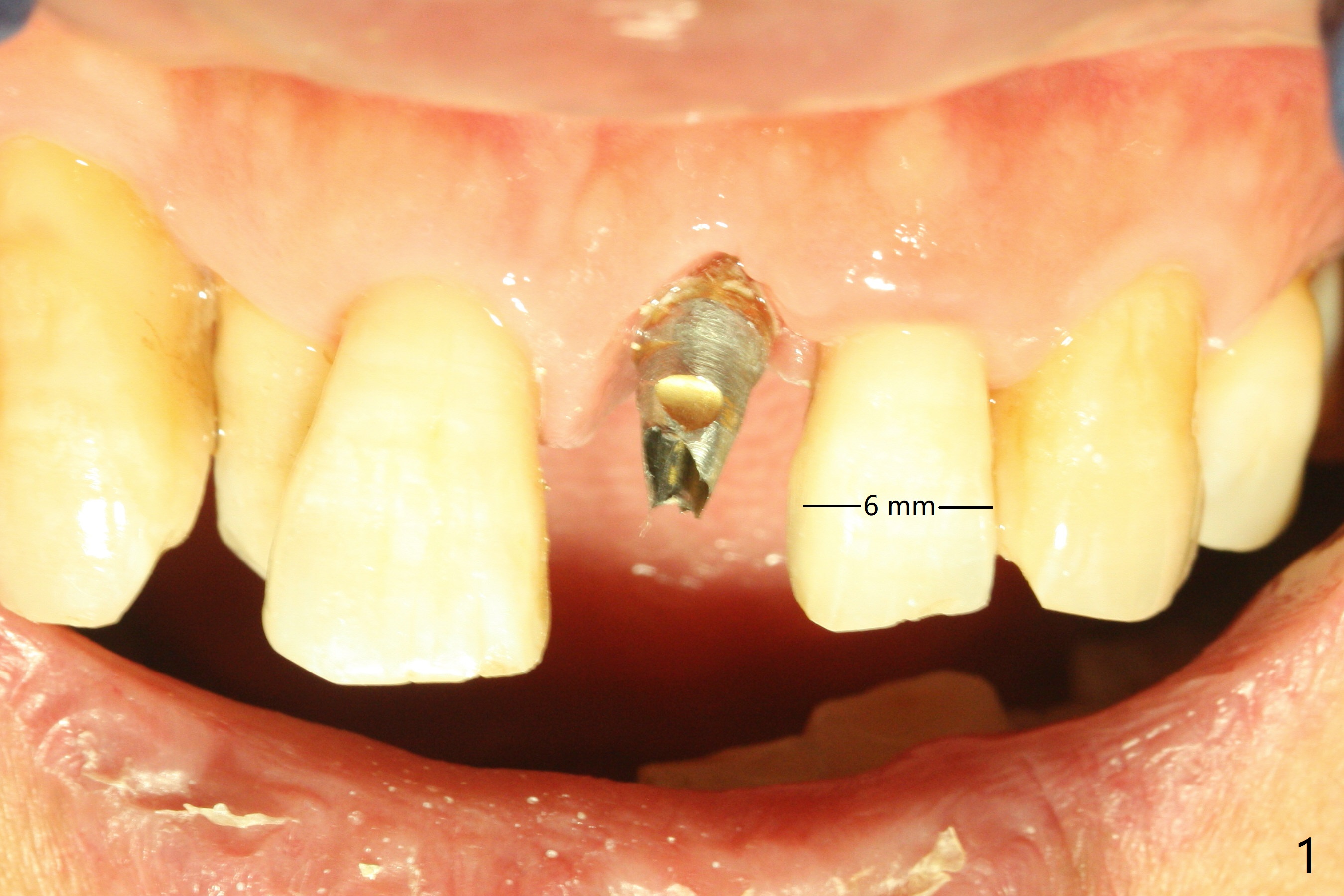
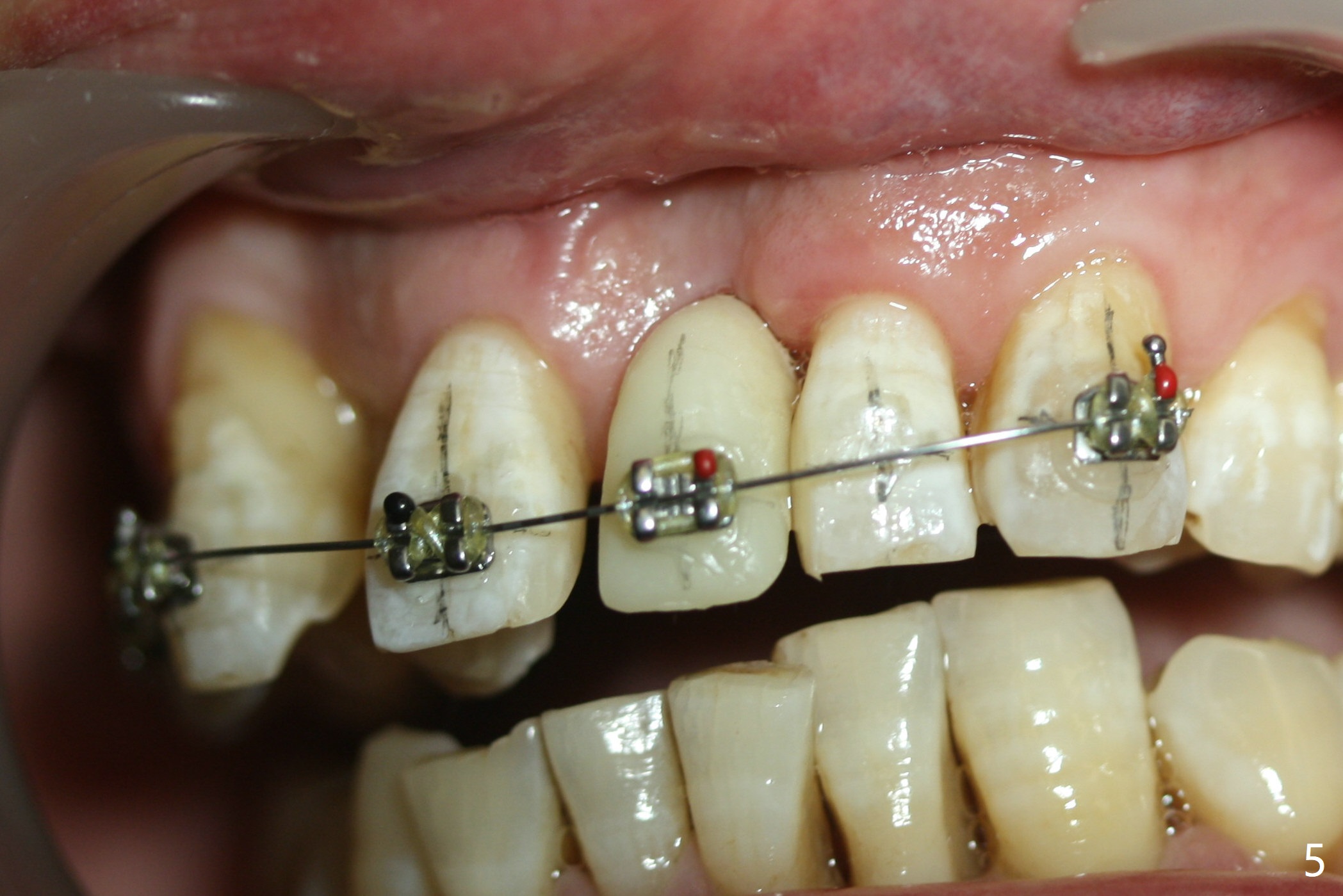
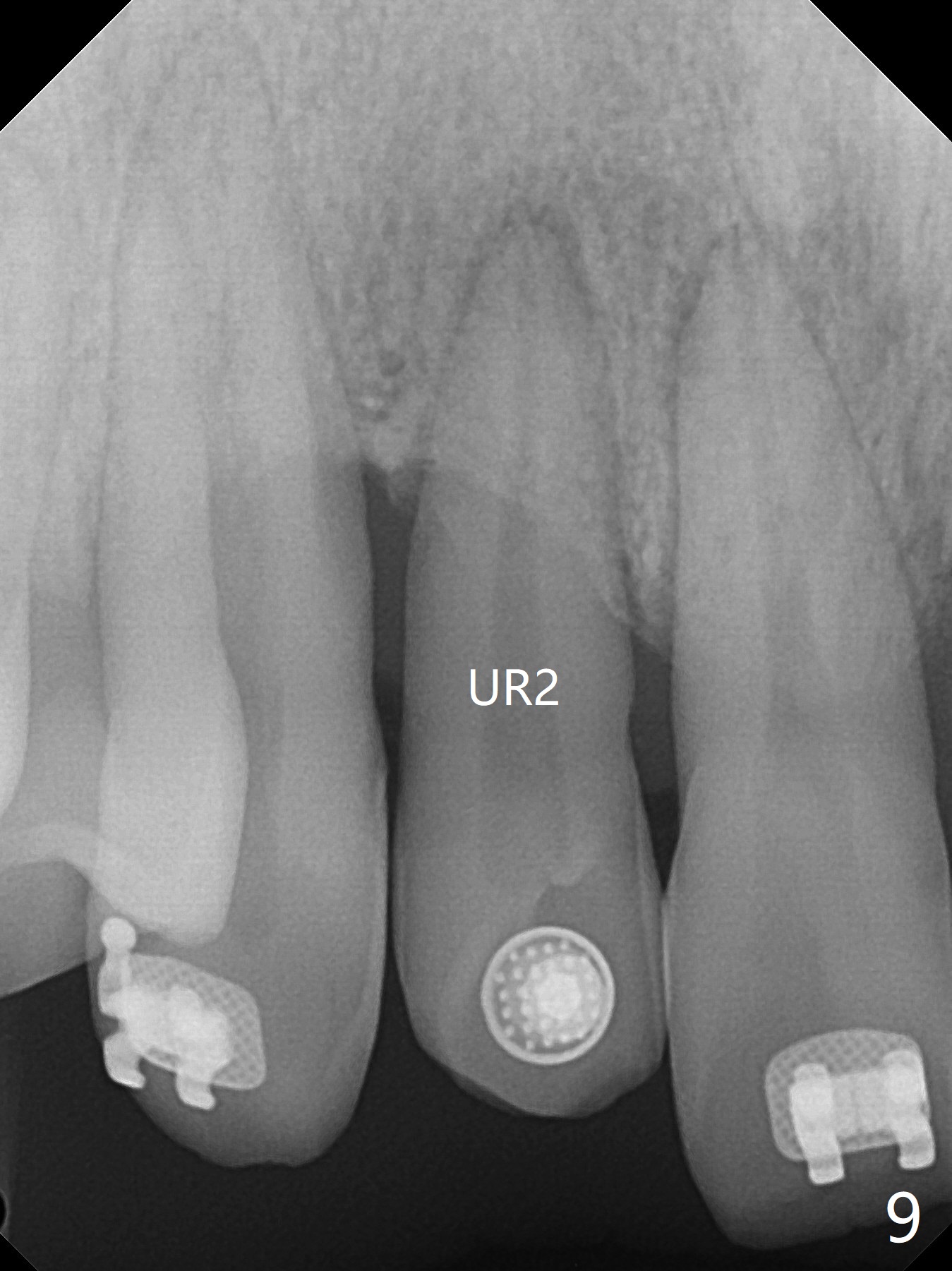
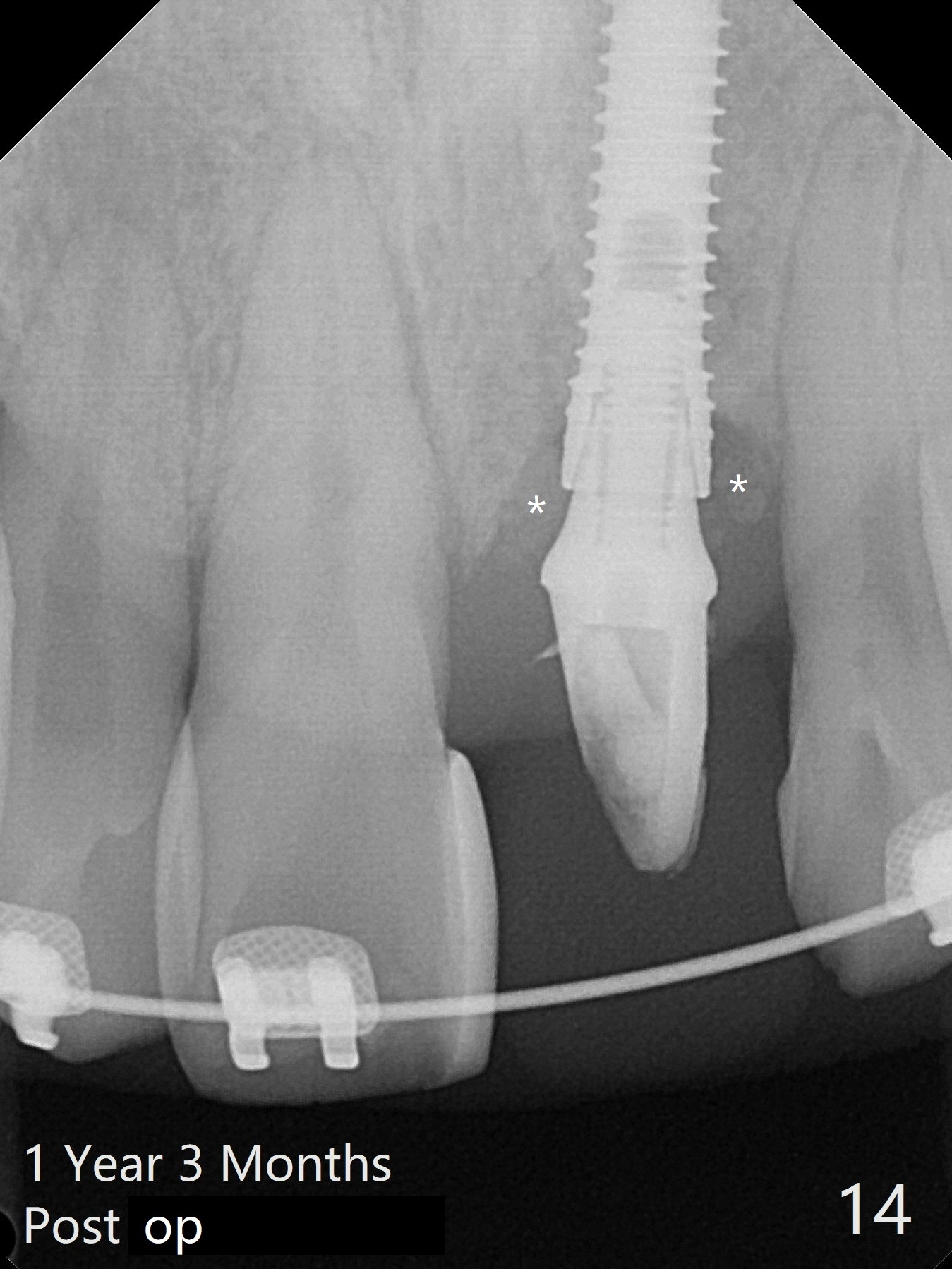
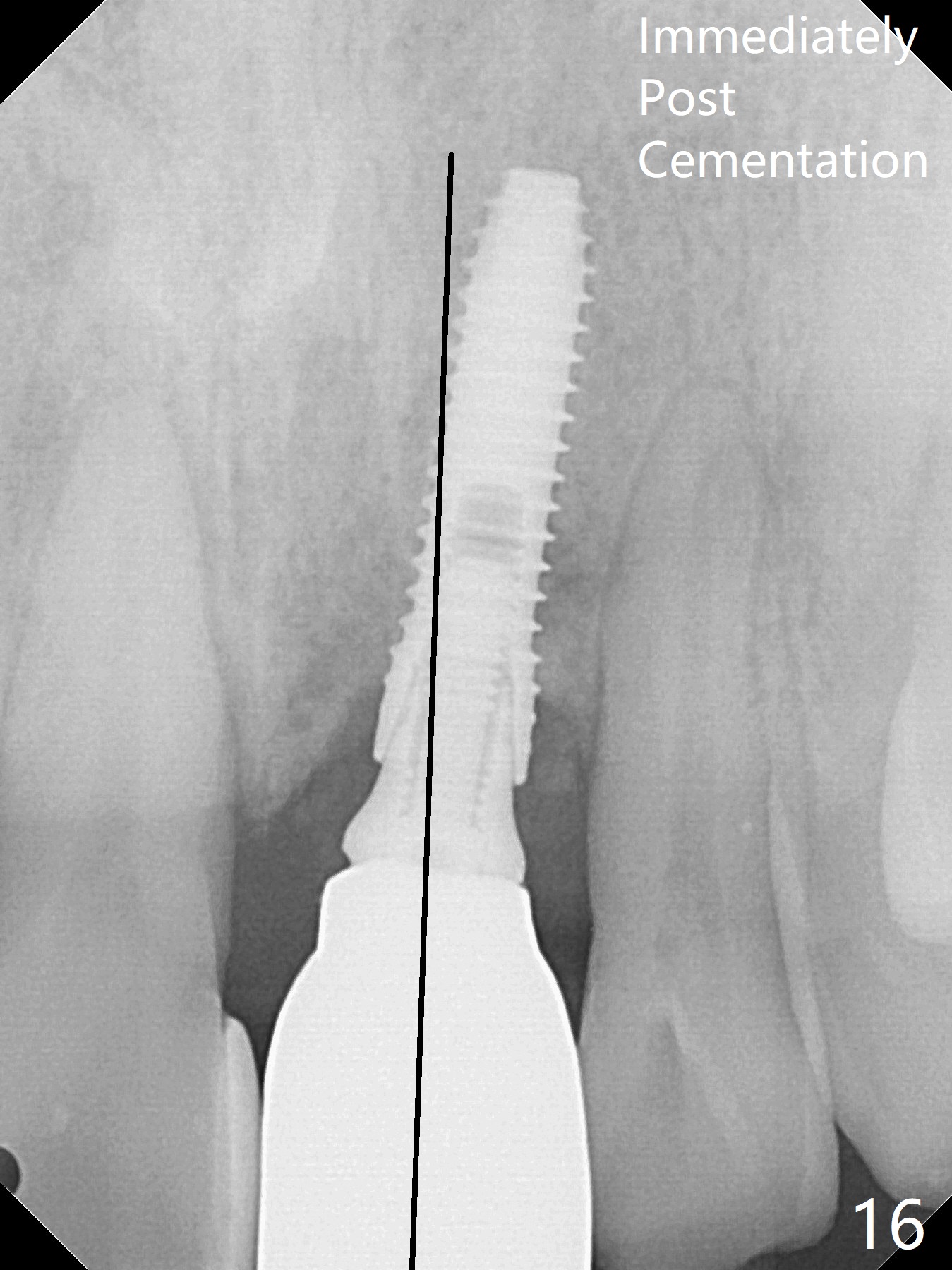
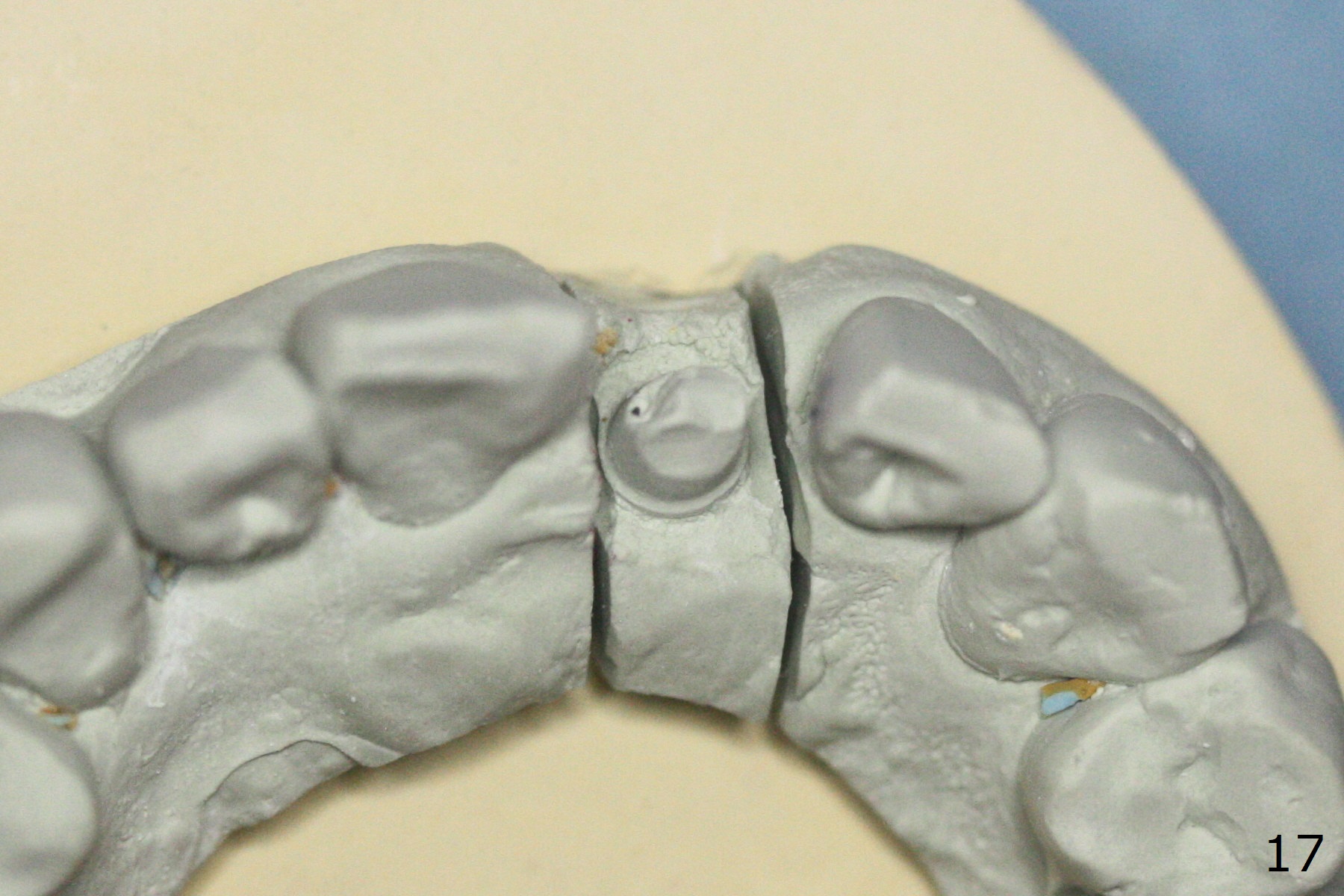
Nearly 7 months postop, the immediate provisional at UL1 is removed; with the mesial reduction of UL2 from 7 to 6 mm (Fig.1), an angled abutment is to be changed (4.5x15 degree, 2 mm cuff). A new provisional (Fig.2,3) co-incides with the facial midline. Brackets will be placed between UR4 to UL3 except UL2 (symptomatic once with chronic periodontitis) with initial proximal reduction between UR1-4 in preparation to correct cross bite of UR2. Twelve days later, the patient returns for UR5-UL3 bracketing after UR1-4 initial proximal reduction with 14 niti wire (Fig.4-6). UR1 moves mesial 20 days post open coil spring (Fig.7 arrow), while UL1 debracketes after permanent re-cementation of the temporary crown last visit (*, no re-bracketing, since it appears not essential). Before placement of 20 ss wire, diastemata are created by proximal reduction (Fig.8 *). In fact UR1 moves mesial, while UR3 does not move distal with the open coil. With placement of UR6 (implant) molar band, UR3 is distalized effectively. With sling shot, UR2 is almost labialized in one appointment (Fig.9). After consolidation of the diastemata between UR1-6 with power chains following UR2 cross bite correction (Fig.10), the restoration space for UL1 seems to be too large (Fig.11). Next visit, check the midlines, take 1-2 PAs for #7-9 and determine whether a straight abutment should be changed back and whether composite should be placed UR1 mesial to reduce the space. One week later, composite is added to the mesial surface of the tooth #8 to increase its width, while the provisional at #9 is relined to improve the interdental papilla (Fig.12). Minimal bone loss at UR2 is observed 8 months post banding (Fig.13), while the socket at UL1 seems to have healed except the most coronal 1 year 3 months postop (Fig.14 *). The margin of the abutment should be uneven, more coronal proximal than buccopalatal (Fig.15). The final crown has an open margin, partially due to less ideal trajectory (Fig.16 (black line: ideal trajectory, nearly 1 year 4 months postop)). Guided surgery could solve the problem. Sticky bone may restore the buccal plate defect. Die shows that the implant is palatally placed (Fig.17). CT will be taken to determine whether the implant perforates the palatal plate.
Return to
Upper Incisor Immediate Implant,
Armaments,
Ortho Cases
Xin Wei, DDS, PhD, MS 1st edition 08/31/2018, last revision 04/20/2020