
|
|
|
|
|
|
|
|
|
|
|
|
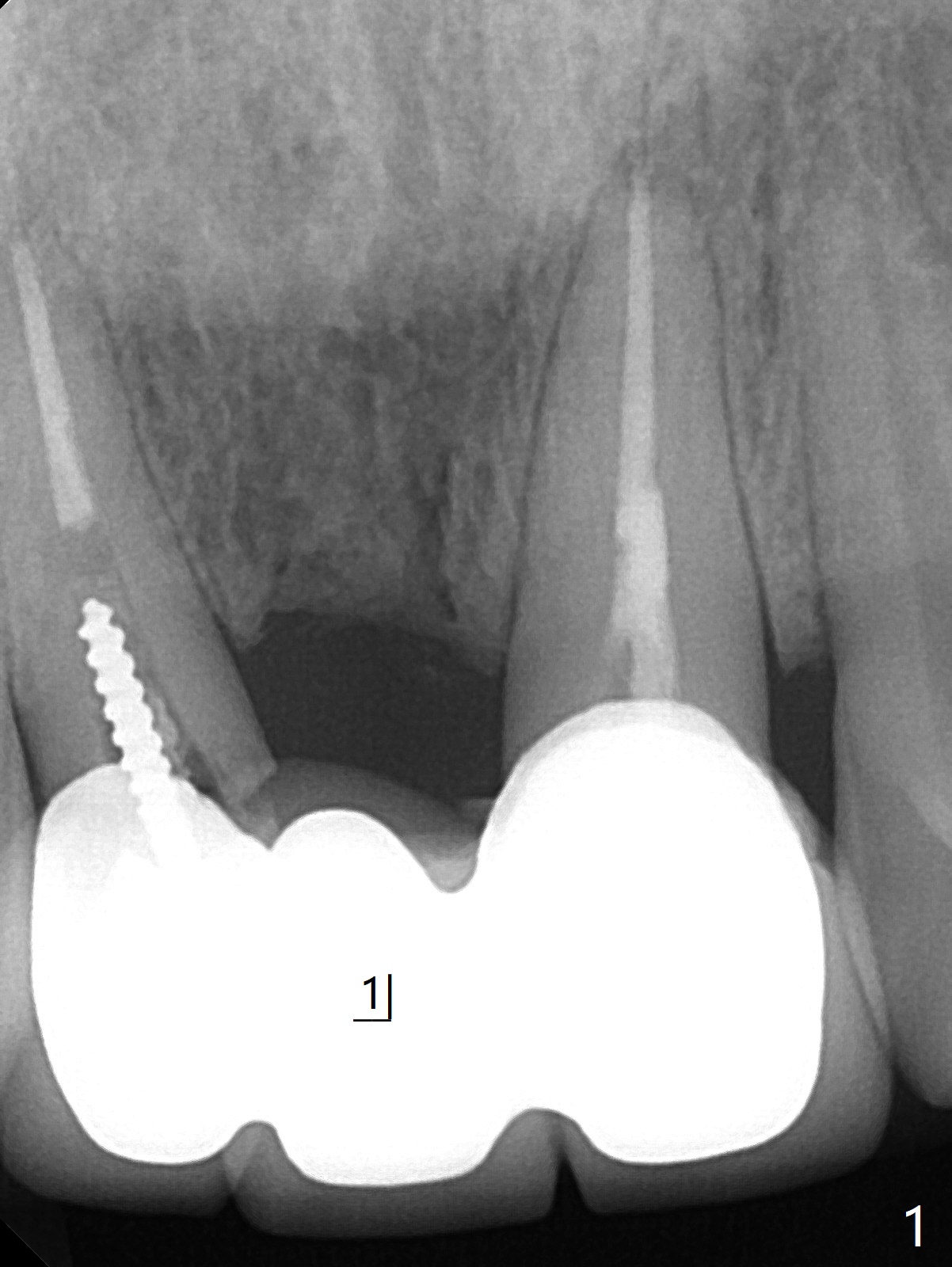
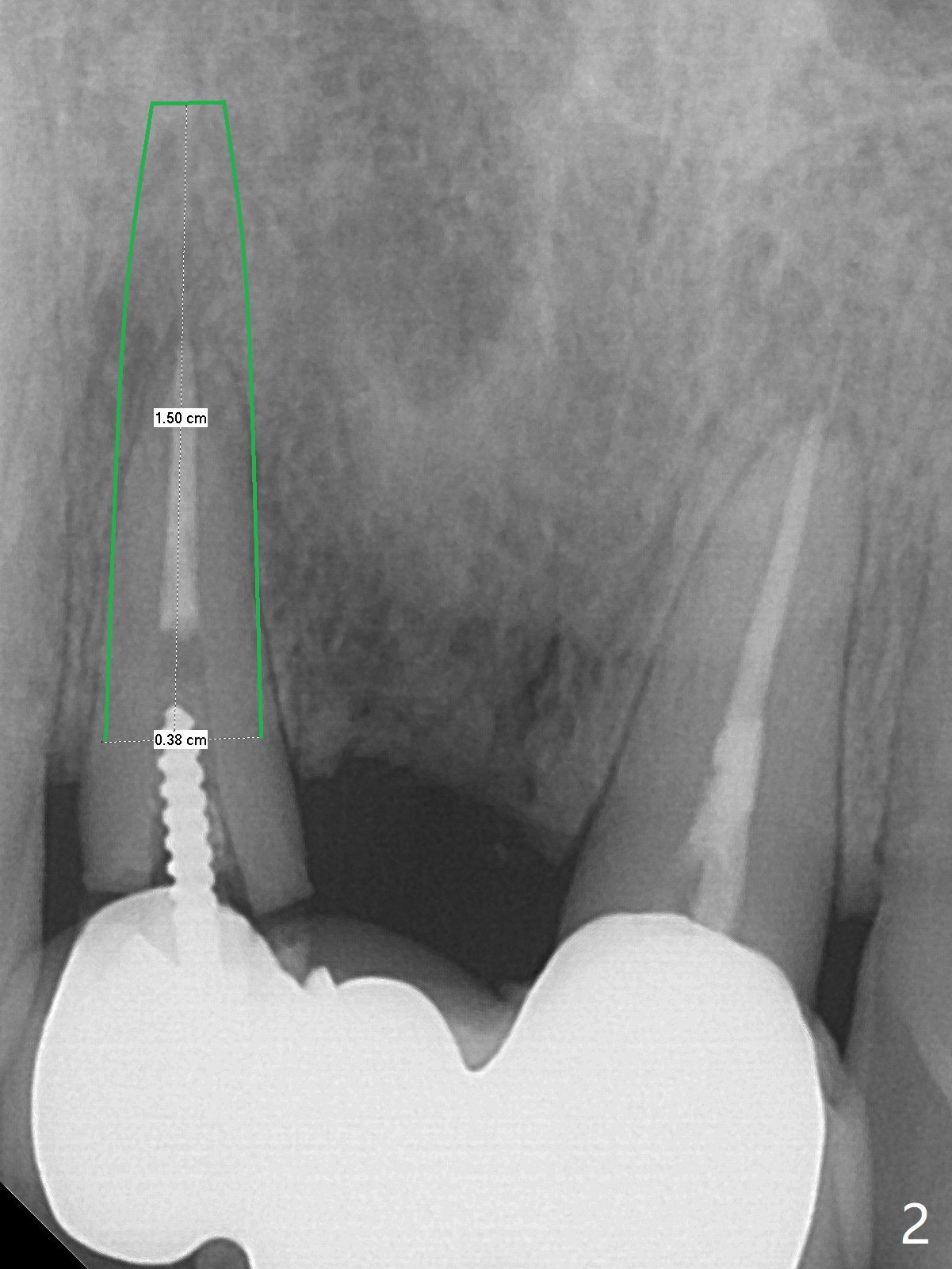
FPD Abutment Fracture
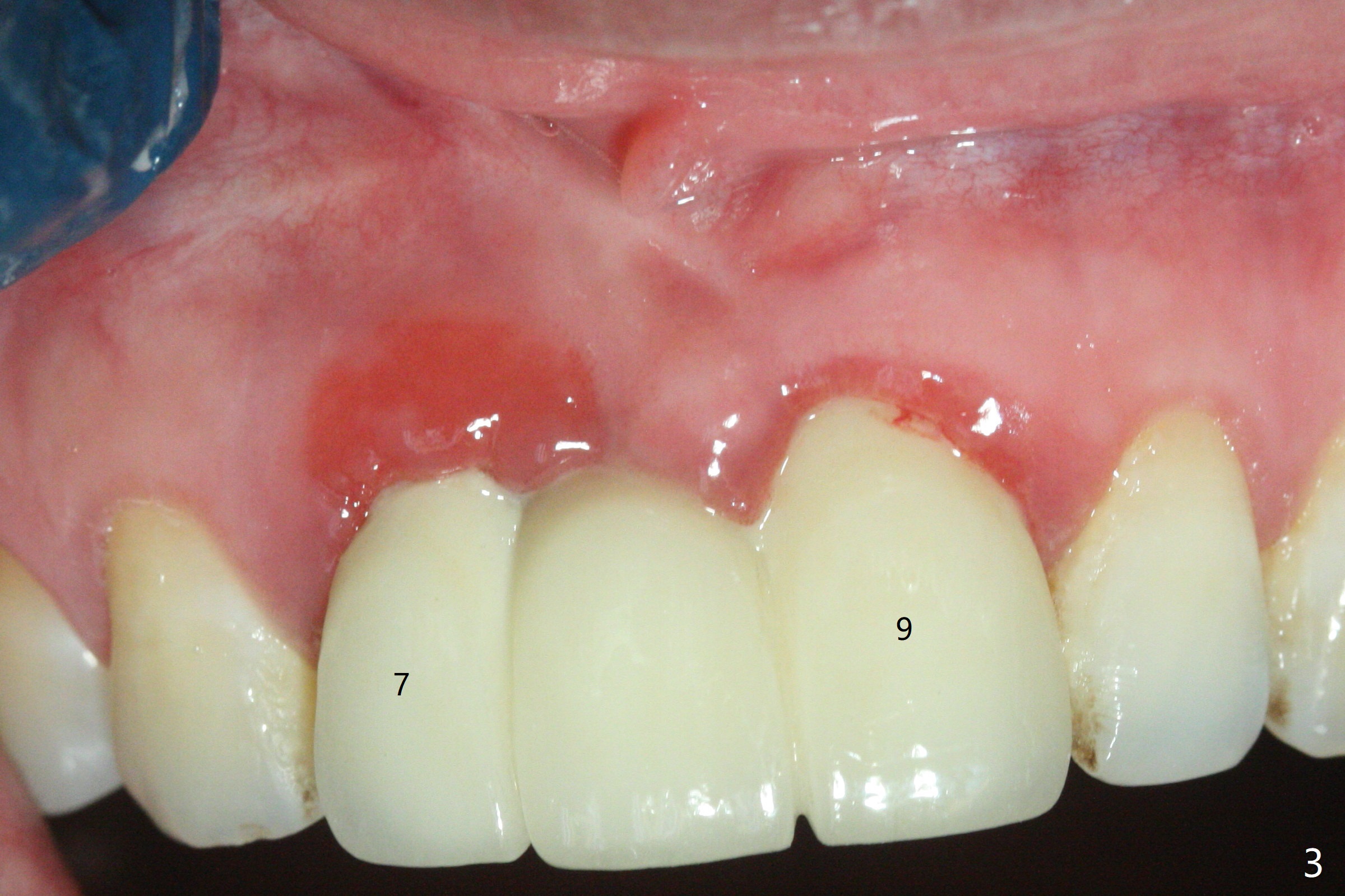
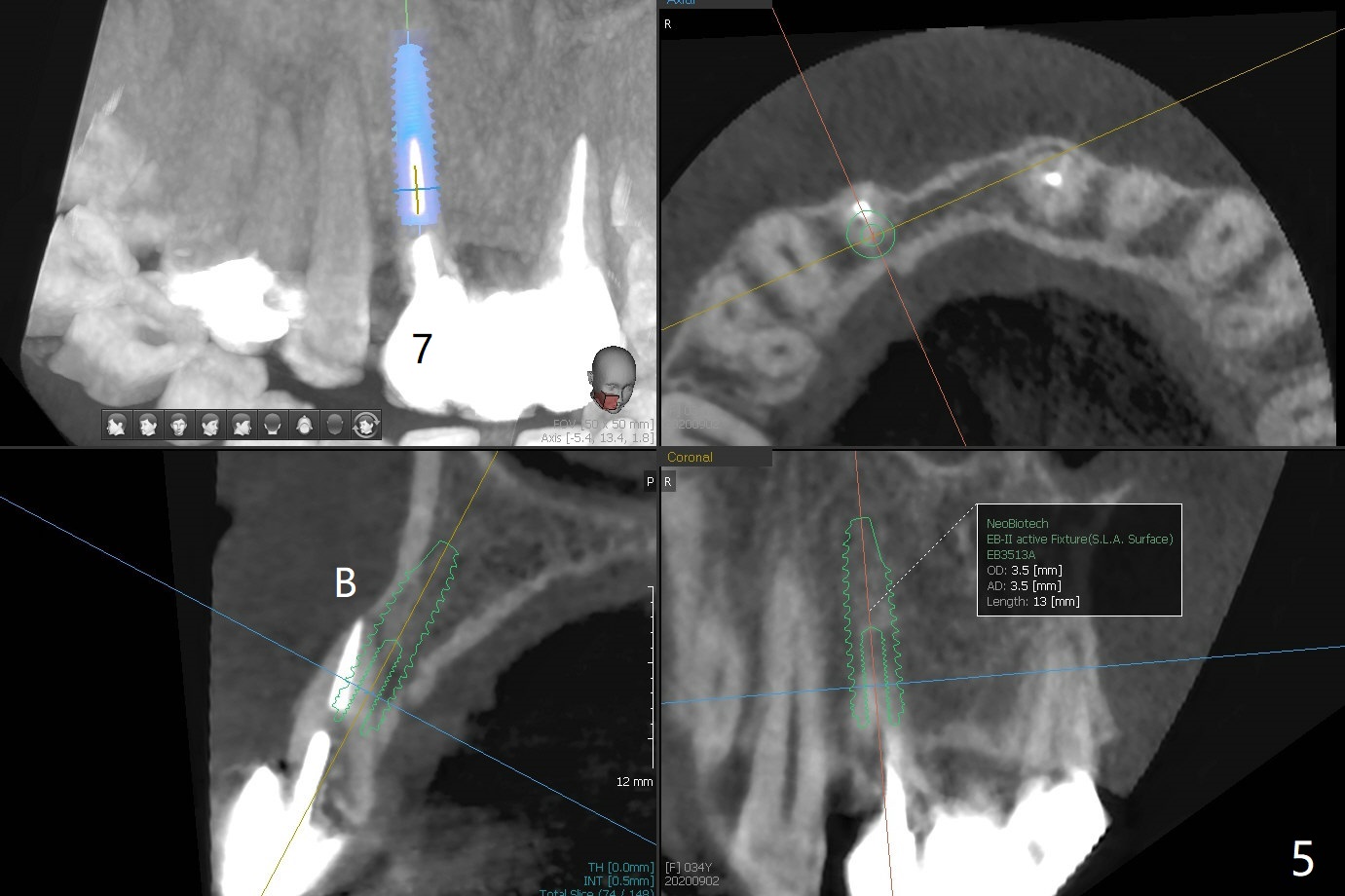
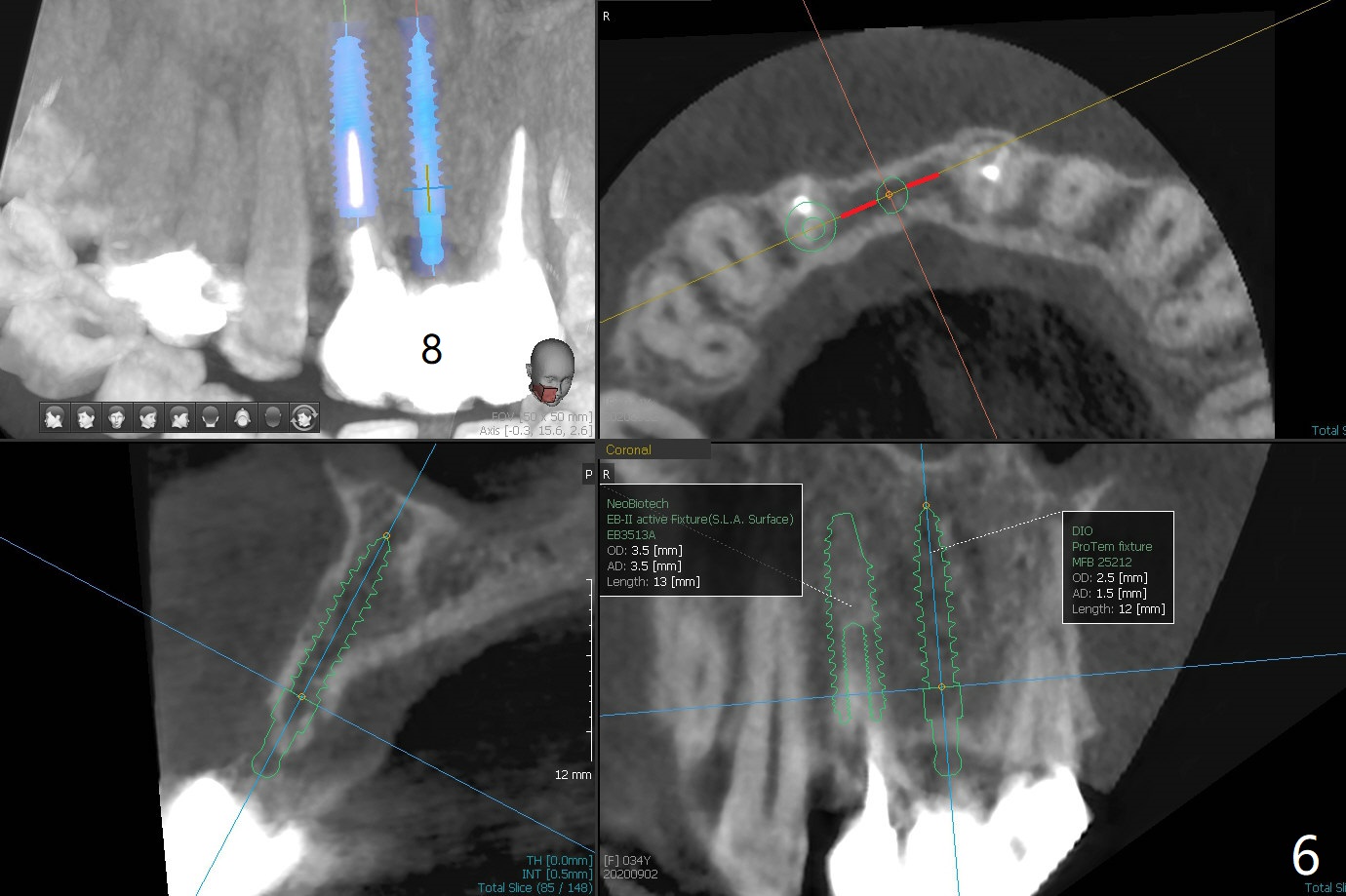
A 34-year-old woman requests fixing the failed anterior FPD (Fig.1). The edentulous alveolus looks thin; 1-piece implant may be indicated at most. A regular narrow 2-piece implant will be placed at the lateral incisor (Fig.2). CT is necessary for treatment planning. Impression has been taken for stent fabrication. 34岁女,一年半前来诊所(图一,二(侧切牙种植,做悬臂桥,暂时保留左上1牙冠)),希望修复右上门牙桥。现在终于要求立即做,基牙处牙龈红肿 (图三(今天做深洗)),牙桥颊侧移位(图四),侧切牙(7号牙)牙槽嵴也不是很宽,植入3.5毫米植体(两段式, IBS)还勉强(图五)。为了简化,避免悬臂桥,我还想在中切牙(8号牙)无牙处植入一段式2.5毫米植体(图六),适当做些牙槽嵴劈开(图六右上图:红线; from IBS cassette)。这周末徒手植入,她离开时应该有固定临时修复物。
Sequence of treatment: Section FPD between 8 and 9, photo of the narrow ridge of #8, incision, suture fixation of the flaps, ridge trimming with surgical handpiece/round diamond bur, confirmed by Tatum implant positioners (3 mm), 1.2 mm drill (8 mm deep), broken drill in place for PA later, ext #7, photos of curettes and granulation tissue removal instruments, 1.6 mm drill in the middle of the palatal slope, 1st intraop PA, #8 ridge split with IBS blade osteotome or thin surgical bur, subcrestal implant placement, fabricate temp especially for #8 before bone graft and suture to make sure subgingival margin and temp creating space for bone graft to make sure buccal and palatal bone thickness.
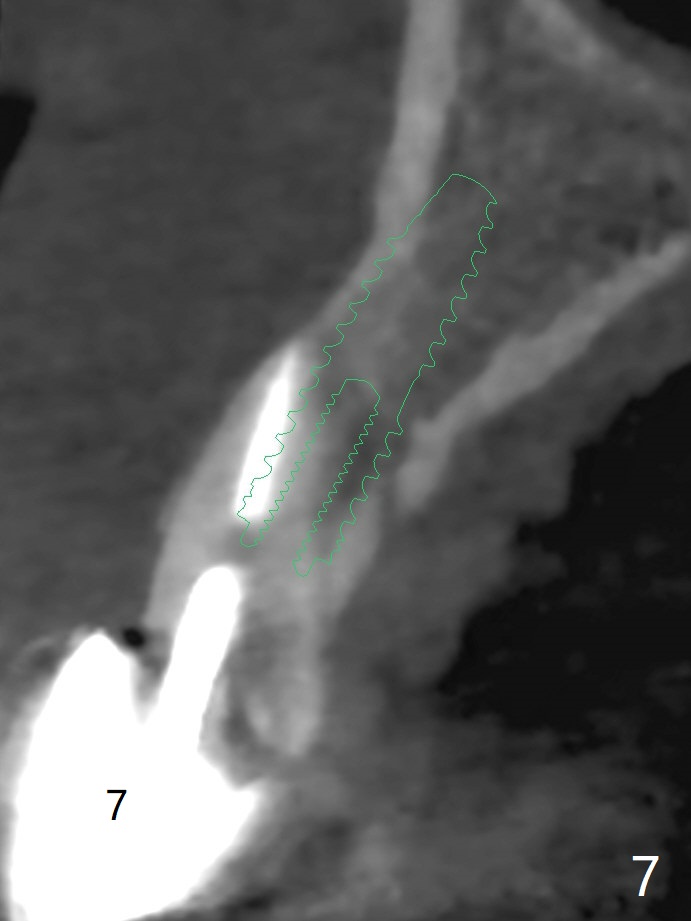
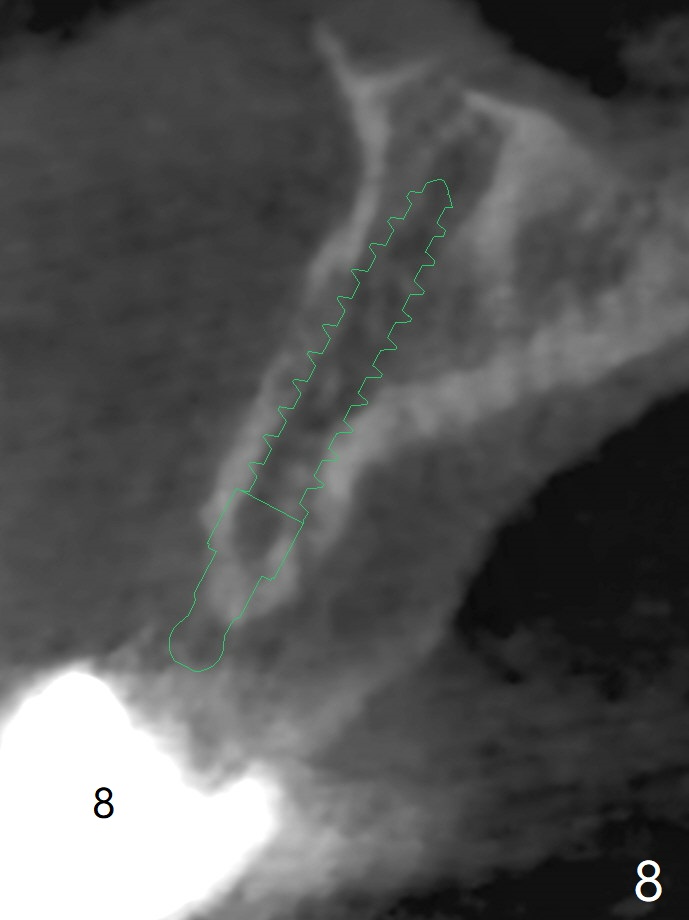
一段式植体似乎不美观,其实它适用于近中远中空间狭窄地方,如这个病例,而两段式植体显得太粗,没有空间形成牙龈乳头,况且容易以后导致植牙周围炎。即刻临时牙冠手术第一天就起到美观作用,术后三四个月中反复调整,为永久性牙冠奠定基础。以下手术步骤就是为了这个目的。在中切牙之间切断牙桥,为右上1狭窄牙槽嵴拍摄照片(颊侧,咬合面观),切口,铬羊肠缝线牵拉,外科车针去除尖端牙槽嵴直到后者宽度达到~ 3毫米,使用1.2毫米一段式钻头,8 毫米,插入一个已经折断同样大小车针作为定位;拔除侧切牙,拍摄各式各样刮匙和肉芽组织去除器械,用1.6毫米钻头在腭侧骨板钻洞,深度9毫米,拍摄术中第一张根尖片;在中切牙处使用片状骨凿稍做骨扩张,必要时旋转式扩大器,之后完成牙槽嵴下植体放置,侧切牙牙槽窝以及中切牙术野插入无絮棉布,做必要基台制备,使用成品临时牙冠制作两个分开牙冠,确保牙龈下边缘,取出棉布,植骨,放置PRF膜,插入临时牙冠,尤其是中切牙牙冠和骨粉将改善颊侧,腭侧(与图四箭头对比)饱满度,最后缝合,调整咬合。7,8号牙骨质密度分别为700和 500单位(图七,八)。
Return to No Deviation No Antibiotic Xin Wei, DDS, PhD, MS 1st edition 08/27/2020, last revision 09/06/2020