|
|
|
|
|
|
|
|
|
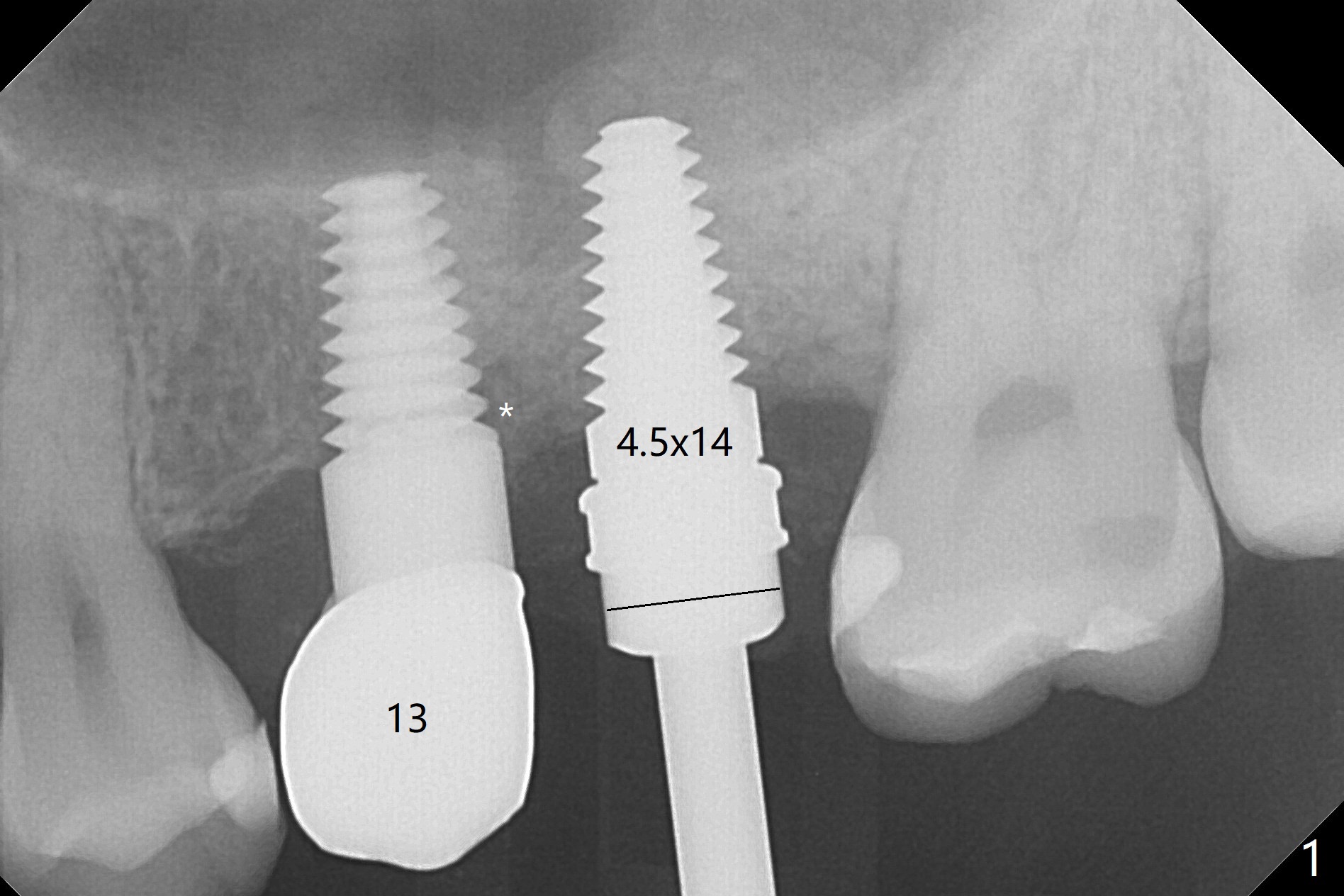
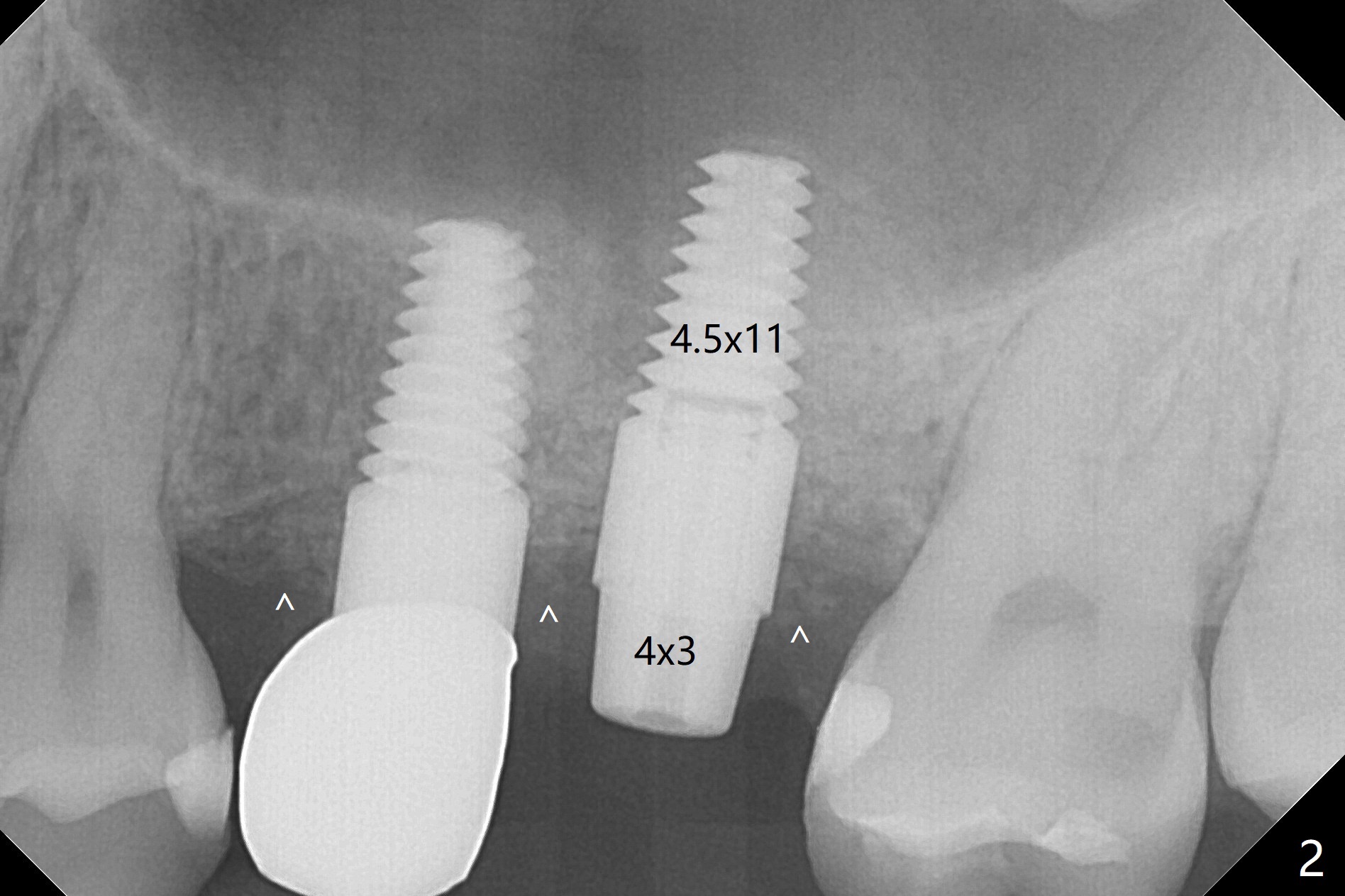
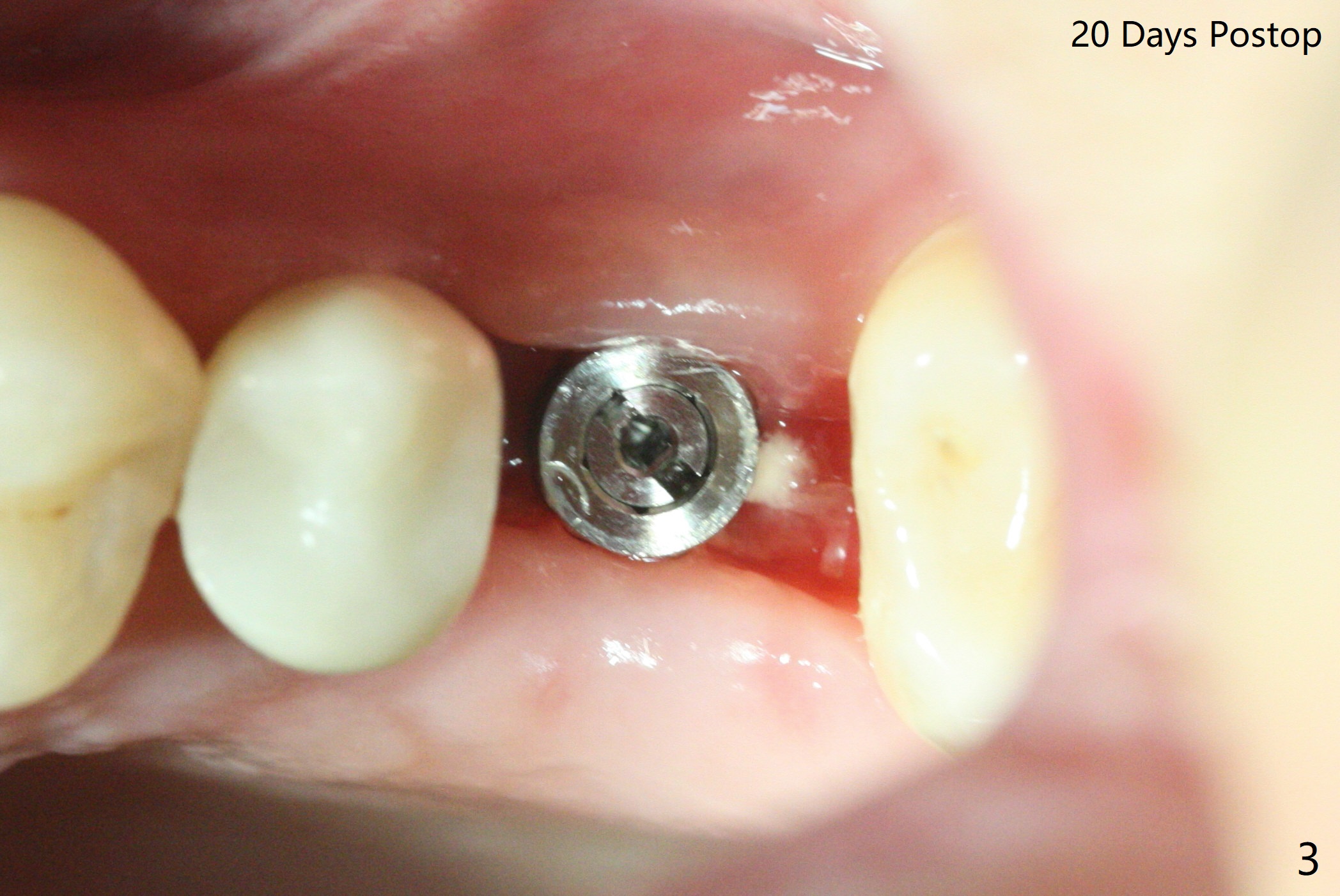
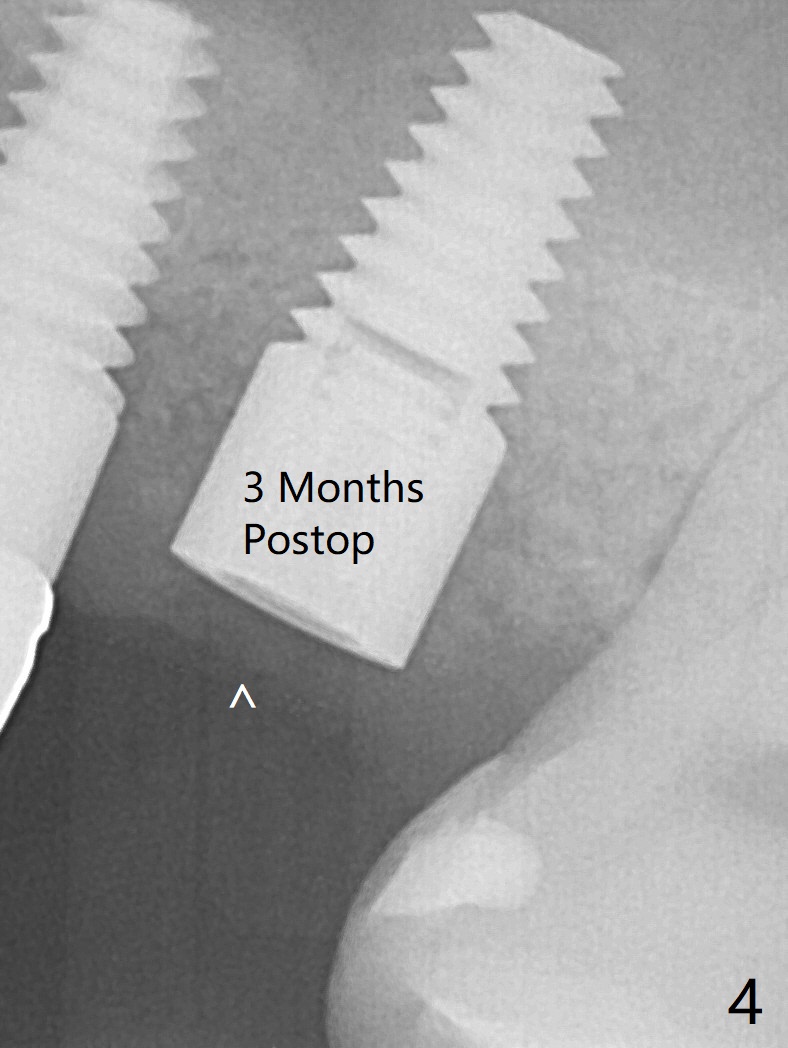
No CT No Implant (I)
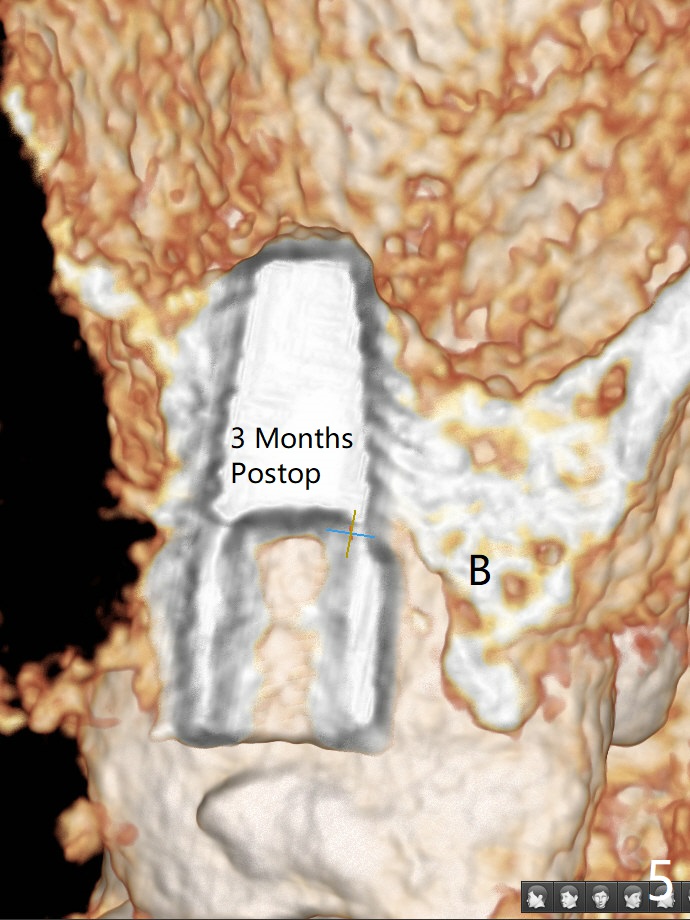
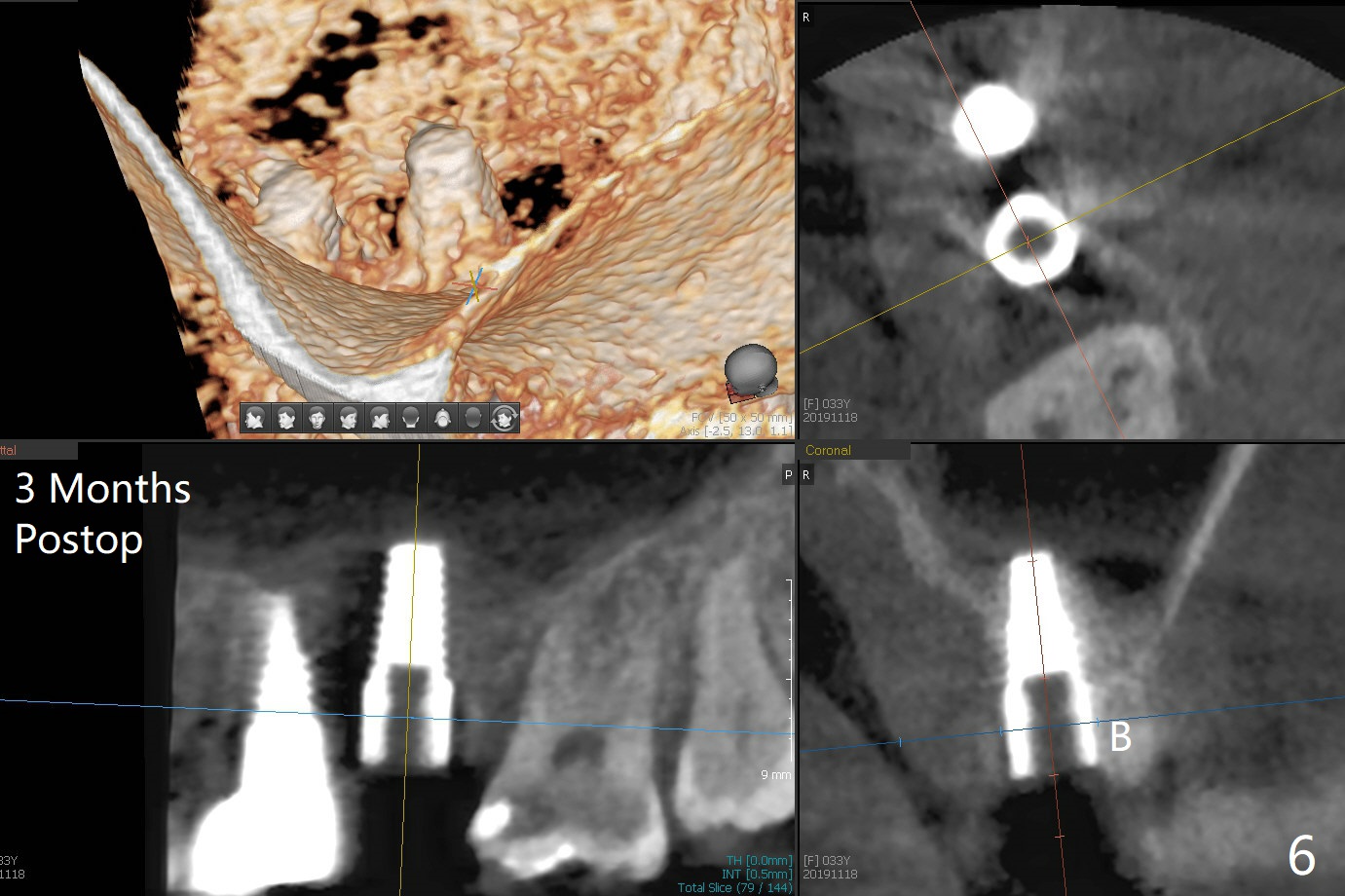
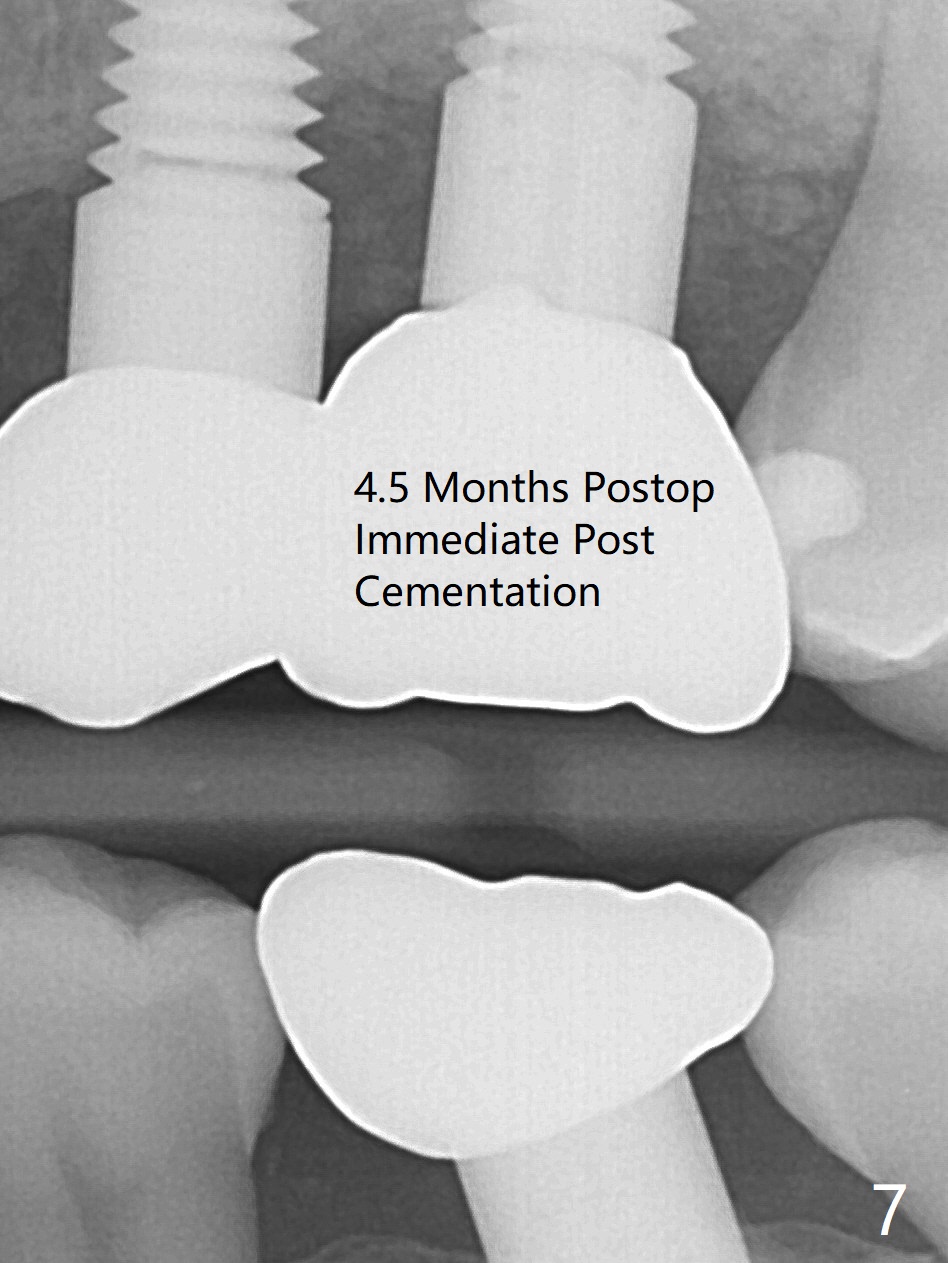
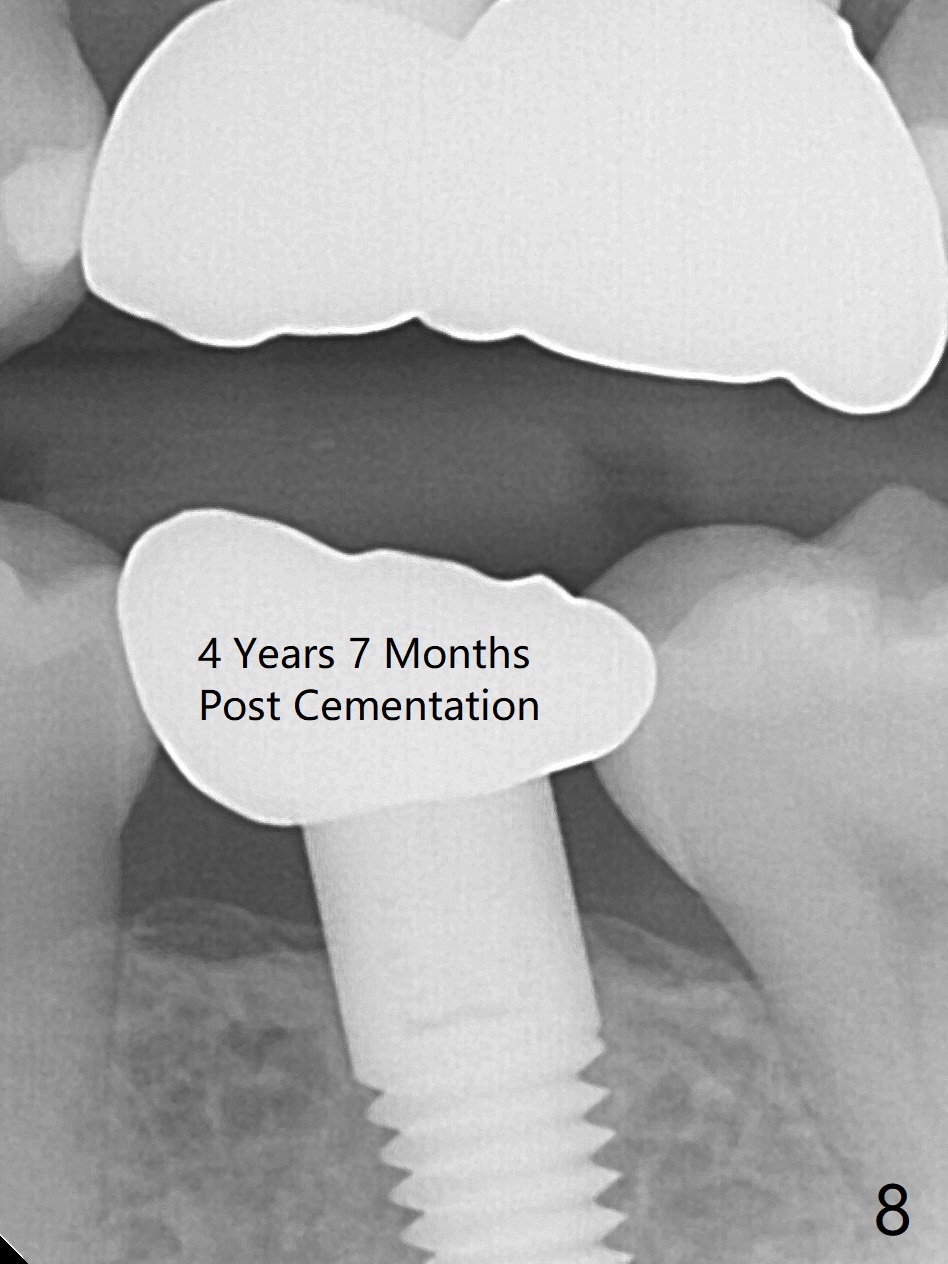
The ridge at #14 seems wide 6 months post implant removal and bone graft (before and after incision). In fact the palatal bone is low, which was the basis for periimplantitis. The new osteotomy is not initiated buccal enough. Immediate redo or guided surgery can avoid this complication. When a 4.5x14 mm tap is placed (Fig.1), the palatal threads are exposed. The buccal bone of the osteotomy has to be removed before placement of a 4.5x11 mm with 1 thread exposure palatal (Fig.2). Periimplantitis at #13 is found intraop (Fig.1 *). After removal of granulation tissue and use of Titanium brush, allograft is placed at #13 and 14 (Fig.2 ^) and is covered by PRF. Bone expansion is not conducted because of high bone density. If there is difficulty in restoration due to deep implant placement, it has to be backed up using torque wrench. The wound appears to heal by secondary intention 20 days postop (Fig.3). The implant is subgingival nearly 3 months postop (Fig.4 ^: gingival margin). It appears that the implant could be backed up (Fig.5,6). A 5 mm healing cuff is placed with Cetacaine and antibiotic ointment. The implant remains subgingival with the healing abutment 4 months postop. With Cetacaine and 2 gingival retraction cords, the implant margin is barely exposed. Large and deep gingivectomy is performed with Waterlase without too much pain. The gingival cuff is slightly erythematous and hemorrhagic on cementation (partially due to suboptimal oral hygiene, Fig.7). The margin is deep. Tatum implants are contraindicated when the gingiva is thick (Fig.8).
Return to Upper Molar Immediate Implant, Trajectory II
Xin Wei, DDS, PhD, MS 1st edition 08/27/2019, last revision 01/09/2020