












|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Prevent Screw Loosening
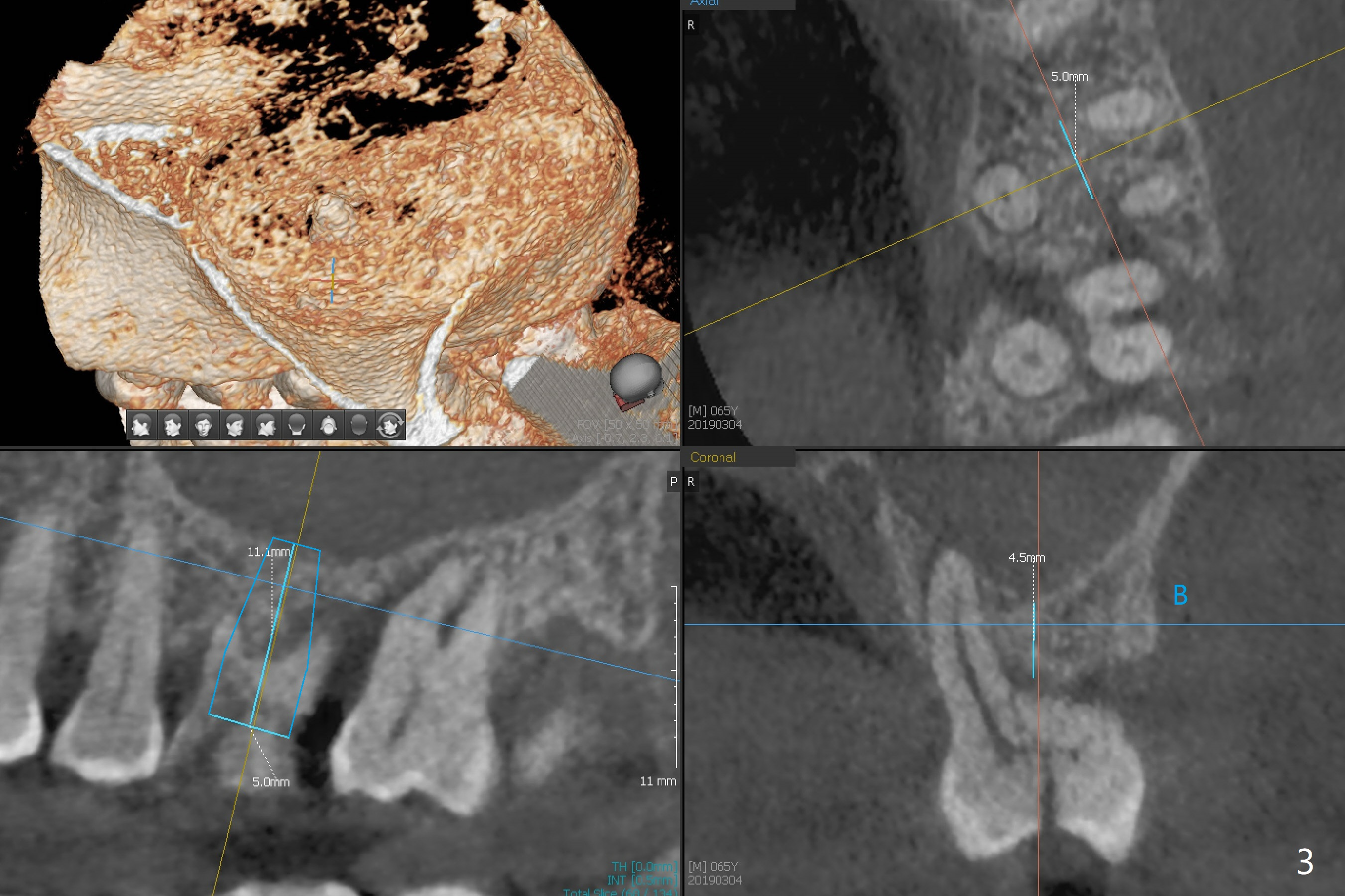
A 65-year-old man had crack tooth syndrome at #14 one month earlier (Fig.1). He shows up with crack and pain in an emergency manner (Fig.2 arrowheads). Preop CT confirms 4.5 mm bone height (Fig.3). Osteotomy will be initiated in the middle of the septum between 3 sockets (Fig.4). Depth of osteotomy is controlled with drill stoppers. After sequential osteotomy free hand, a 5x11 mm tap is used to break through the sinus floor (Fig.5) and sinus lift with Vanilla allograft. To prevent abutment screw loosening, a 5x11 mm tissue-level implant is placed; the distal thread is equicrestal (Fig.6 arrowhead). Following deeper placement of the implant (Fig.7 arrow) with a larger and longer abutment (as compared to that in Fig.6), the margin for an immediate provisional (Fig.9 white curved lines) is prepared in the coronal end of the implant (Fig.8 between arrowheads). With the tissue-level implant, the crown/implant ratio improves. Stress will be partially acting on the implant so that there is less likelihood of abutment screw loosening. The socket heals 1 month postop (Fig.10). The rough surface of the implant is exposed ~ 1 mm. With the margin modified and polished, the provisional returns to place with oral hygiene instruction. It is hoped that the gingiva will cover the exposed rough surface. The buccal rough surface remains exposed 5 months postop (Fig.11). The bone in sinus lift is mature 5 months postop (Fig.12,13). The first 1-2 implant threads are expected to be filled with mature bone in the near future (*). Since the abutment seems long enough for retention, temp bond is used for cementation (Fig.14). Water pik is being applied.
Return to
Upper
Molar Immediate Implant,
Prevent Molar Periimplantitis (Protocols,
Table),
Trajectory,
Clindamycin
Next Similar Case
3
Xin Wei, DDS, PhD, MS 1st edition
03/04/2019, last revision
02/20/2020