
,%20Vanilla.jpg)






|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
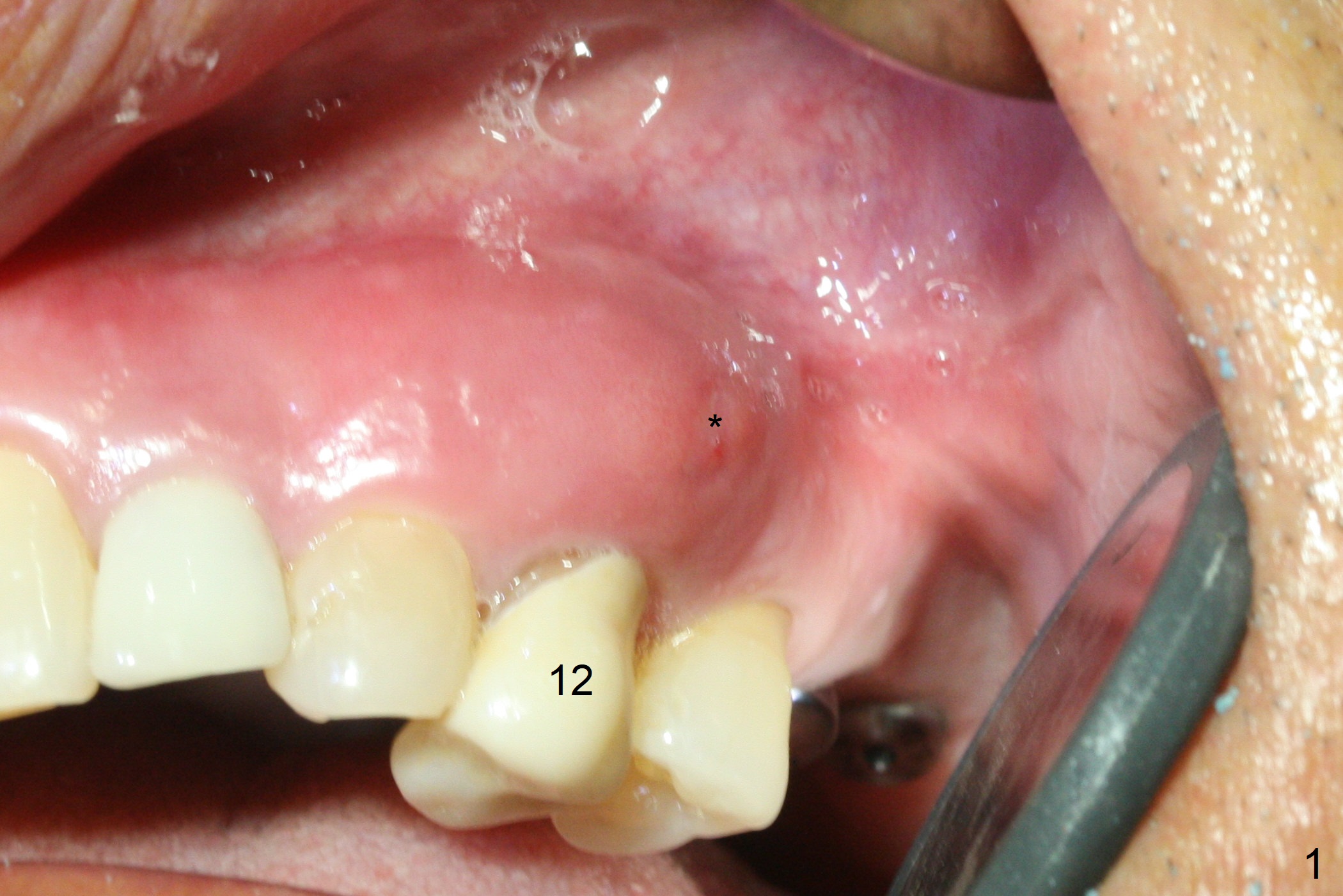
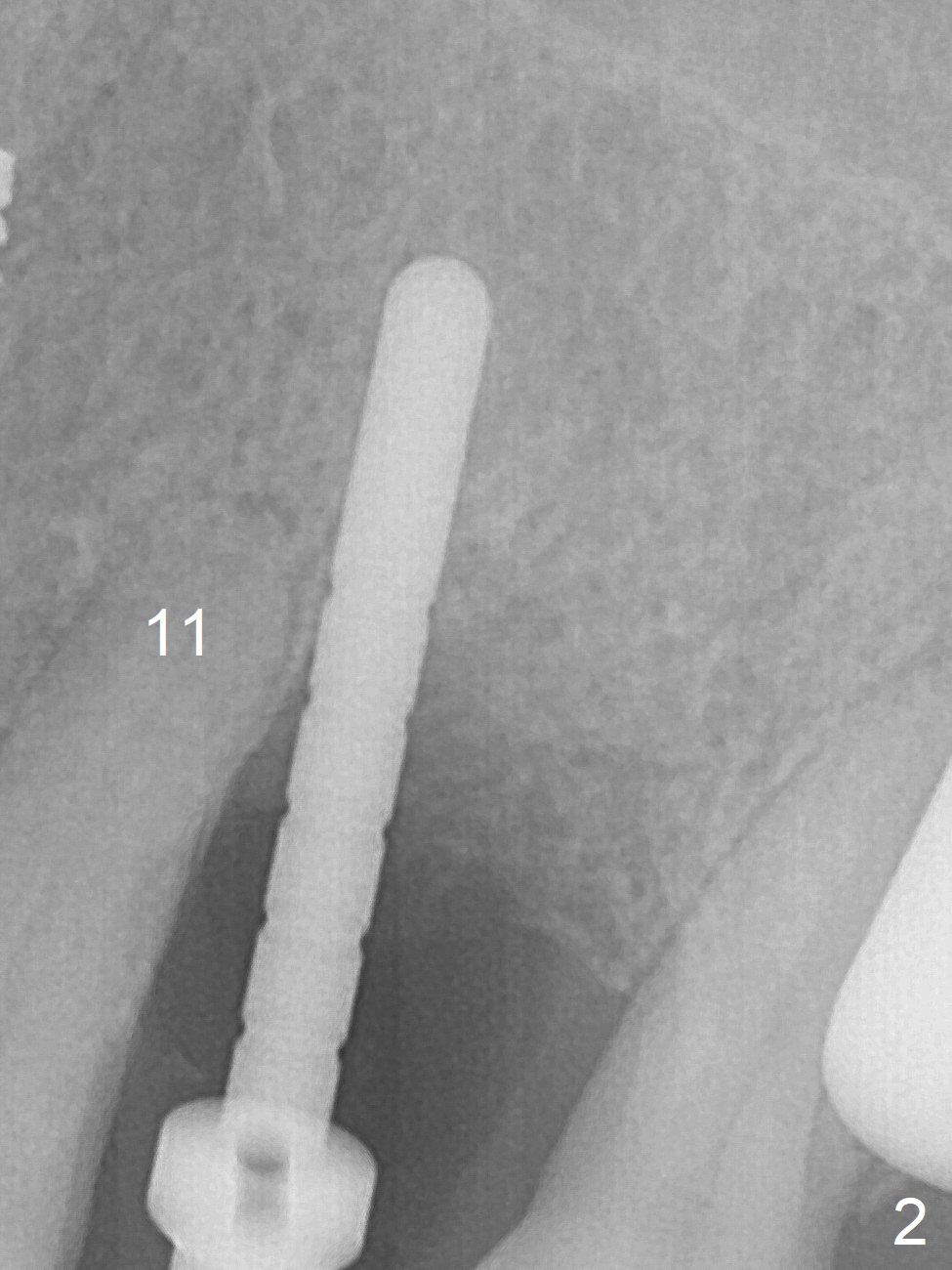
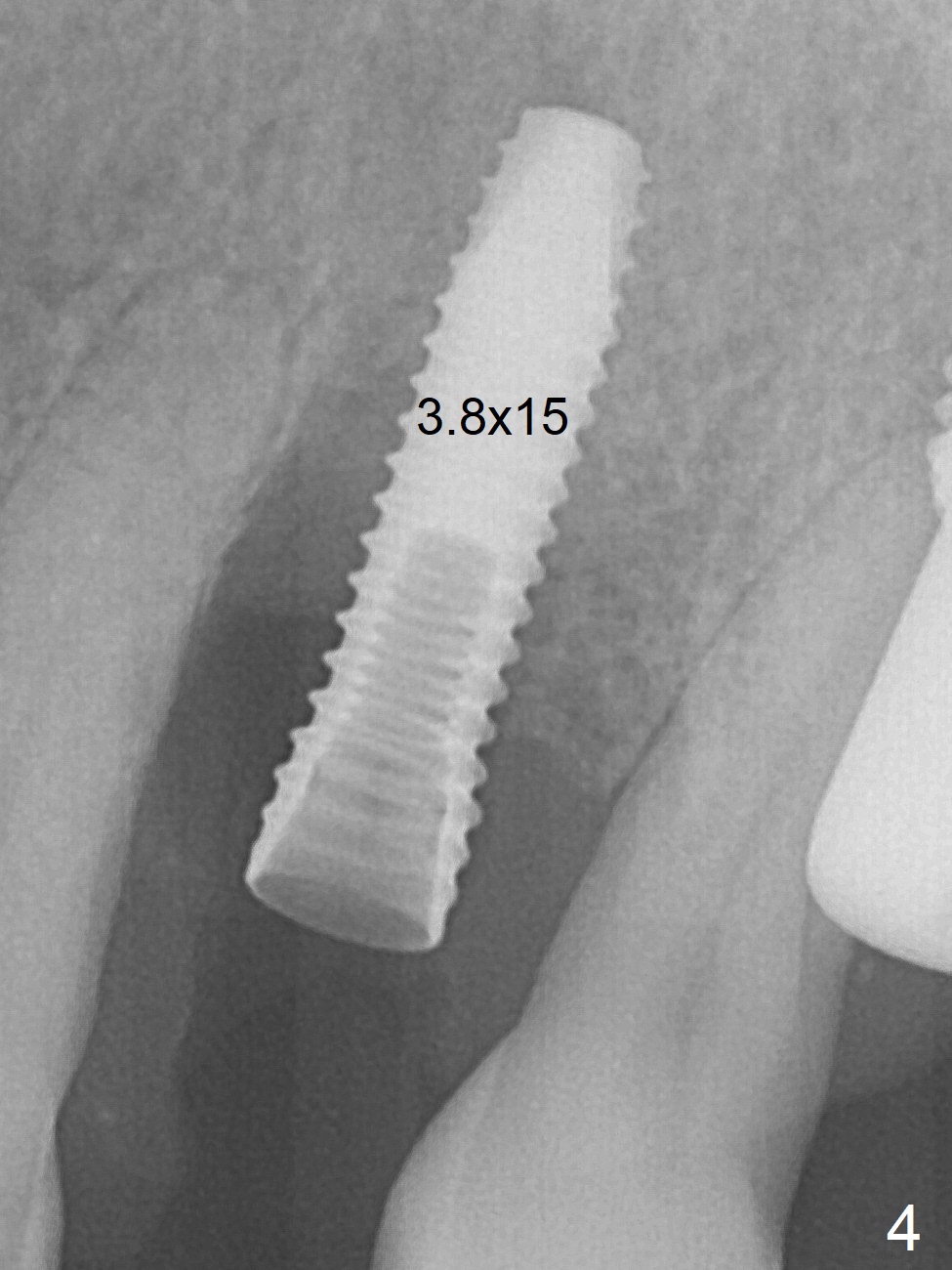
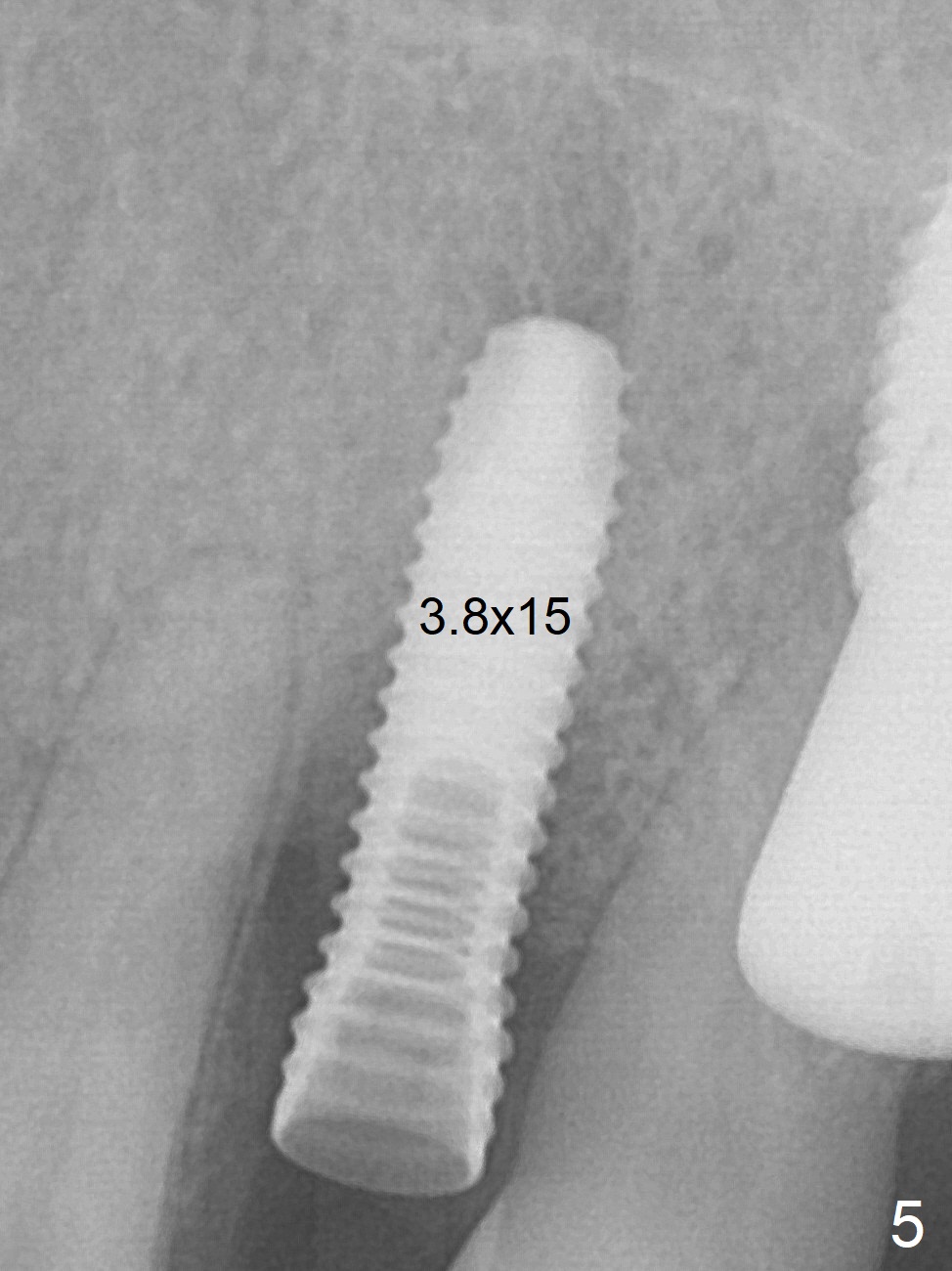
Deep Placement with Thread Exposure
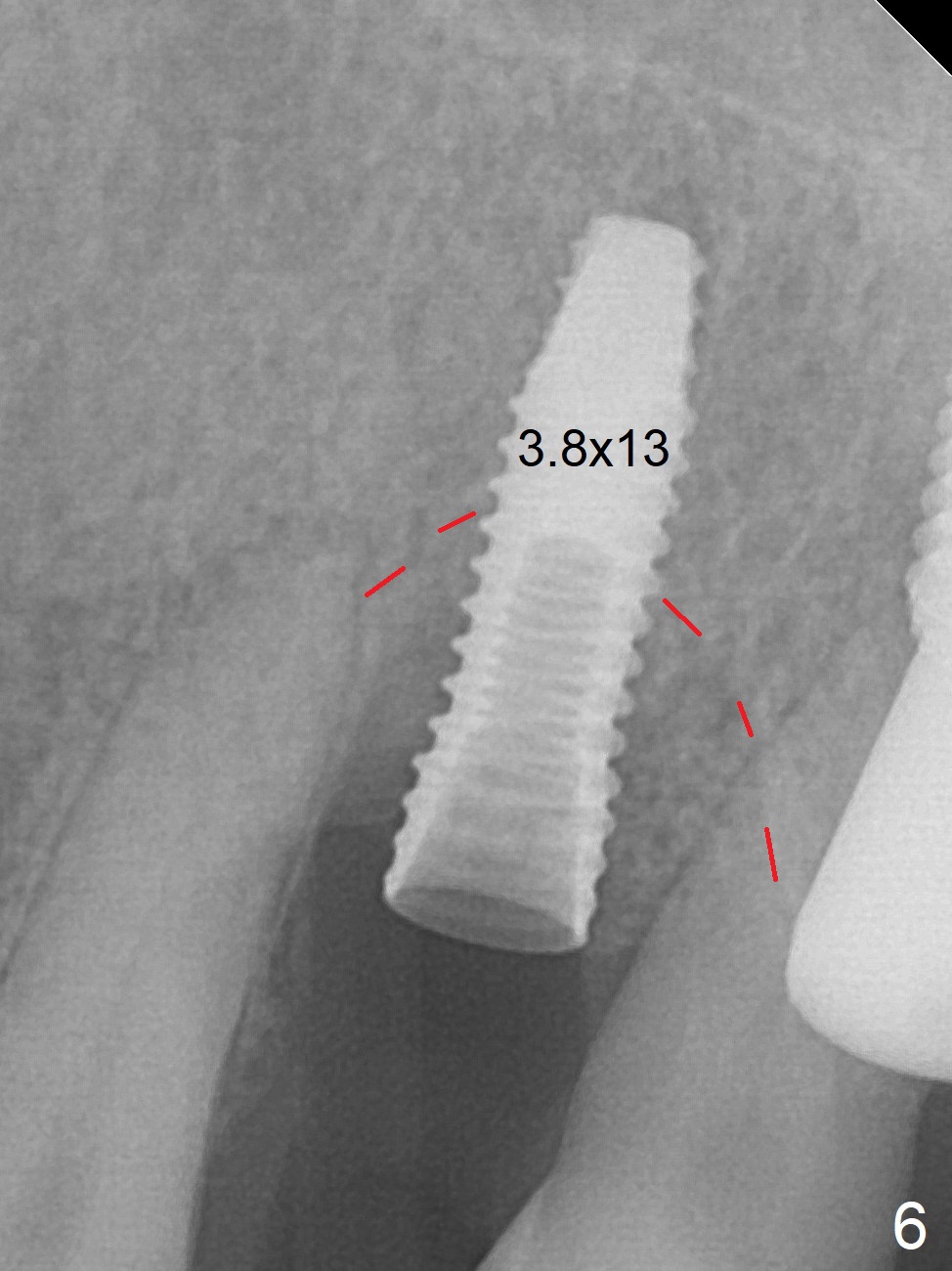
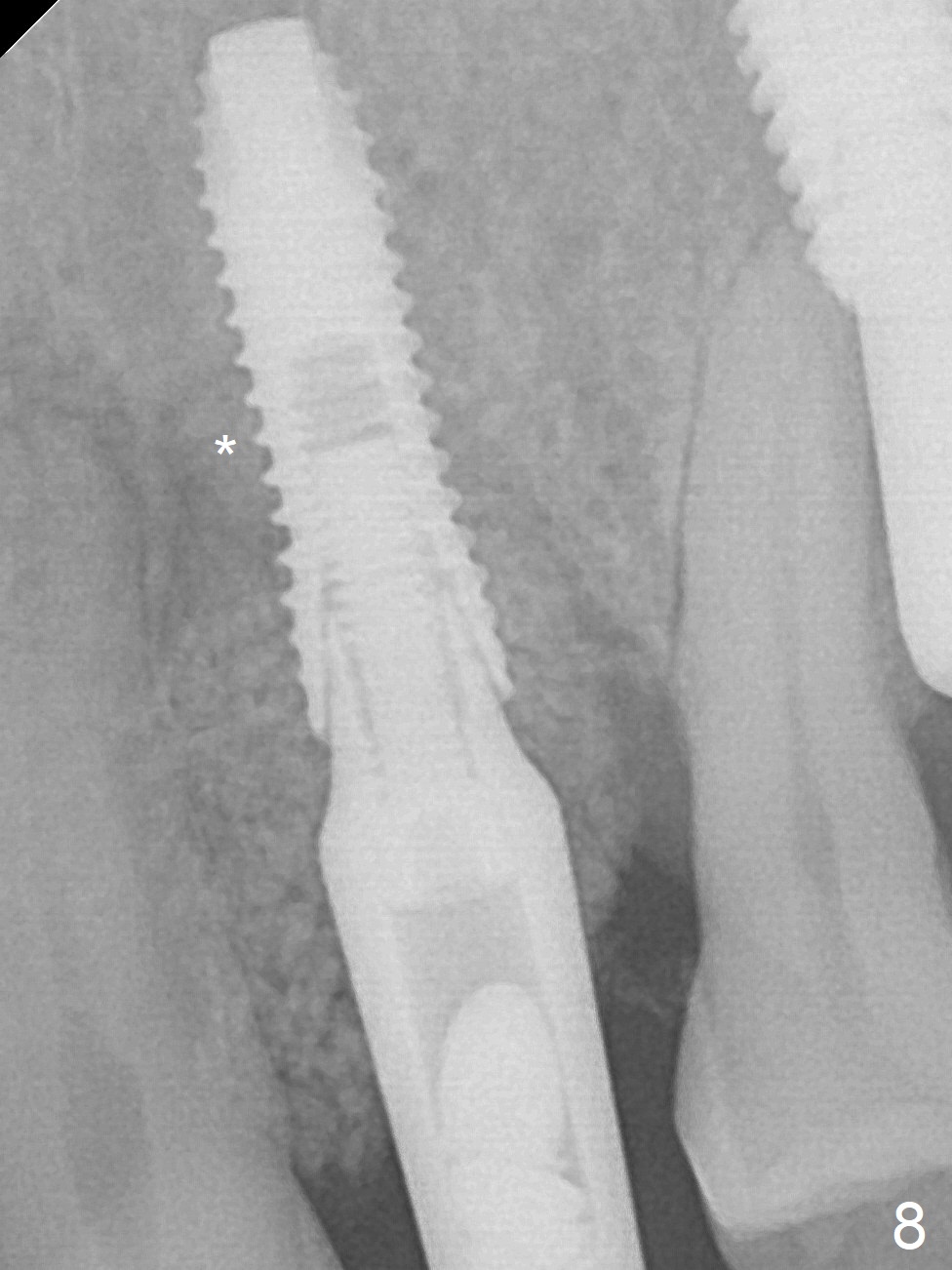
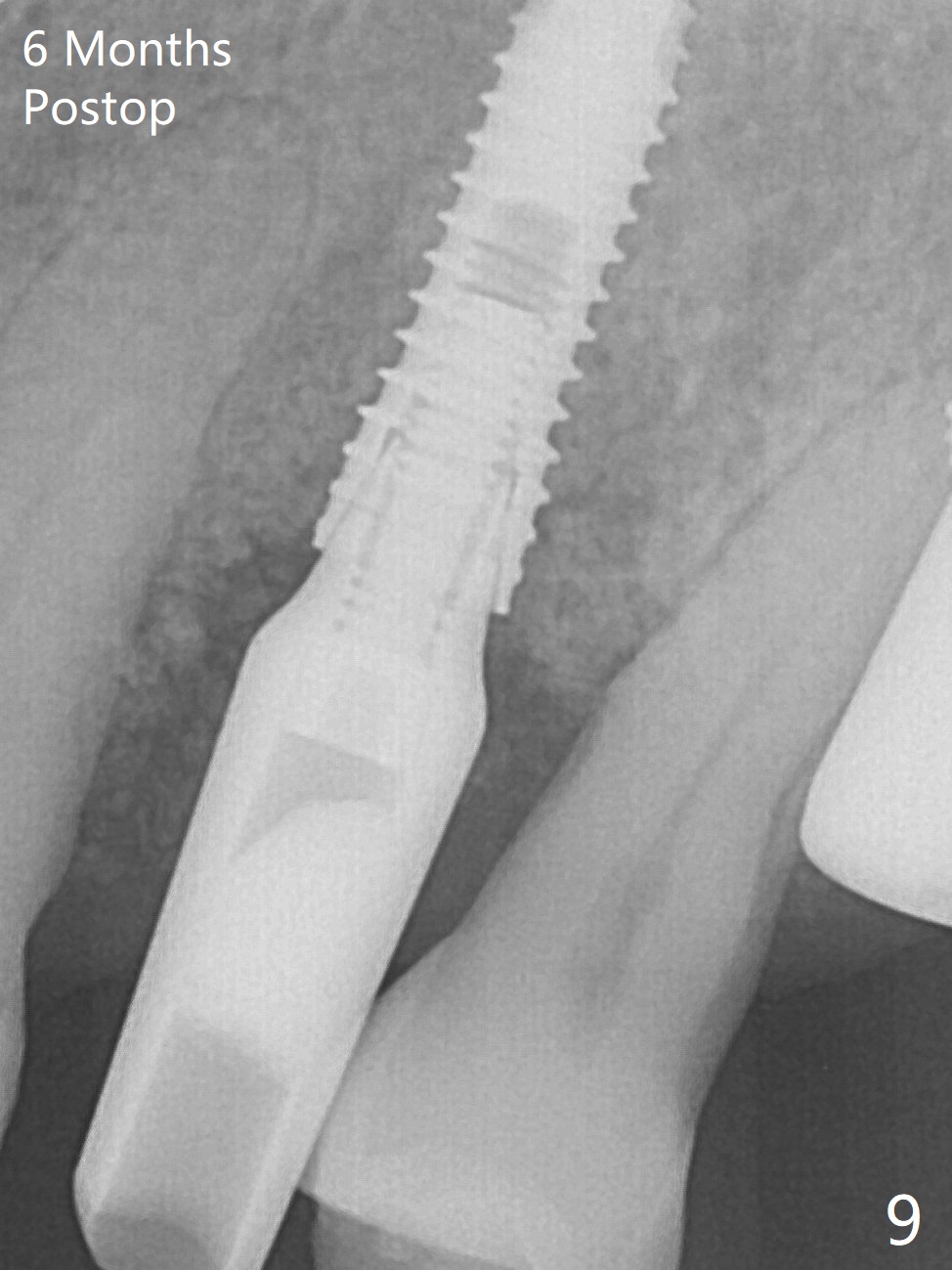
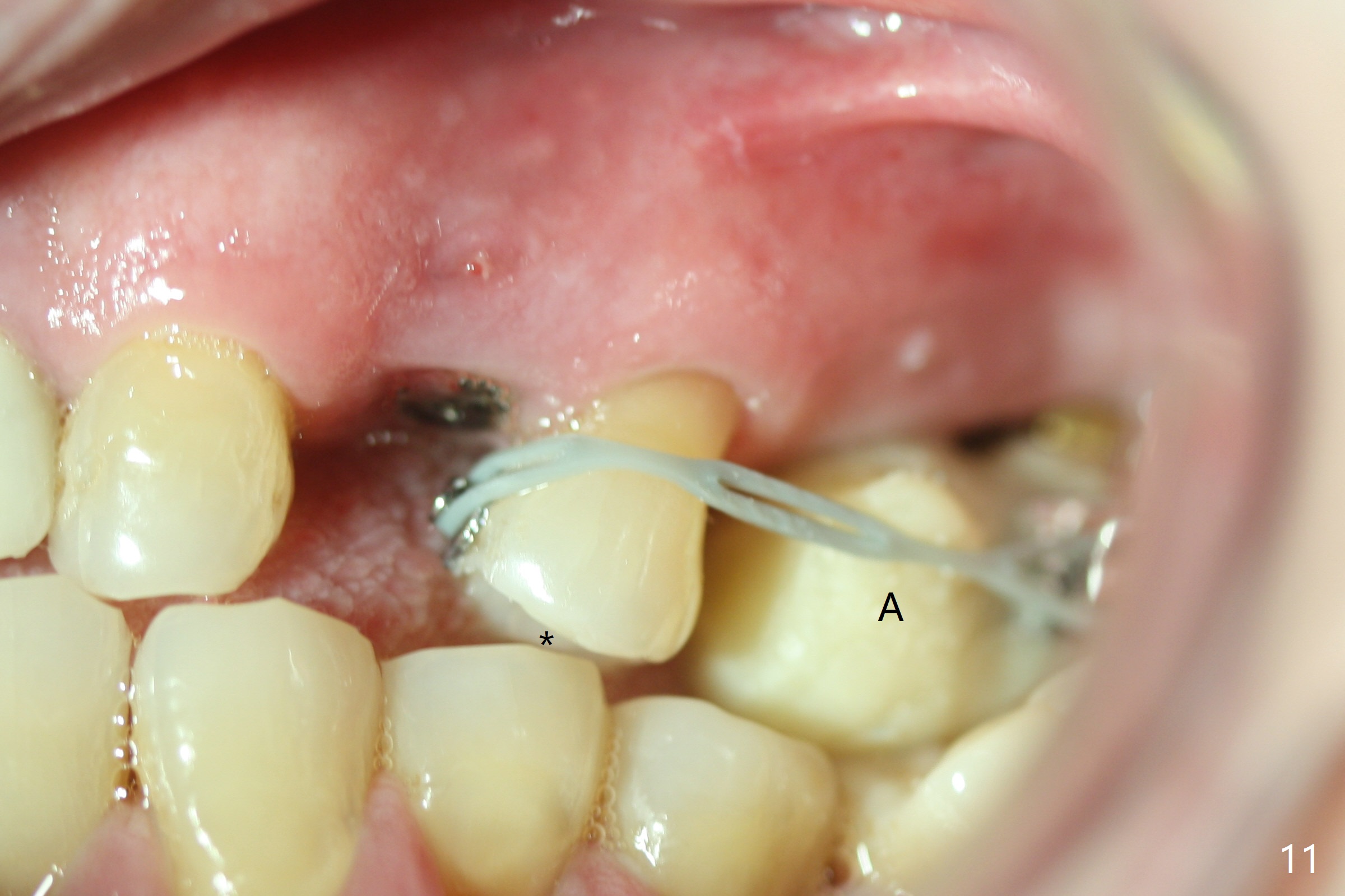
A few days prior to surgery, the tooth #12 developed abscess, self controlled by water pik (Fig.1 *). The buccal plate is defective. Initial osteotomy is close to the root of the tooth #11 (Fig.2). After adjustment of the trajectory and the depth of osteotomy (Fig.3), a 3.8x15 mm dummy implant is placed (Fig.4,5). In spite of a shorter implant (3.8x13 mm) placed deeper, approximately 7 mm implant threads are not covered buccally by the native bone (Fig.6 red dashed line). If the implant were placed deeper, the crown/implant ratio would become more unfavorable (abutment screw loosening, Fig.7). Since a mill abutment (4.5(2) mm) is inserted before Vanilla Graft, the deepest portion of the socket is unfilled (Fig.7 *). With meticulous use of a long explorer and additional allograft, the space is closed (Fig.8 *). The buccal plate collapses with apparently fistula formation 2 months postop. The patient removes the provisional for cleaning. It appears that the mill abutment is buccally placed and needs heavy reduction. The mill abutment is loose 2 months 10 days postop. When it is retightened, it tilts distal. Bone remains around the implant 6 months postop (Fig.9). Without a provisional at #12 for 5 months, the tooth #13 appears to have been shifted mesially (Fig.10 arrow). The mill abutment at #12 changes to a healing one. A lingual button is placed in the mesial surface of #13. Splinted provisional is fabricated with supraocclusion at #14 and 15 as an anchor (implants). The tooth #13 is being distalized with power chains. Limited ortho is finished nearly 2 months post banding (Fig.15,16).
Return to Upper Premolar Immediate Implant, Armaments #3 10 14/15 18 30 Xin Wei, DDS, PhD, MS 1st edition 06/15/2018, last revision 03/08/2019