


.jpg)
.jpg)
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|||||
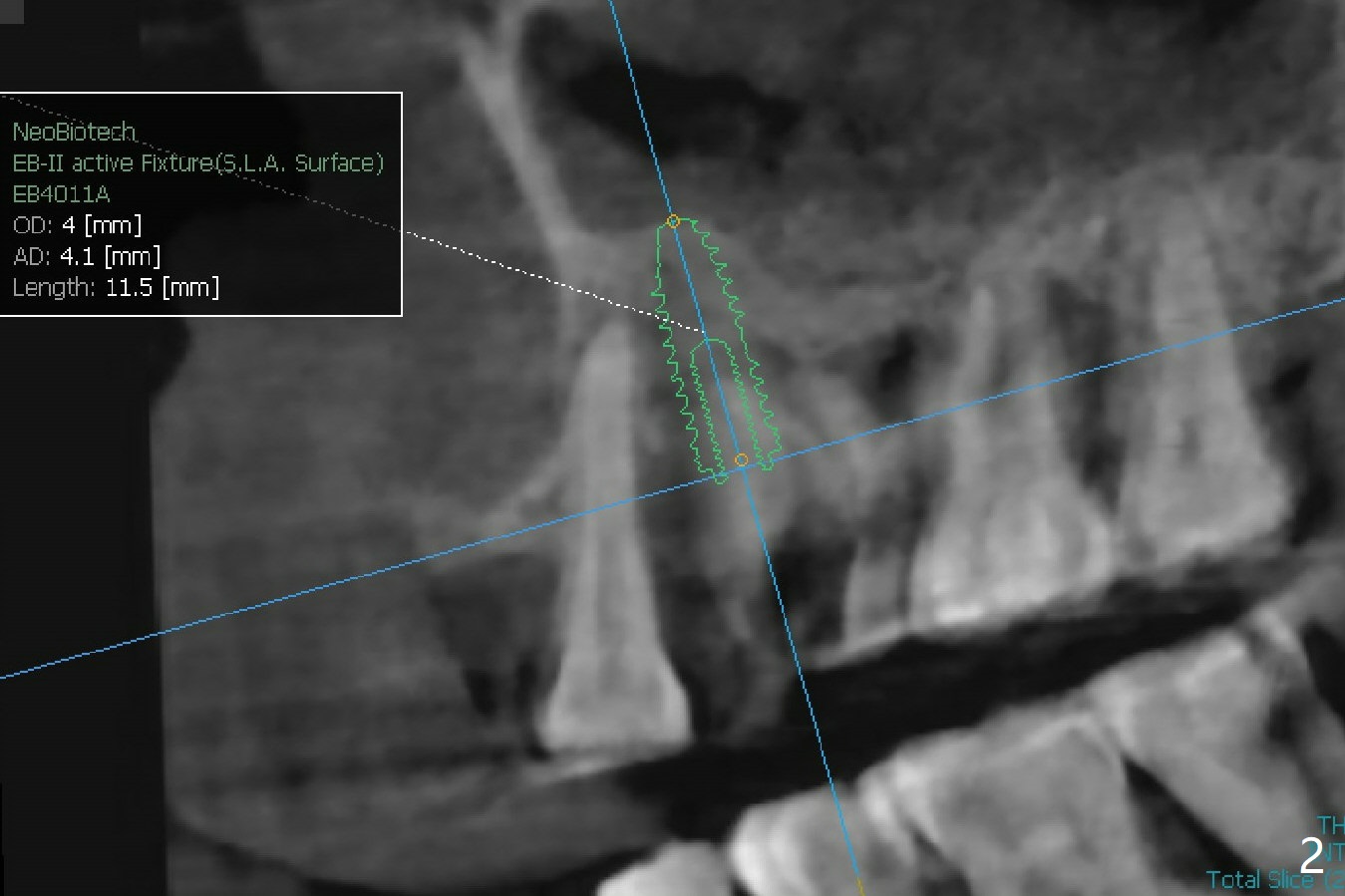
Ideal Trajectory Correction
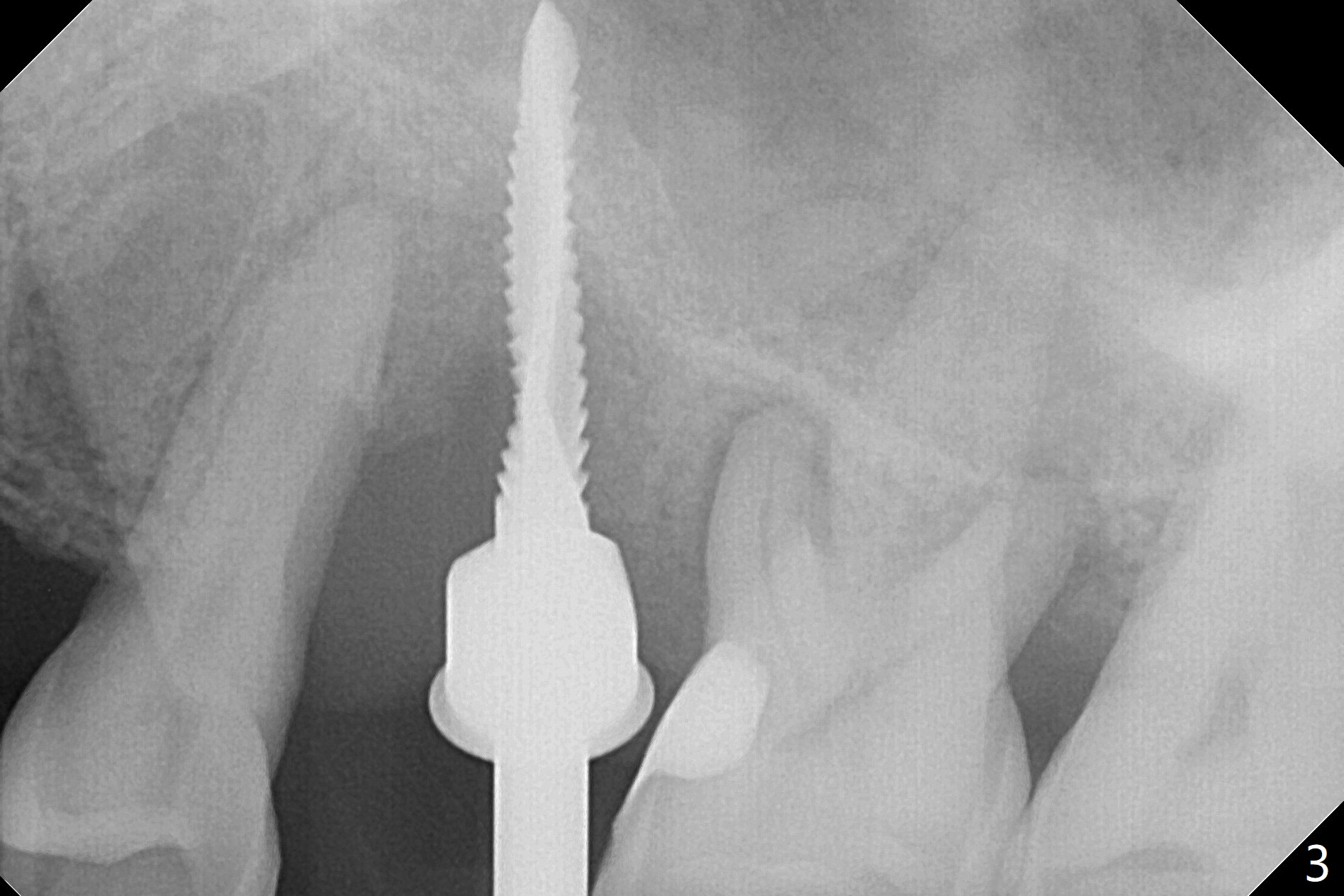
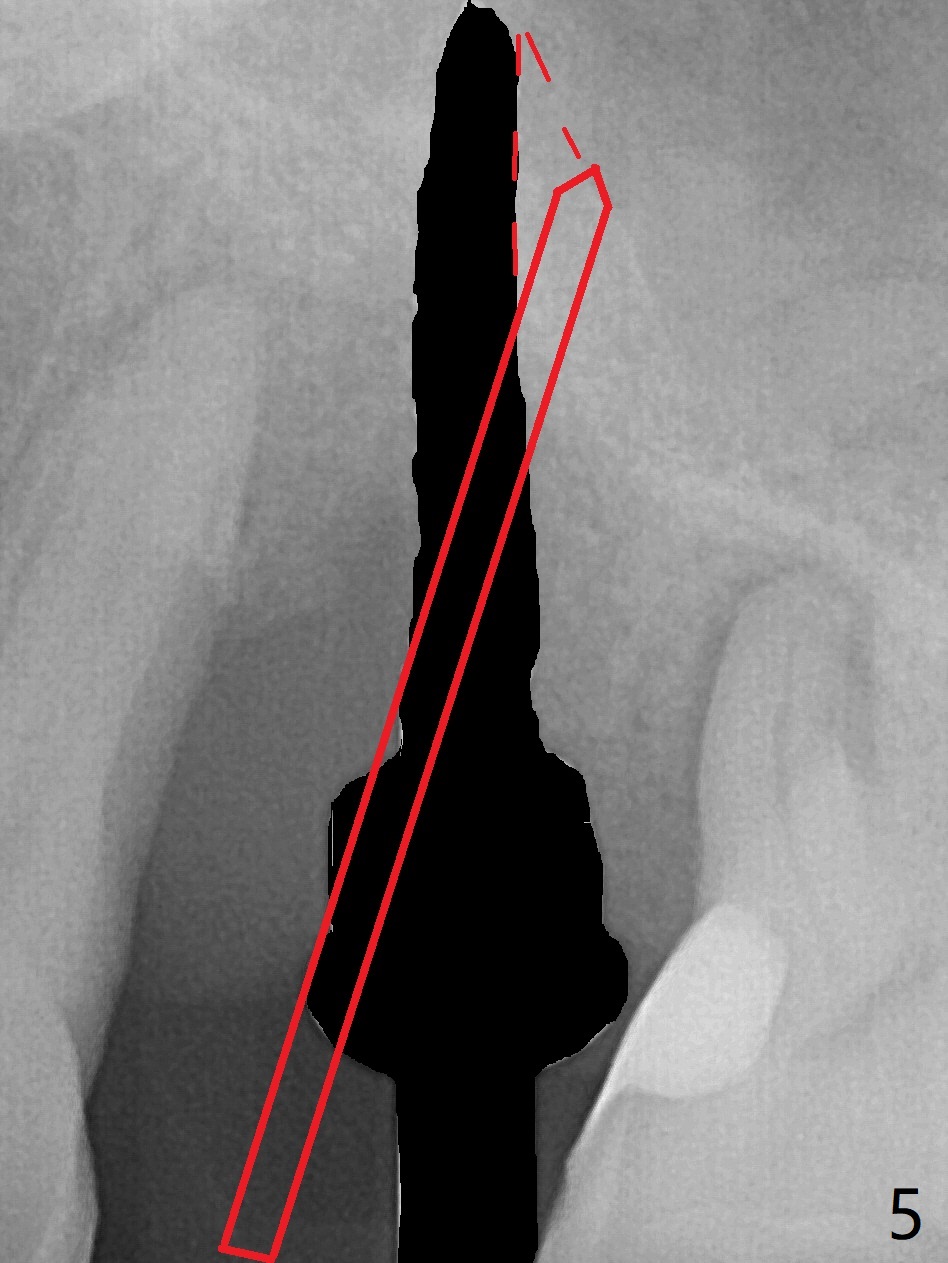
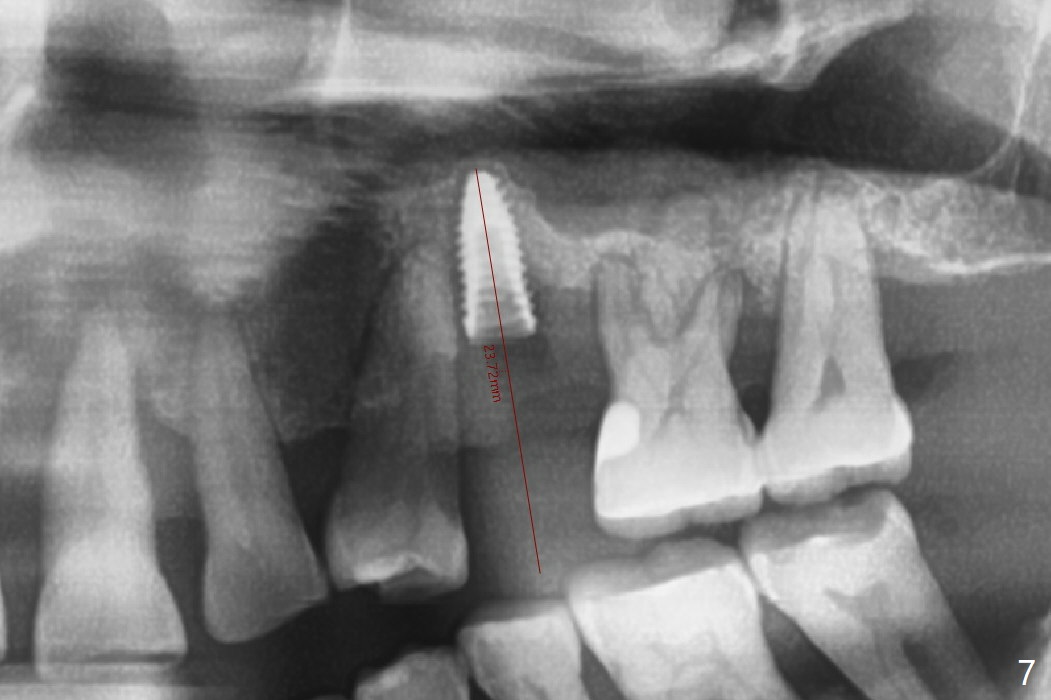
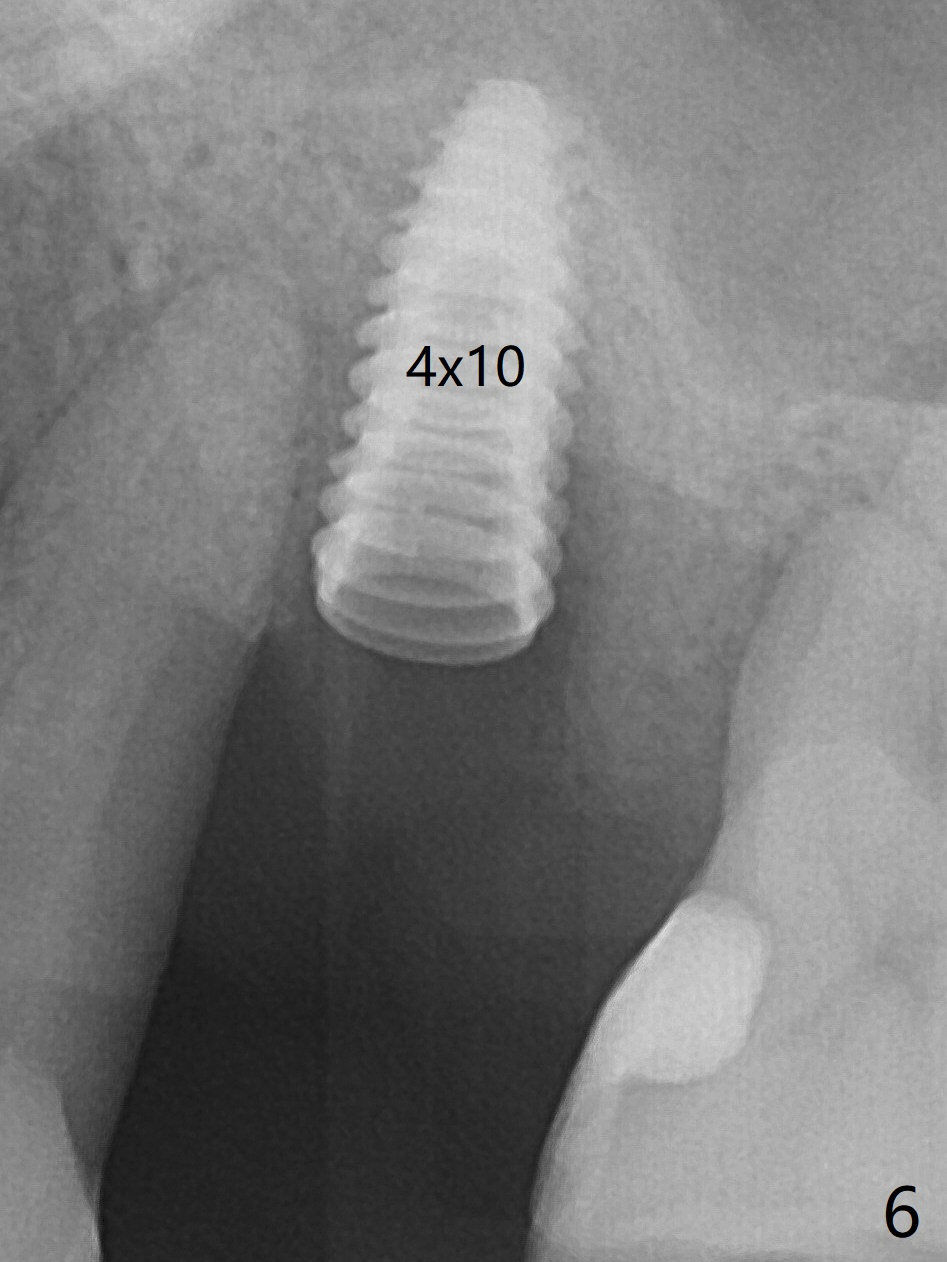
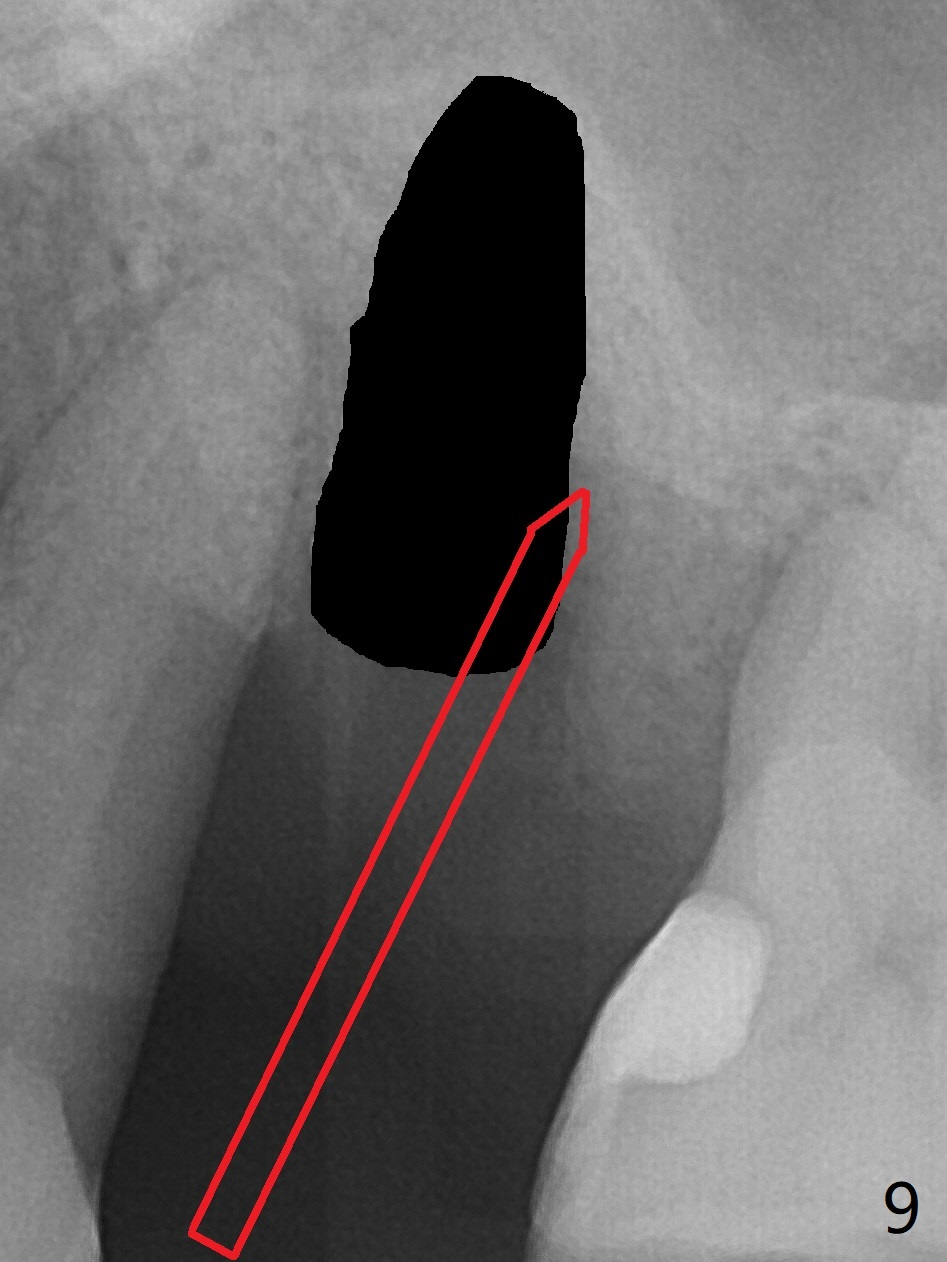
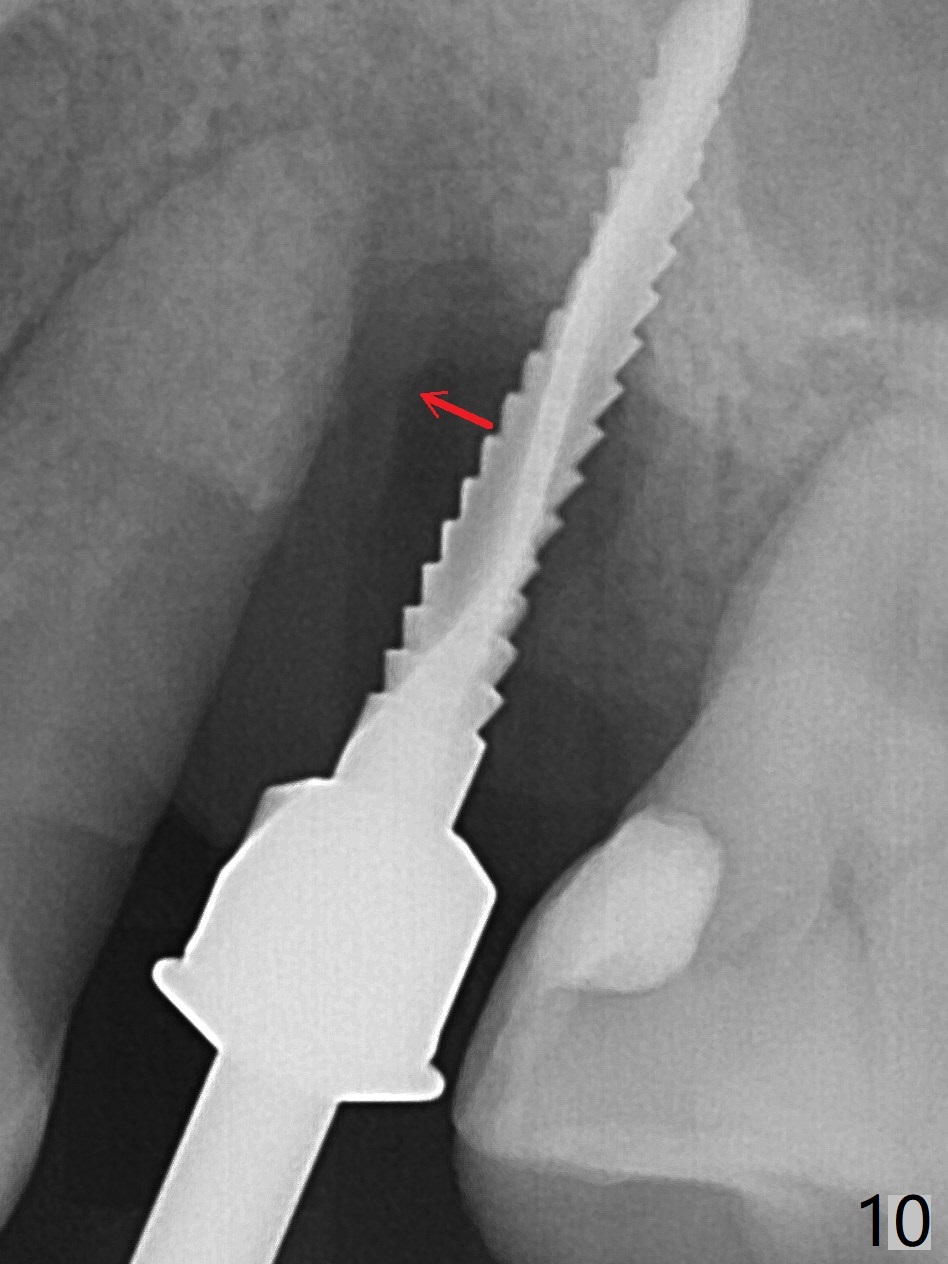
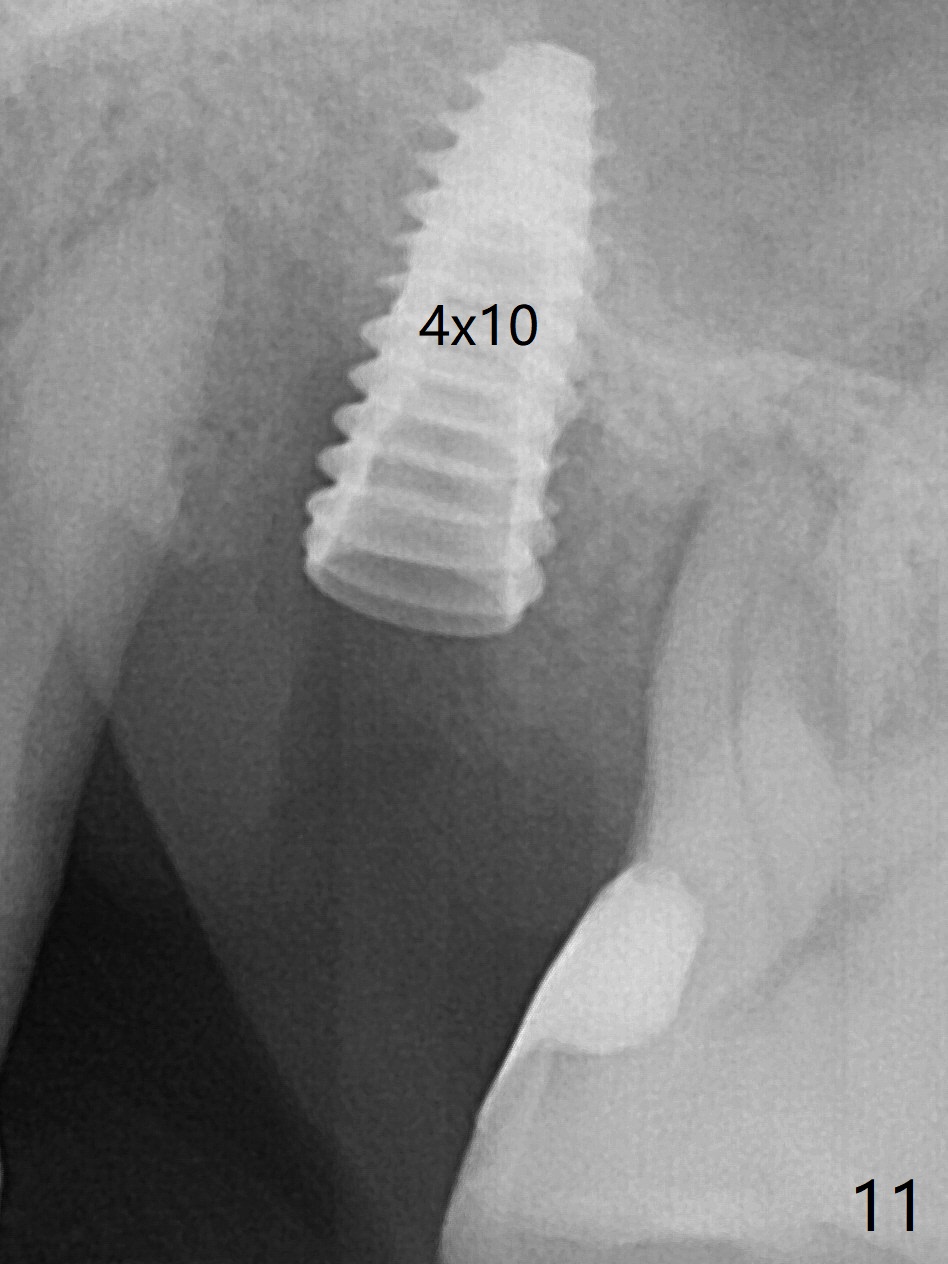
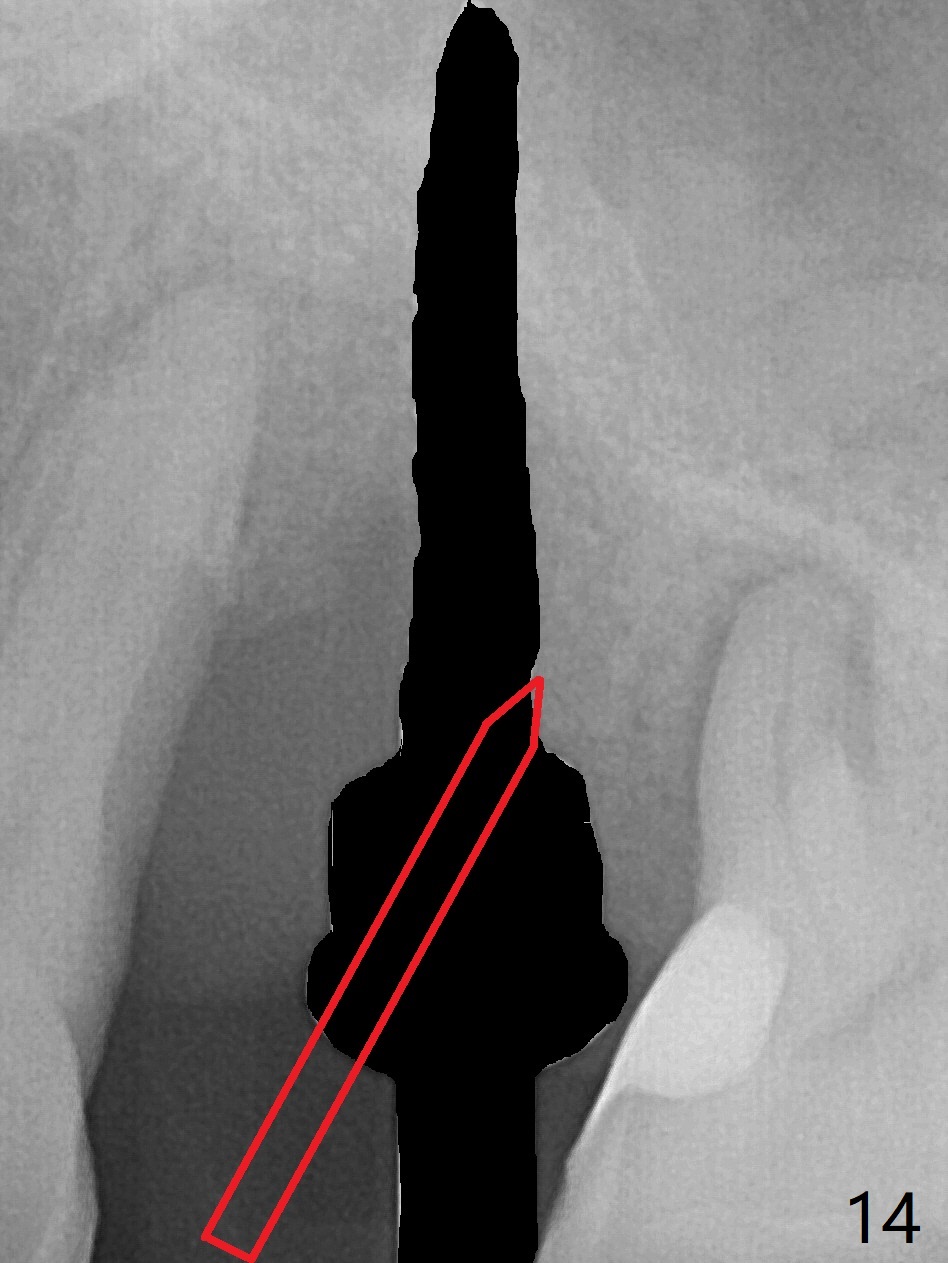
There is more bone apical to the residual root at #13 (Fig.1 red line). An immediate implant along the long axis of the root can be longer, 11.5 mm, favorable for primary stability (Fig.2 (CT taken immediately preop)). The initial trajectory is not ideal (Fig.3). When the pointed/Lindamann bur is removed (Fig.4), effort is made to move the apical end of the osteotomy distal (Fig.5 red arrow) by removing the apical bone (red dashed line). Following sequential osteotomy, a 4x10 mm dummy implant is placed with the trajectory remaining not so ideal (Fig.6,7). As the dummy implant is removed (Fig.8), a new osteotomy is established distal to the existing one (Fig.9). Subsequent drills gradually shift into the original osteotomy (Fig.10 red arrow). When the same dimension dummy implant returns, the trajectory improves with decreased stability (Fig.11). It seems reasonable to place a larger implant without further osteotomy. After placing PRF membrane and Vanilla graft for sinus lift (Fig.13 *), a 4.5x10 mm definitive implant is placed with loss of control in the trajectory (Fig.12,13).
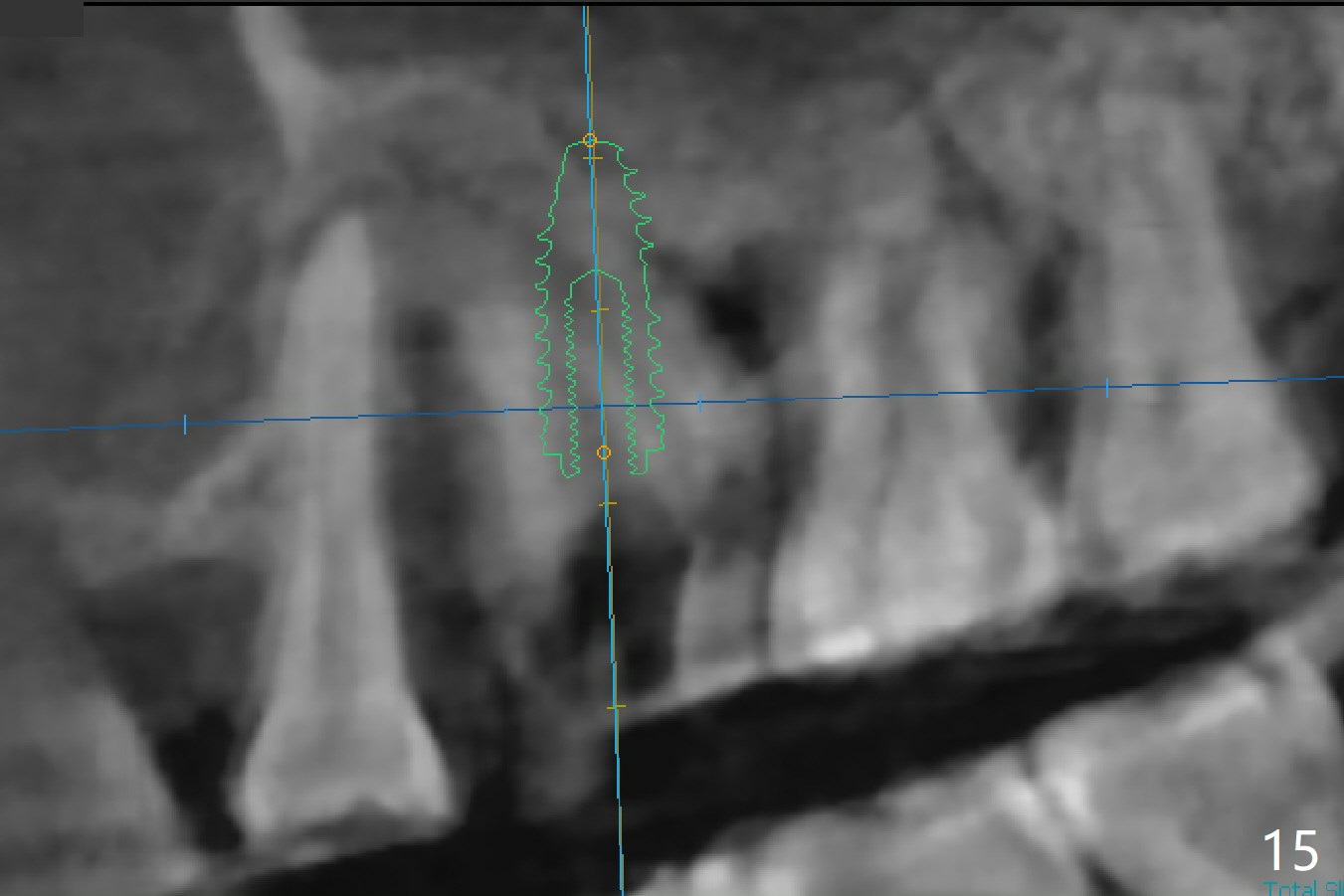
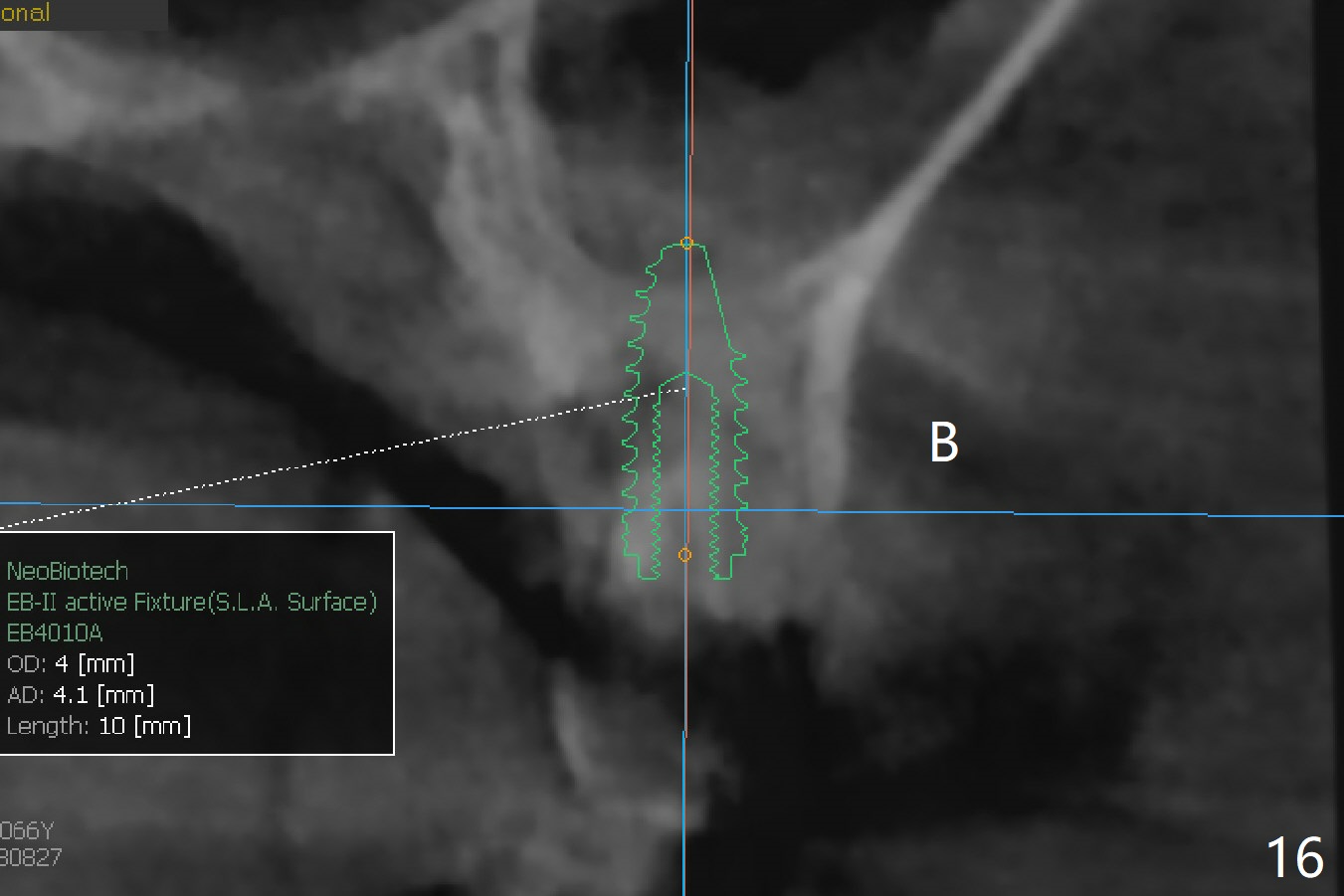
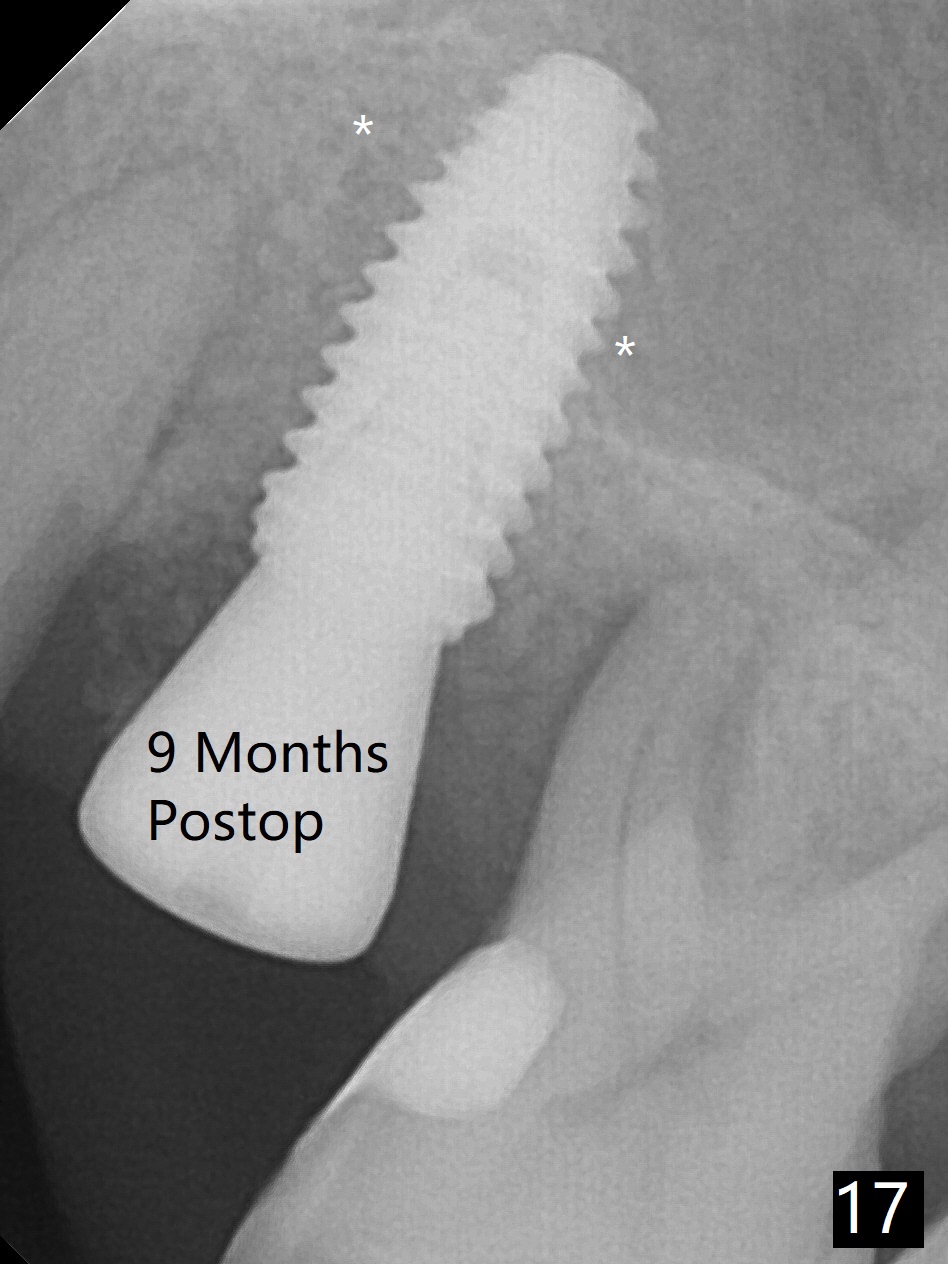
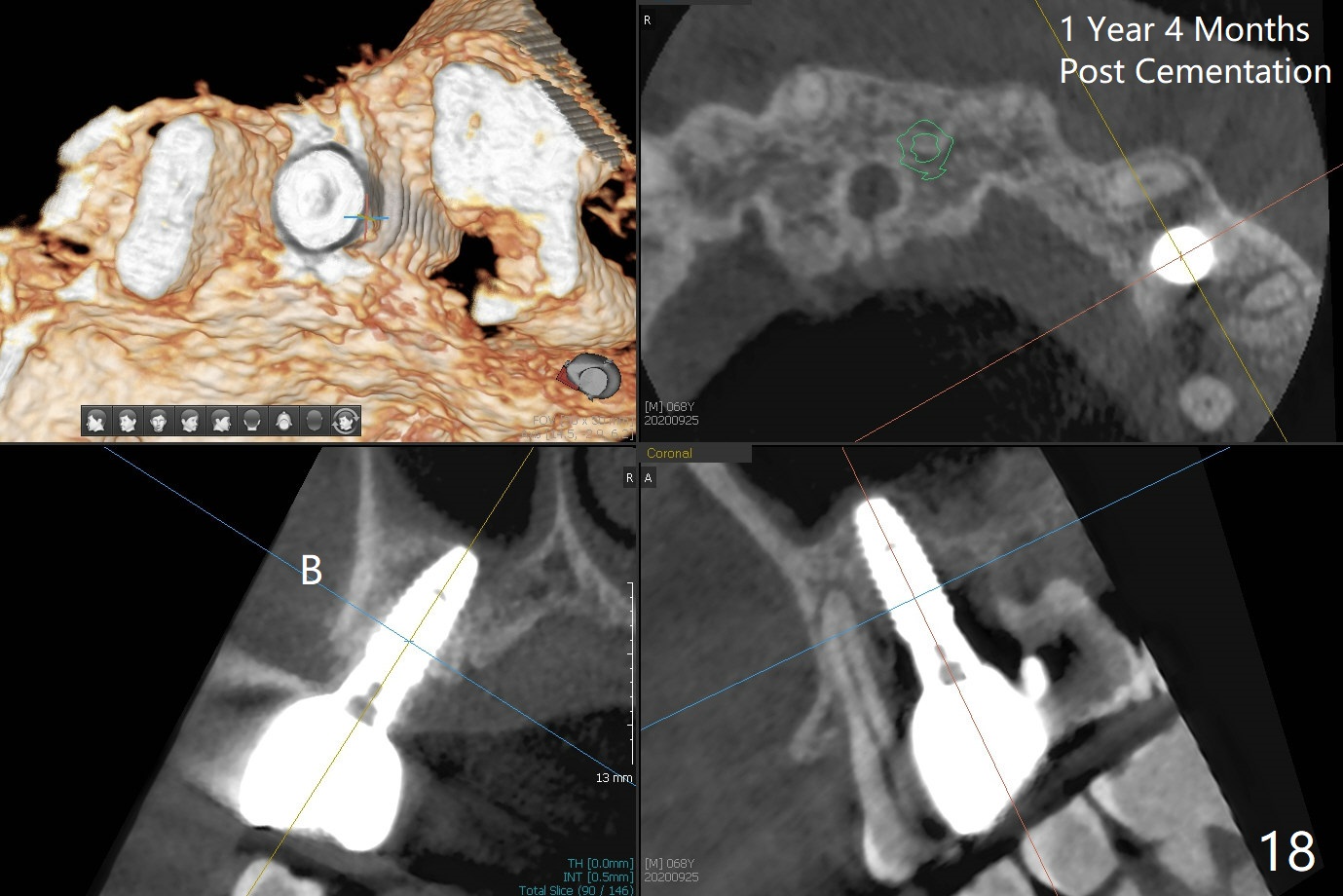
When the initial osteotomy is off substantially (Fig.4), an osteotomy should be established de novo and as early as possible (Fig.14) so that subsequent osteotomy will not relapse to a great extent. More ideally, the initial osteotomy should be planned correctly (Fig.15,16) with sacrifice of the bone height. Nearly 1 month postop, the 4.5x5.5(5) cementation abutment is loose. When it is removed, the patient feels pain from the implant. A 5.5x6 mm healing abutment is placed instead. The implant osteointegrates with trabecular pattern in the sinus 9 months postop (Fig.20 *). The gingiva around the crown at #13 is healthy 1 year 4 months post cementation (Fig.18). Check the distal surface of #13 for bone loss if the tooth #14 is to be extracted.
Return to
Upper
Premolar Immediate Implant, Armaments
9
Xin Wei, DDS, PhD, MS 1st edition 08/27/2018, last revision 09/25/2020