

|
|
|
|
|
||
|
|
|
|
|
||
|
|
|
|
|||
Why to Bury Implant?
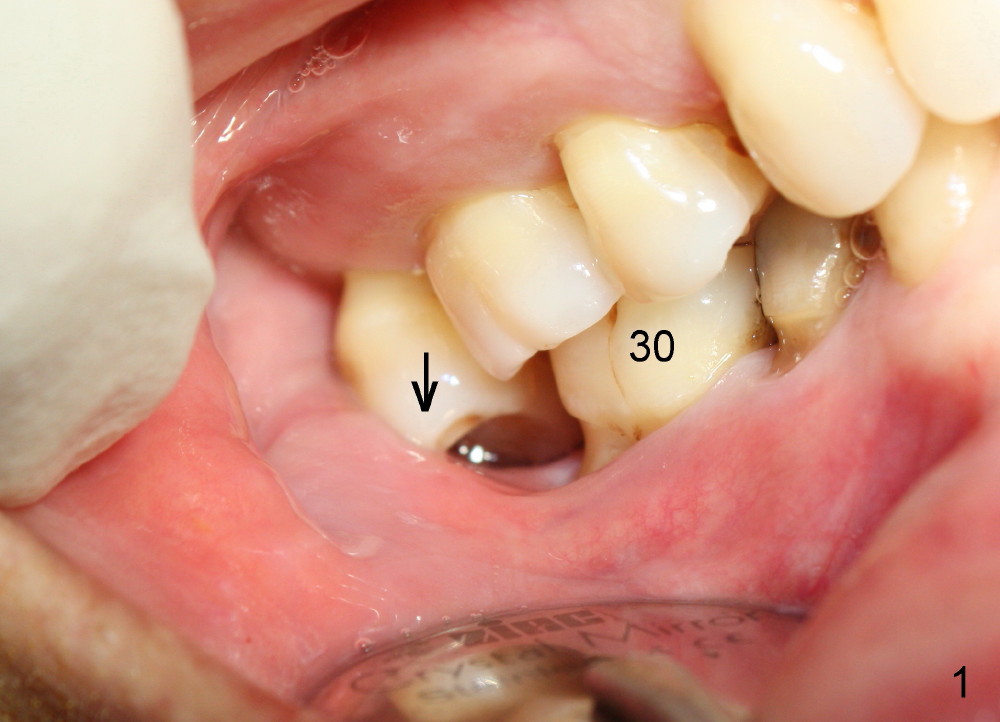
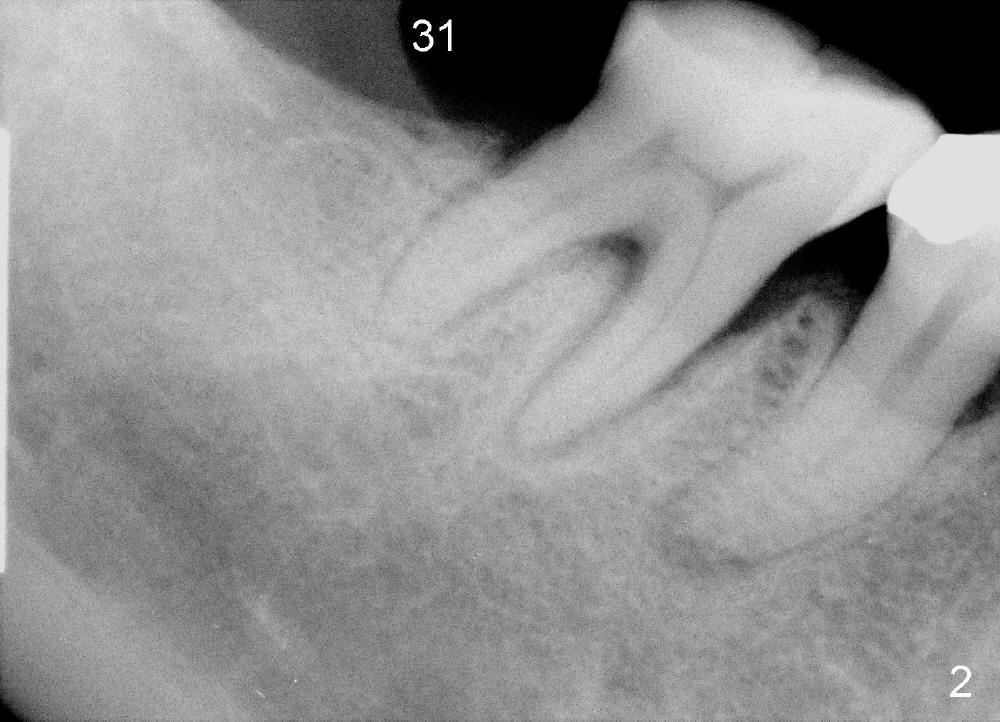
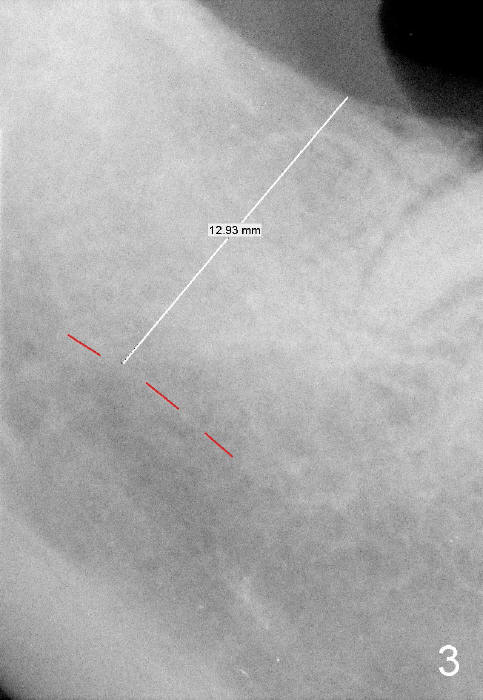
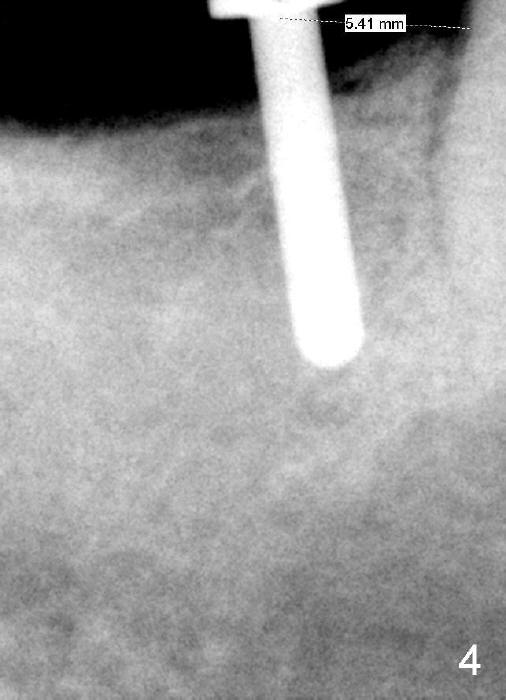
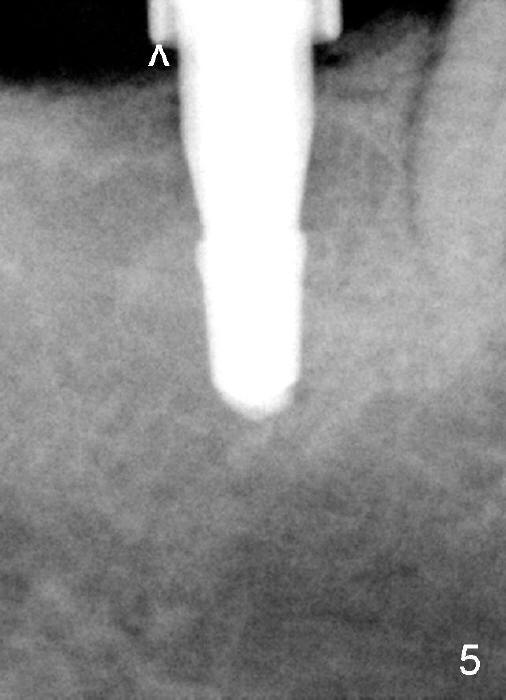
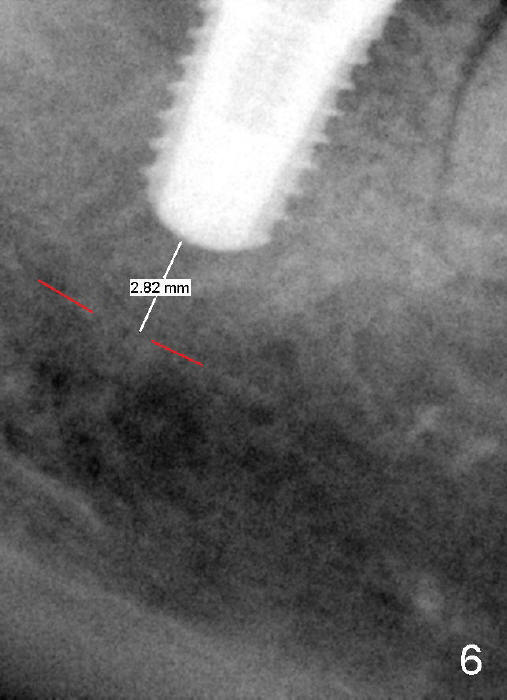
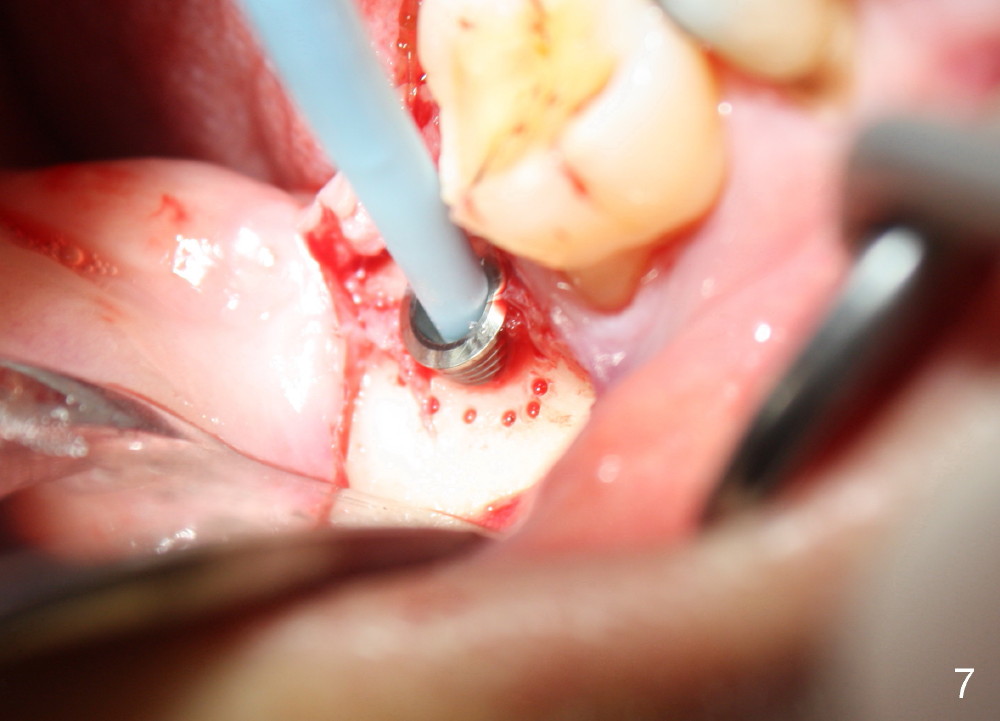
A 57-year-old lady returns for #31 implantation. The vertical edentulous space is limited, as the opposing tooth is supraerupted (Fig.1 arrow). Preop PA is critical (Fig.2), since it is used to measure the bone height (Fig.3: 12 mm). The length of the implant is expected to be 10 mm. The initial osteotomy depth is 8 mm (Fig.4); it appears that the trajectory should be adjusted. Osteotomy increases following depth and angulation adjustment (Fig.5: 4.5x10 mm drill). The submerged implant (5.3x10 mm) is placed with insertion torque approximately 35 Ncm (Fig.6). The buccal microthreads are exposed (Fig.7); to prepare for bone graft, the buccal plate is decorticated. Following placement of freeze dry mineralized allograft, collagen membrane is fixated by a healing screw (Fig.8). The incision is closed by 4-0 Chromic gut sutures and perio glue (Fig.9).
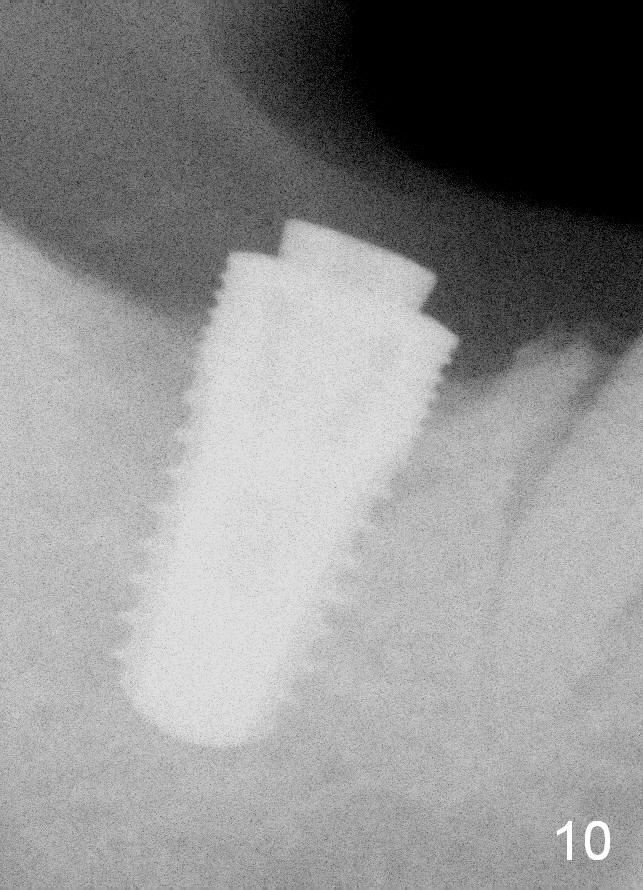
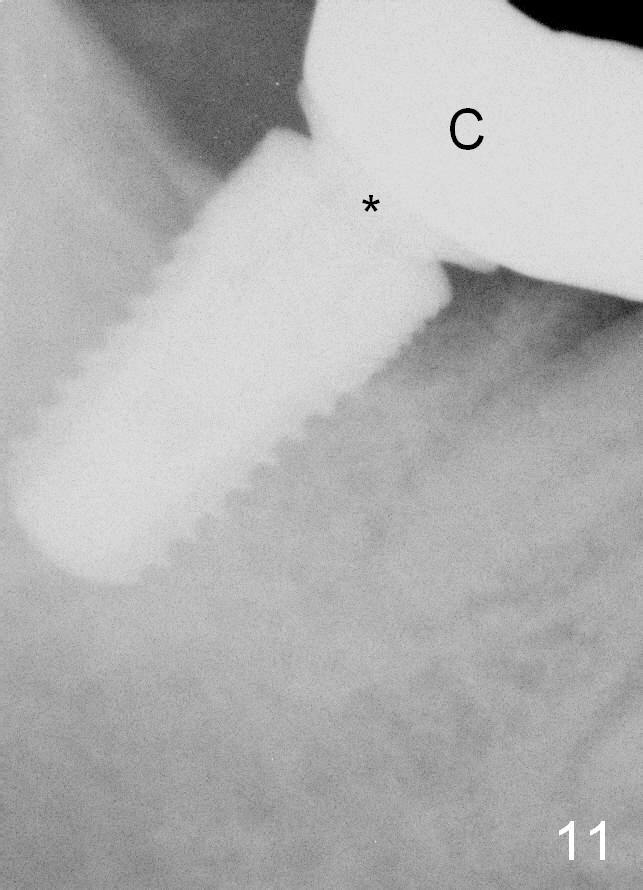
Bone-level implants offer two options after placement (stages 1 and 2). If the insertion torque is high and there is sufficient vertical edentulous space, a healing abutment is placed (stage 1). No surgery is required for restoration. Otherwise, the implant should be buried, as shown in this case. Two mini-implants are going to be placed to intrude the opposing supraerupted tooth. In fact, the orthodontic intrusion is quite difficult. Finally the intrusion apparatus has to be removed prior to chemotherapy for breast cancer. PAs taken 1 year 3 months (Fig.10) and 1 year 9 months (Fig.11, 6 months post cementation) postop appear to show that there is coronal bone loss. An abutment with short cuff (Fig.11 *) is chosen for final crown (C). Ideally the implant should have been placed deeper (Fig.7) for easy restoration. Pre-op examination and diagnosis are critical.
Return to Professionals Dr. Wu Lower Molar Immediate Implant Implant & Ortho 2
Xin Wei, DDS, PhD, MS 1st edition 04/04/2014, last revision 02/19/2017