
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bone Expander Kit
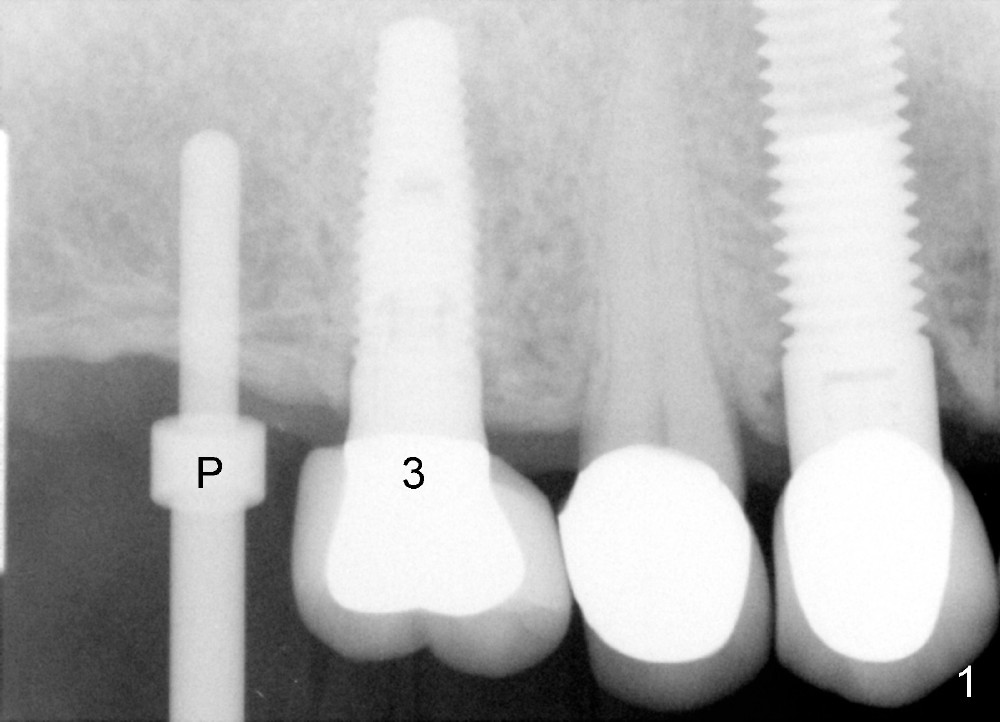
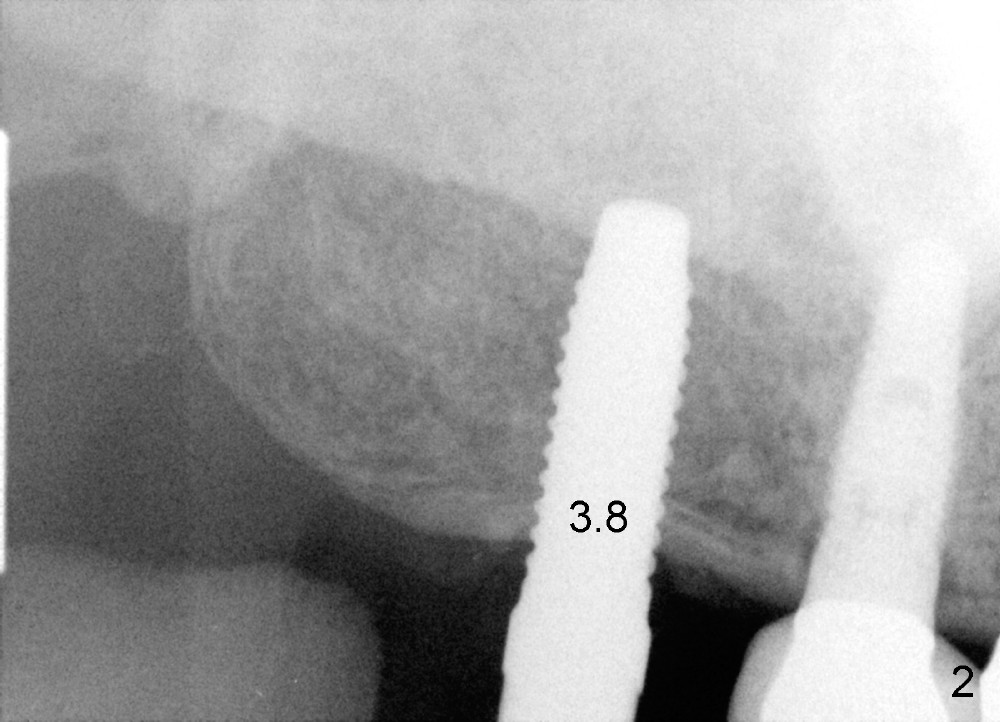
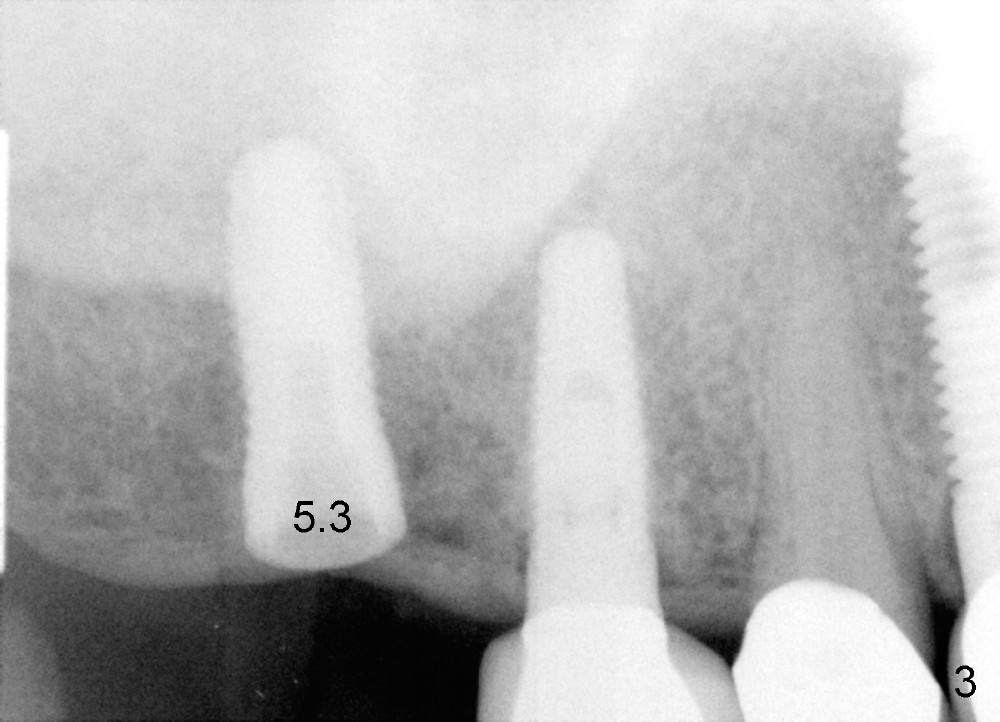
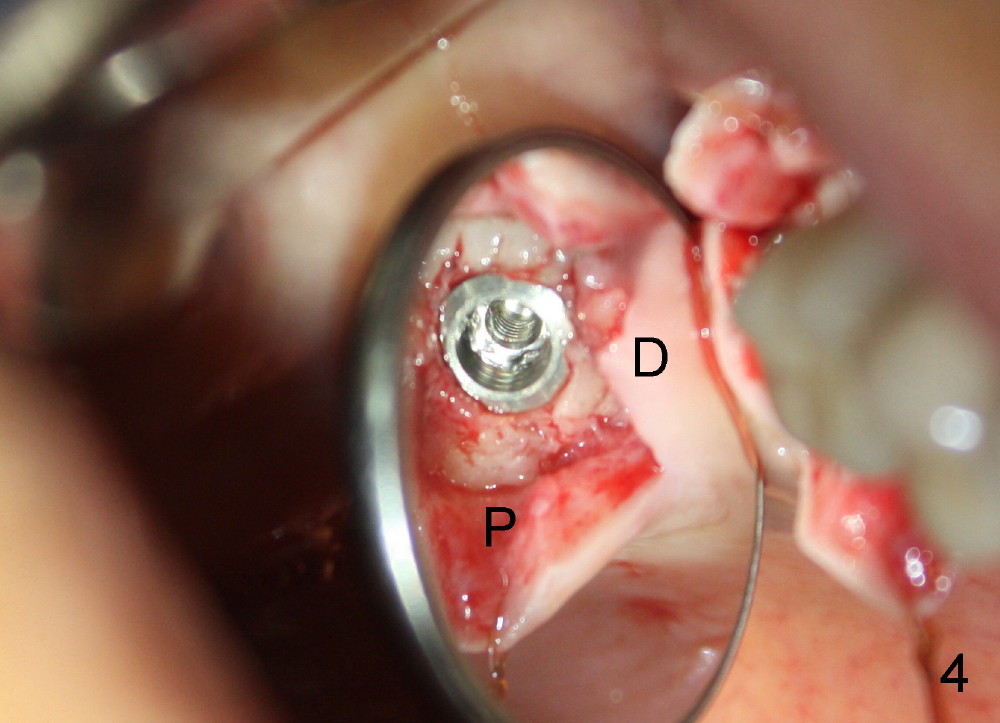
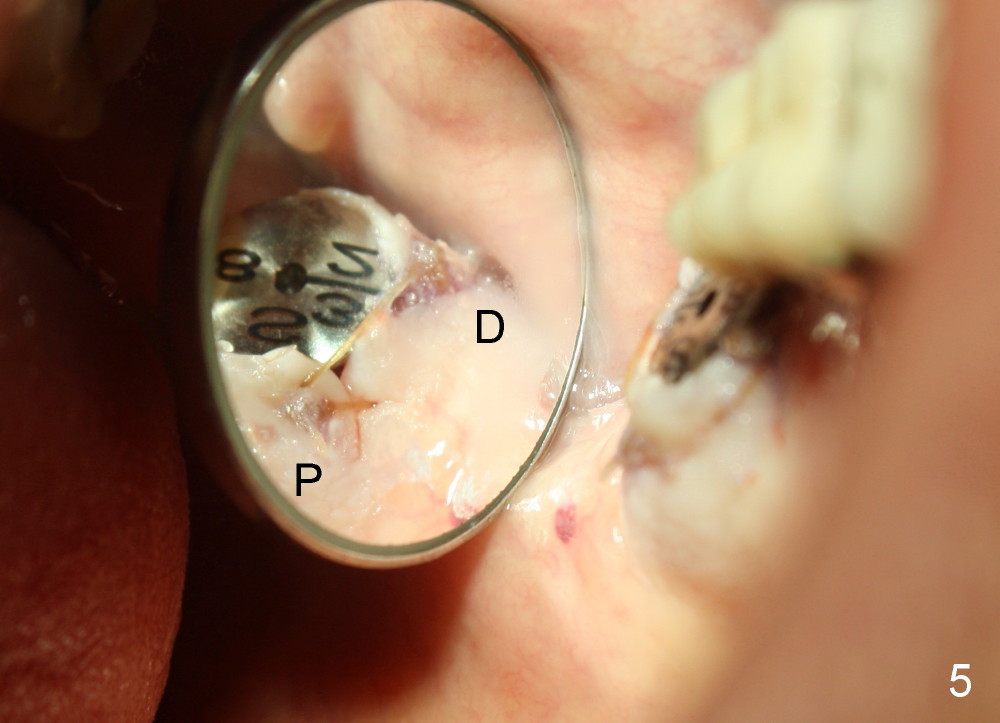
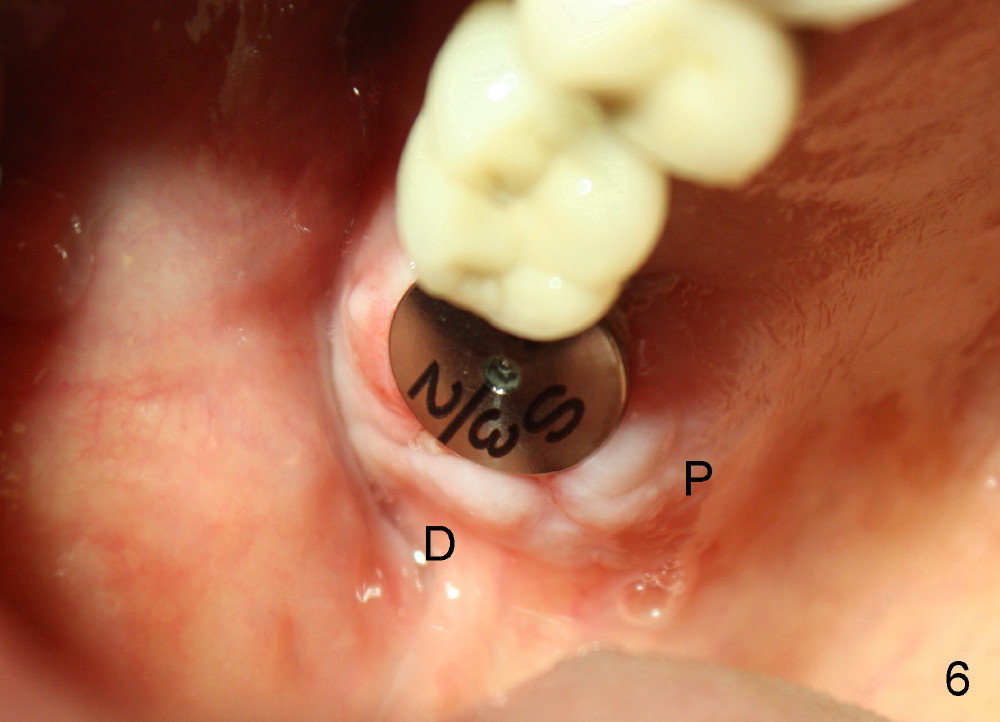
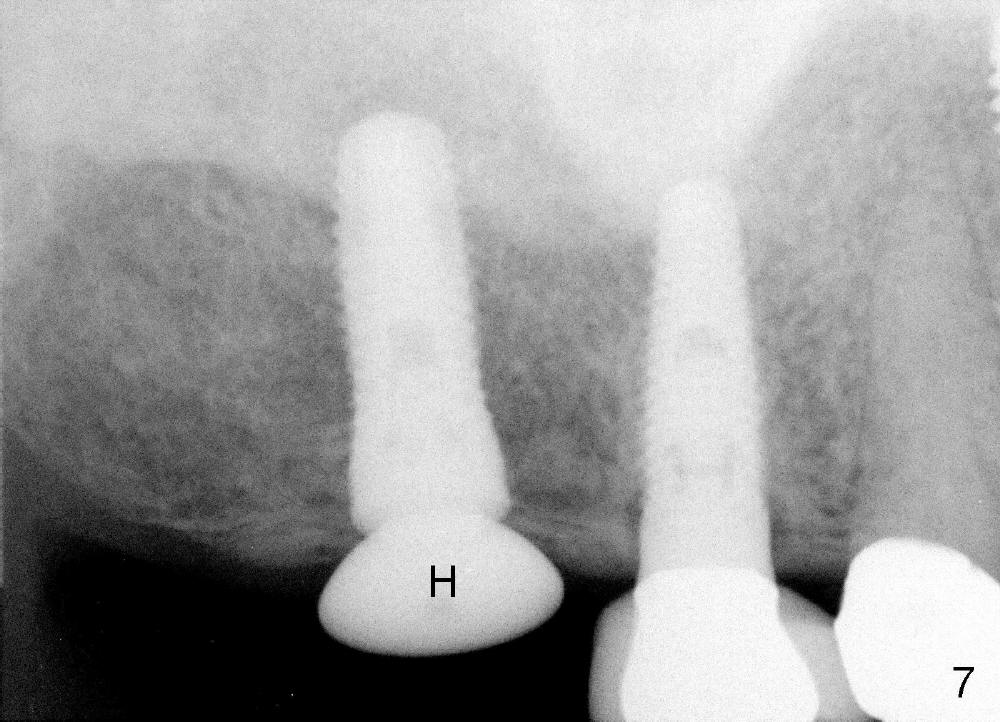
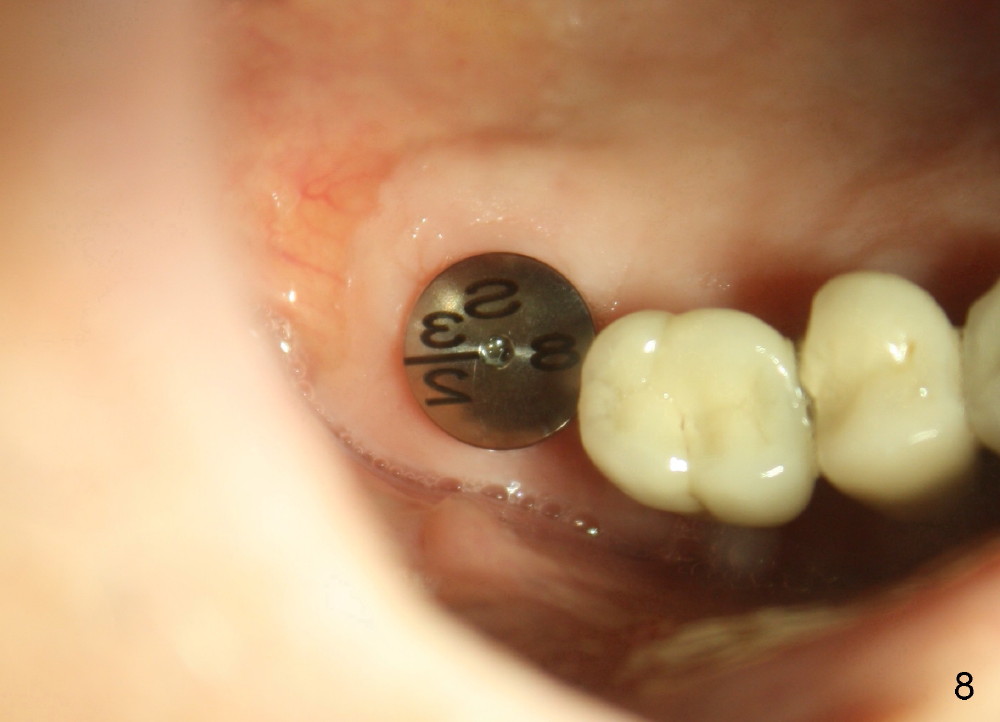
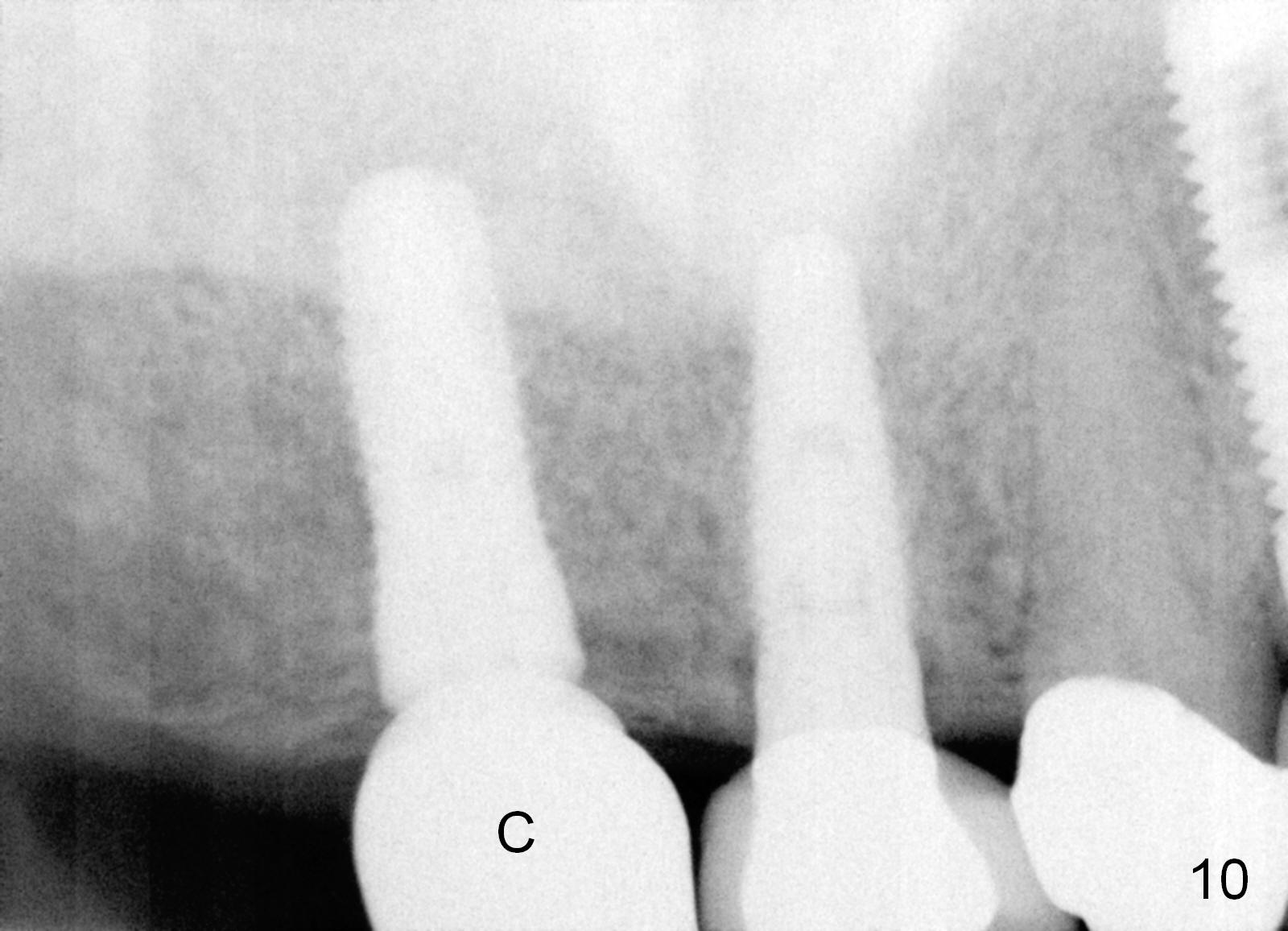
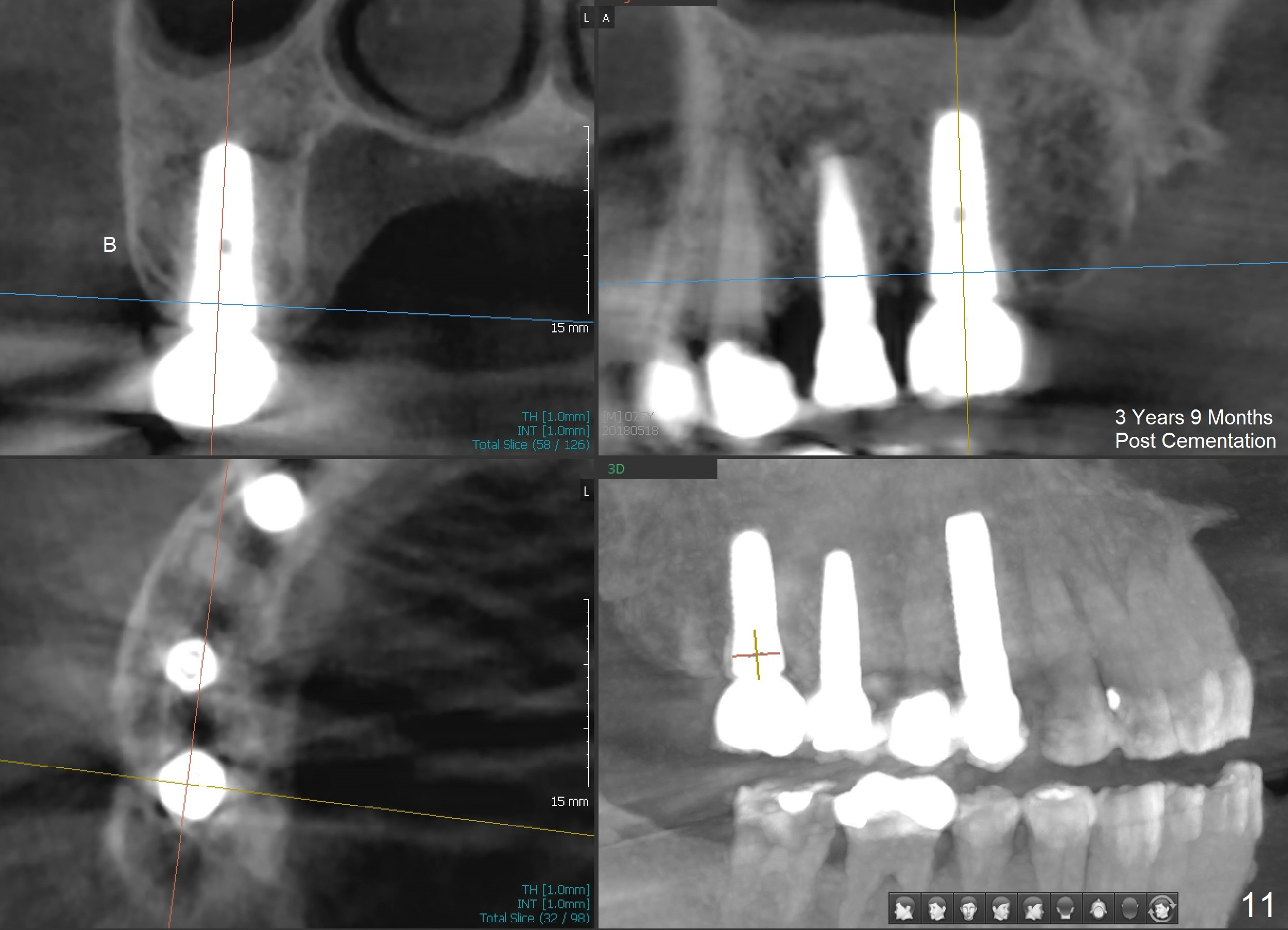
Analysis of preop PA suggests that the density of the cancellous bone is low at the site of the tooth #2. It is confirmed when a 2 mm pilot drill is used to initiate osteotomy. There is no drilling resistance once the pilot drill penetrates the cortex. A parallel pin is inserted for trajectory (Fig.1: P; 8 mm deep). The osteotomy is slightly moved distally with Lindermann bur and enlarged by inserting Bone Expanders from 2.6 to 3.8 mm at the depth of 12 mm (Fig.2). The osteotomy is then intended to move mesially and the depth is increased to 14 mm. Finally a 5.3x14 mm submerged implant is placed with insertion torque ~ 40 Ncm (Fig.3). The implant looks to have been tightly engaged into the bone (Fig.4). In one word, minimal bone removal is required for implant placement in the soft bone, particularly in the maxillary posterior region. A 8.2 mm healing abutment is placed; the flaps are closed by Chromic gut suture and perio glue (Fig.5). The wound heals normally 1 week postop (Fig.6). Fig.7 shows X-ray 3 months postop (H: healing abutment). Soft tissue looks healthy 4 months postop before (Fig.8) and after (Fig.9) removal of the healing abutment for restoration. There is no bone loss 7 months post cementation and 11 months postop (Fig.10 C: crown). It appears that bone expansion prevents bone resorption. There is no bone resorption 1 year 9 months post cementation. The implant is functioning 3 years 9 months post cementation (Fig.11).
Return to Professionals,
Instruments,
Dr. Wu,
#
5, 13
Xin Wei, DDS, PhD, MS 1st edition 05/03/2014, last revision 09/09/2018