




|
|
|
|
|
|
|
|
|
|
|
|
|
|
From 1 Stage to 2
A 43-year-old lady presents to our office for implant 1 month post extraction. Treatment plan is to place a soft tissue level implant (1 stage). The surgery is finished as planned, but there is post-implant infection. The implant is removed with bone graft. Three months post implant removal, the socket heals (Fig.1) with wide ridge (Fig.2). Her oral hygiene remains not so pristine. To reduce the chance of infection, submerged implant is planned (2 stages). Oral Amoxicillin is taken preop.
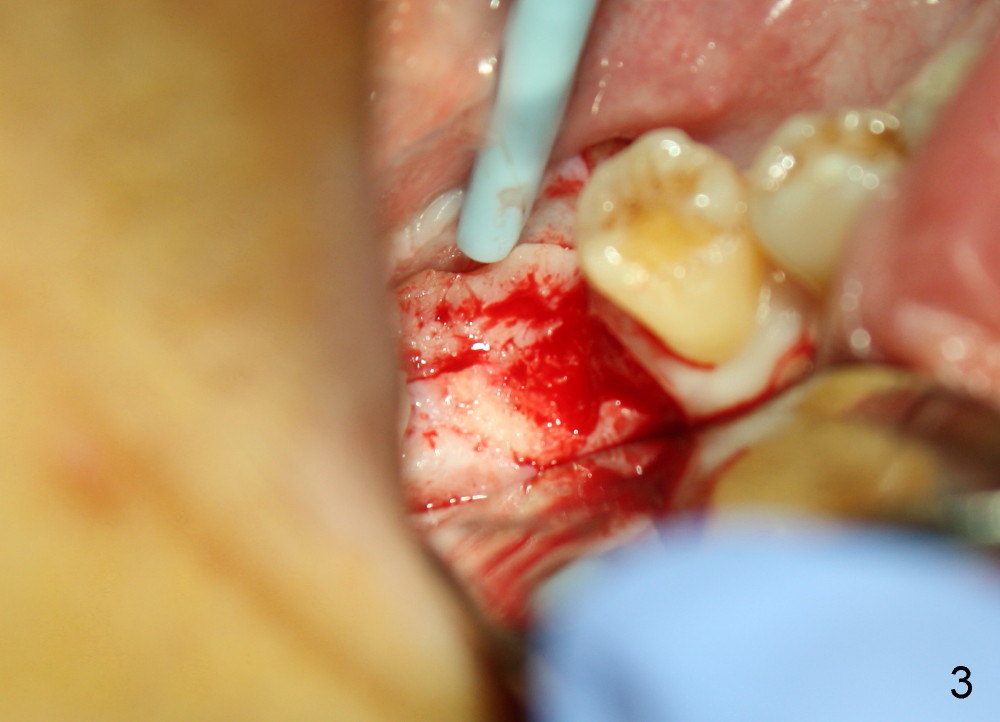
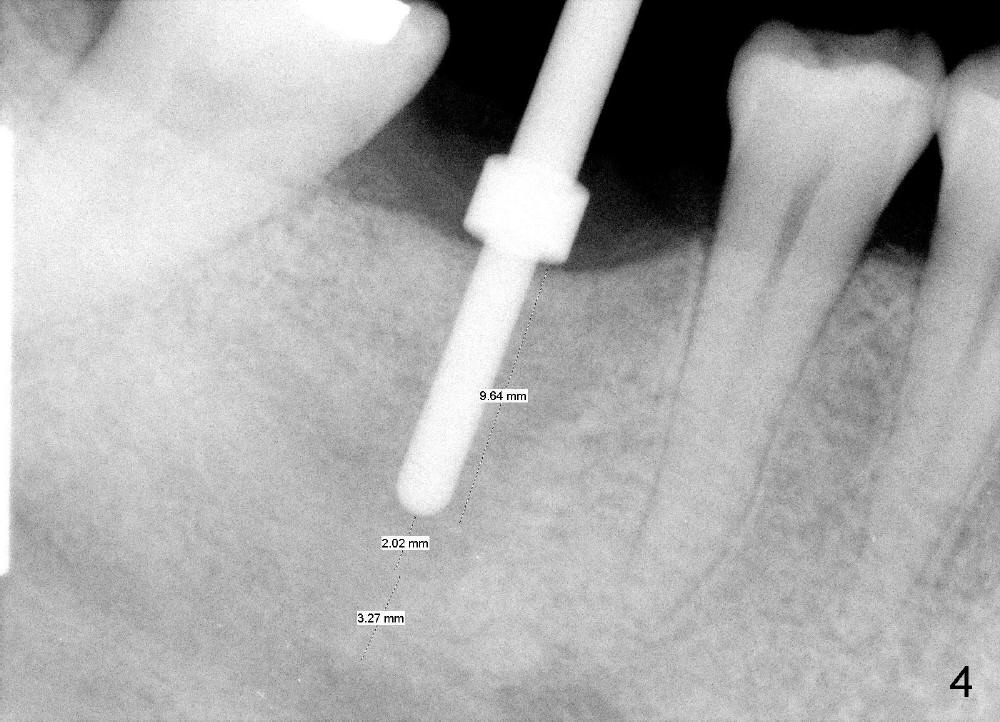
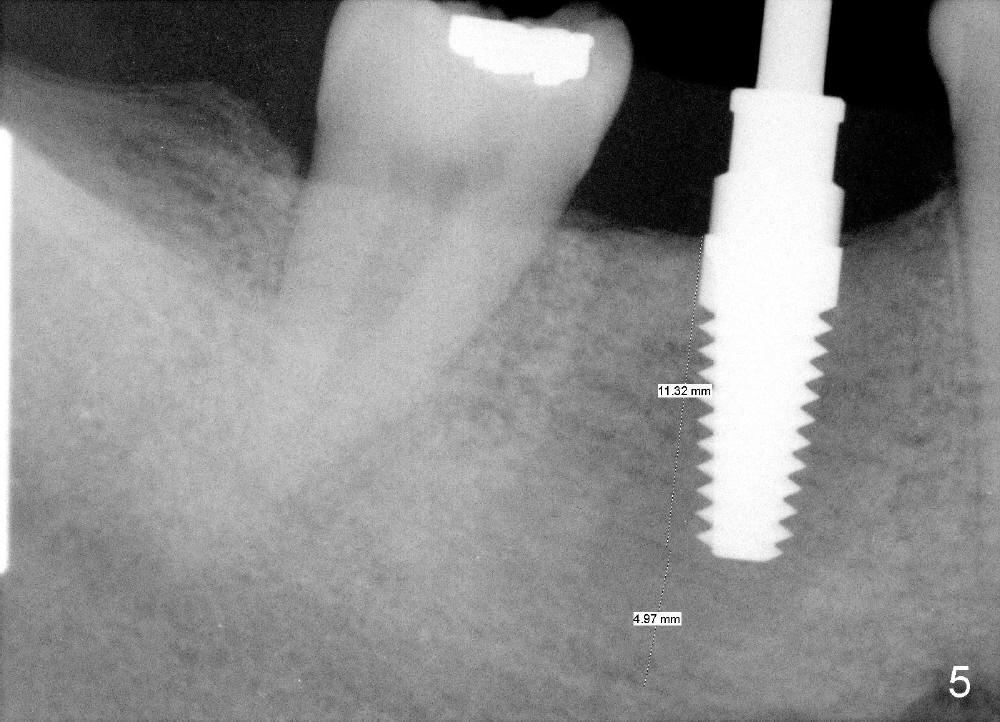
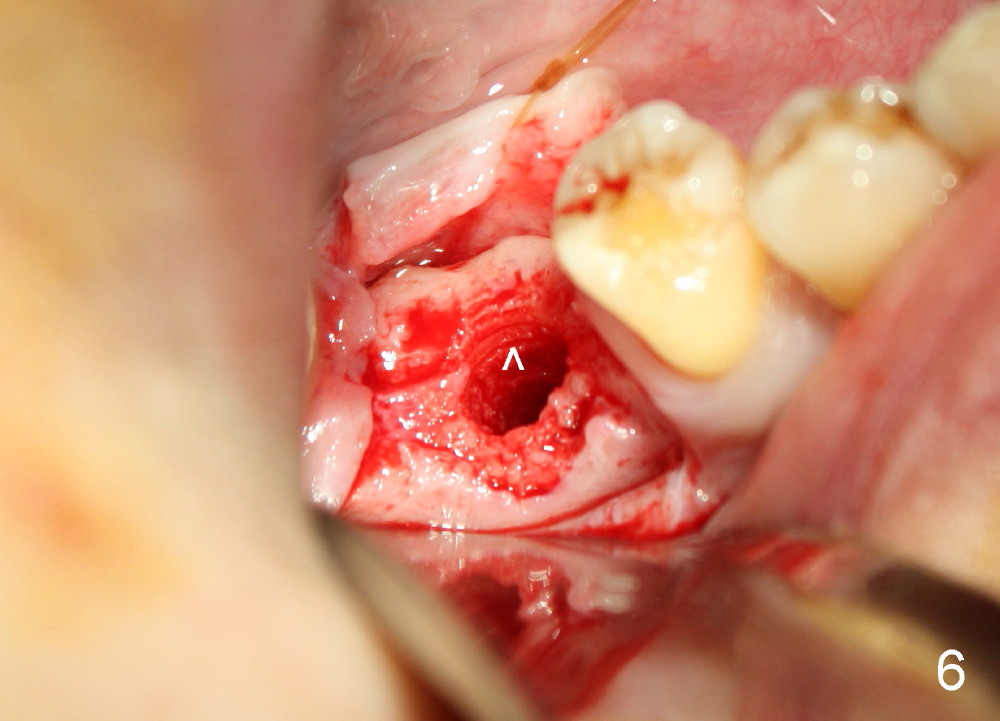
An incision is made instead of flapless, the socket is found to be filled with regenerated bone (Fig.3). After using 2 mm pilot drill, a paralleling pin is inserted to confirm trajectory and distance from the inferior alveolar nerve (Fig.4). Osteotomy is enlarged by Bicon reamers; threads are formed by insertion of Tatum 5x14 mm tap at the depth of 11 mm (Fig.5). The threads are visible when the tap is removed (Fig.6 ^). The advantage of using tap(s) is to test binding to the bone. If the tap is loose, the next sized tap should be used before placing a proper sized implant. This step is particularly critical when placing a large immediate implant or when the socket is immature.
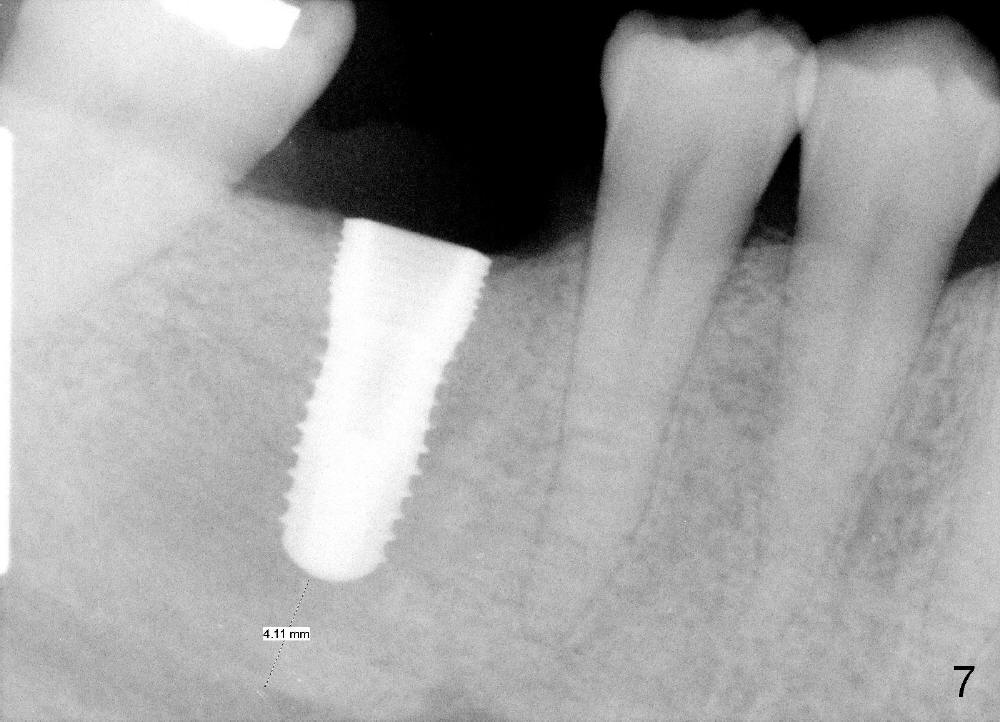
A 5.3x12 mm implant is placed at the crest level (Fig.7,8). The harvested bone from reamers' osteotomy (Fig.9) is placed buccal and lingual to the implant, where there is a half or 1 exposed microthread. The bone graft is then covered by collagen membrane. The periosteum is underscored; the flaps are sutured. The wound is covered by perio dressing. The patient continues postop oral antibiotic.
The wound is healing without symptom or sign of infection 9 days postop (Fig.10). The patient returns for uncover 6.5 months postop.
Xin Wei, DDS, PhD, MS 1st edition 01/30/2014, last revision 01/19/2018