
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Implant & Ortho 2 | |
Mini Journey
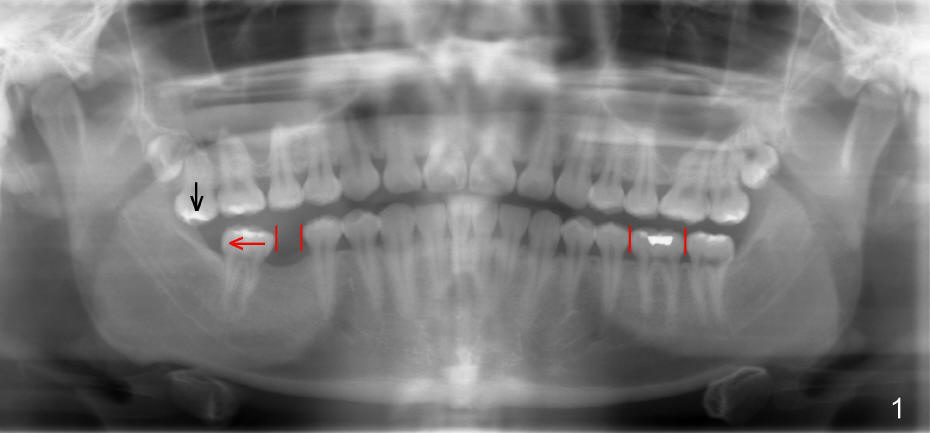
Twenty-year-old man requests restoring missing tooth #30 (Fig.1), but the edentulous space (red lines) is narrow as compared to the mesiodistal width of #19. Ideal treatment plan is to distalize #31 (red arrow) with mini-implant (mini in short) and restore the missing tooth with traditional implant.
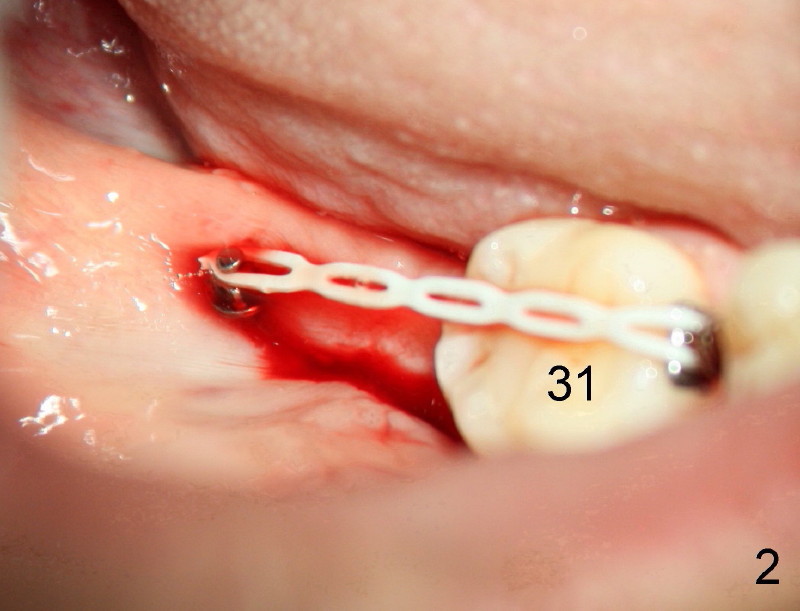
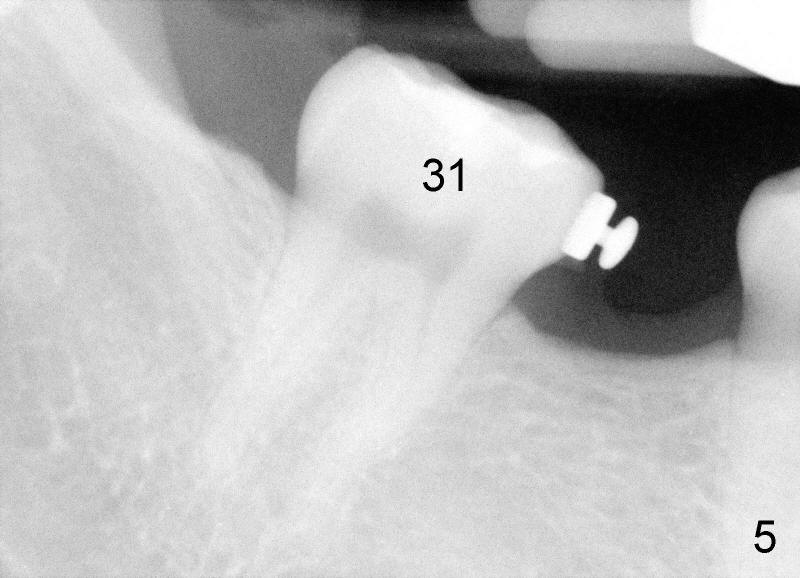
Small incision is made in the retromolar area. Pilot drill is used before a 10 mm Ancor Pro Mini-implant is placed (Orthoorganizer). But it is too loose. Incision is extended distally. With shallower pilot drilling, the next placement of mini is stable (Fig.2). With placement of lingual button on the mesial aspect of #31 and power chain (Fig.2,5), the journey of distalization begins. But it is not so easy as expected.
For 10 months, there is no sign of movement in spite of the effort to tackle supraeruption of #2 (Fig1. black arrow). First, composite is placed on occlusal surface of the left molars for several occasions. It is worn off quickly. Incisal guidance is made. Probably the kid does not wear it constantly. Occlusal reduction is also tried for #2.
Finally Dr. Tim Shaughnessy (orthodontist) is consulted. Two mini should be placed to intrude #2 first. Chinese proverb says that listening to one piece of advice from an expert is better than reading thousands of books by yourself. Second phase of mini-implant journey embarks with pleasure.
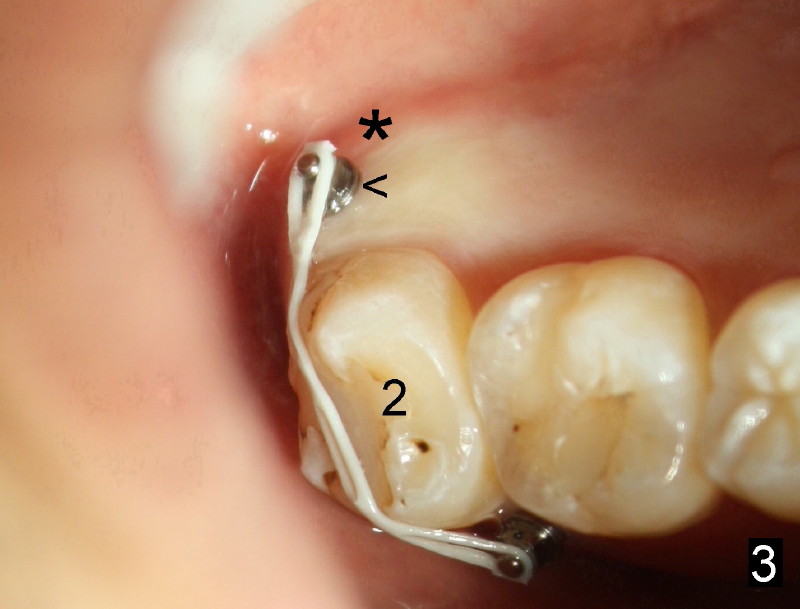
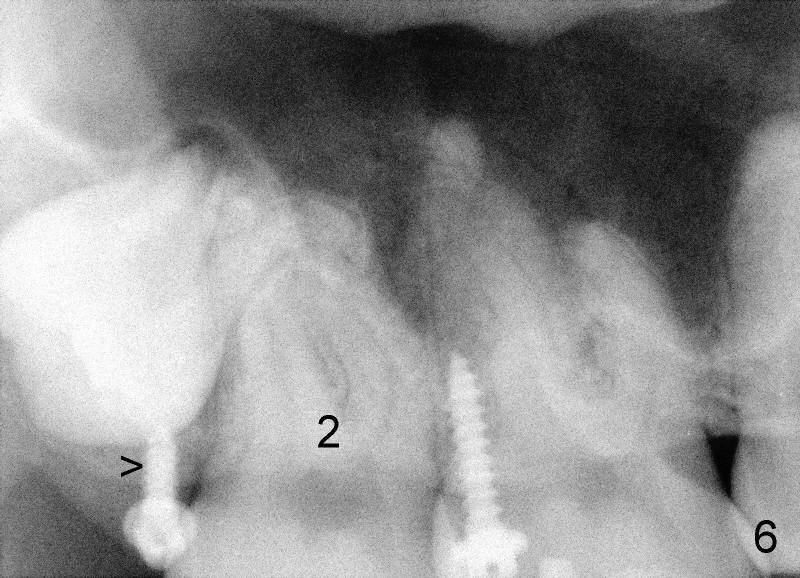
Eight mm of Ancor mini-implant is placed on the mesiobuccal of #2, whereas 6 mm on distopalatal (Fig.3,6 <) without sign of hemorrhage. But a few days later, the patient's father calls, saying that one of mini is out (palatal). The palatal mucoperiosteum is thicker than buccal. Longer mini-implant should have been used (8 or 10 mm). The excuse for short mini in the palate is that there is not much soft tissue (presumably hard tissue) distal to #2. In fact, the patient is dental phobic. Who will faint first dealing with the fearful patient for the same procedure for a second time?
Fortunately, the kid is getting more mature each time. He is pleased to hear that no needle is needed. Another mini company (Tomas, Dentaurums) recommends topical and no incision for mini. Without local anesthesia, the patient may feel pain if a long mini is touching root surface. To get decent anesthesia, Cetacaine (a topical usually used for laser) is applied to the mucosa for prolonged period of time. A 10 mm Ancor mini is loaded in a 16:1 reduction slow-speed handpiece driven by air turbine. The mini penetrates the mucosa without incision or pilot drill. Judged by healed wound, the new mini is placed more mesioapical than the earlier one (Fig.3 *) in hope to catch bone. It appears that the whole hard palate has attached gingiva. The portion near the teeth has thicker gingiva. Mini should be placed in thick gingiva to reduce tissue reaction.
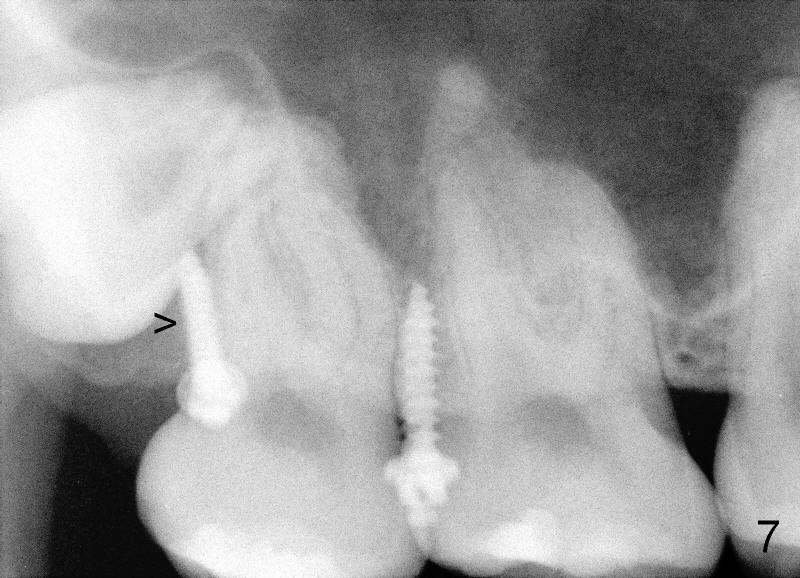
Mini penetration does create soft tissue shaving, which may cause epithelial entrapment and therefore potential mini loosening. At time of placement, it is a minor issue, in comparison to violation of root surface. As the mini goes down, torque builds up. Finally the handpiece halts. Then use a wrench to slowly rotate the mini down while watching for patient's reaction. It appears that the mini eventually has resistance (touching root surface?). The mini does not seat completely (Fig.4 >, as compared to Fig.3 <), but it is solid. When power chain is loaded, it is apparent that the patient feels more pressure upon #2. The patient tolerates the procedure with topical well. It feels like that champagne is needed for celebration. Sweeter is taking and looking at immediately post-op PA (Fig.7 >).
The good things about mini is that if mini does not catch the bone (stability), counter-rotate it, find a new spot and do it again until you hit home run (Fig.2). The wound heals uneventfully in spite of bloody field. Since the maxilla has spongy bone, pilot drilling is not required. The palatal root of the maxillary molar is narrower mesiodistally than buccal. Therefore, mini can be placed a little bit closer to the palatal root than buccal. The tip of mini is directed apically so that there is more room for placement.
Mini journey is not so easy, but the result is amazing. In probably one year, final results will be obtained for this case. What happens if mini touches the tooth #1 and/or #2? Volunteer extraction is provided. The patient's father does not think necessary to keep #2 anyway.
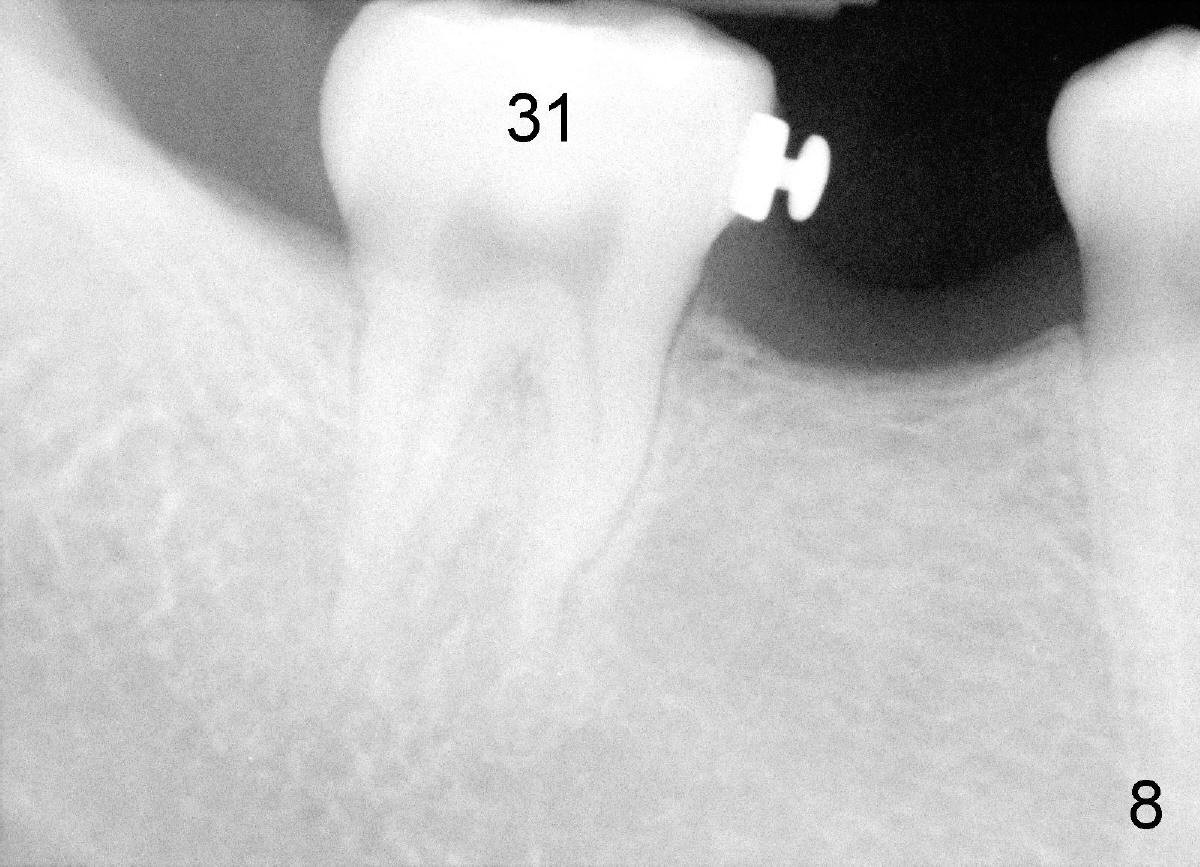
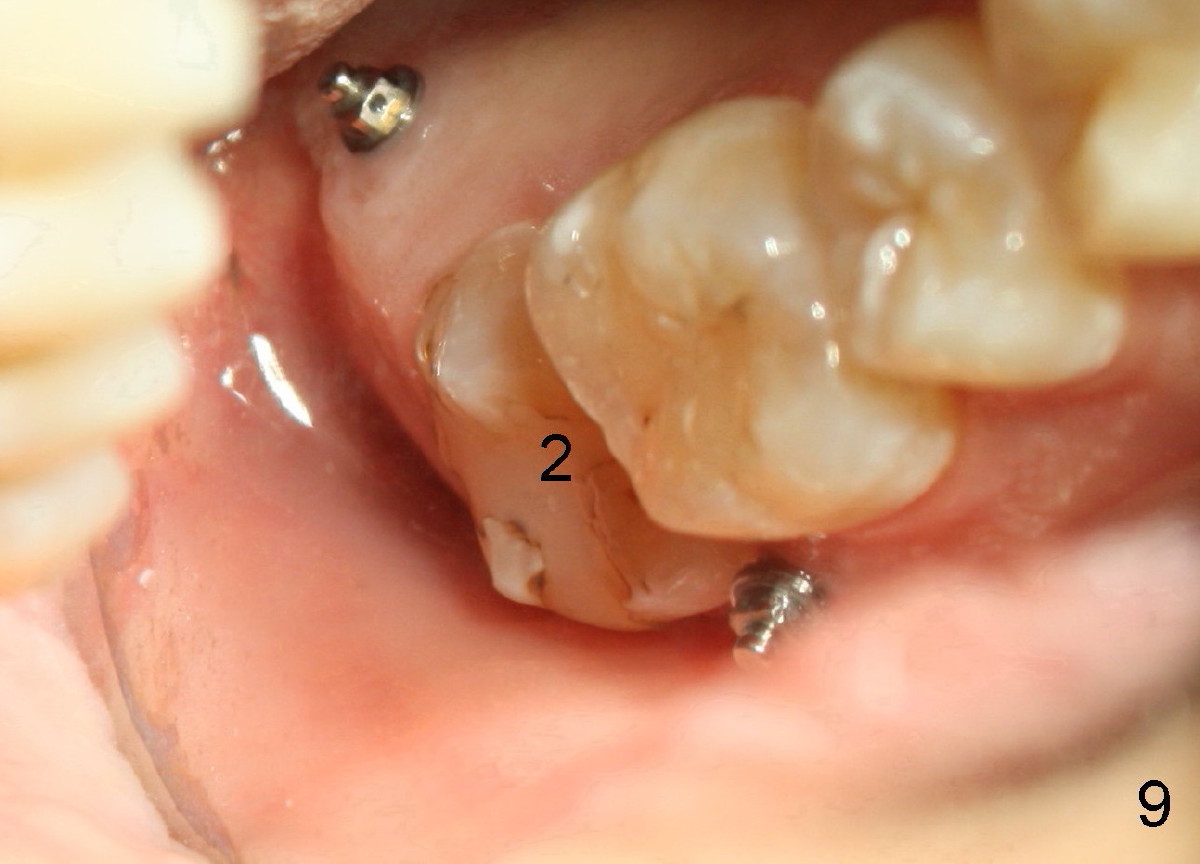
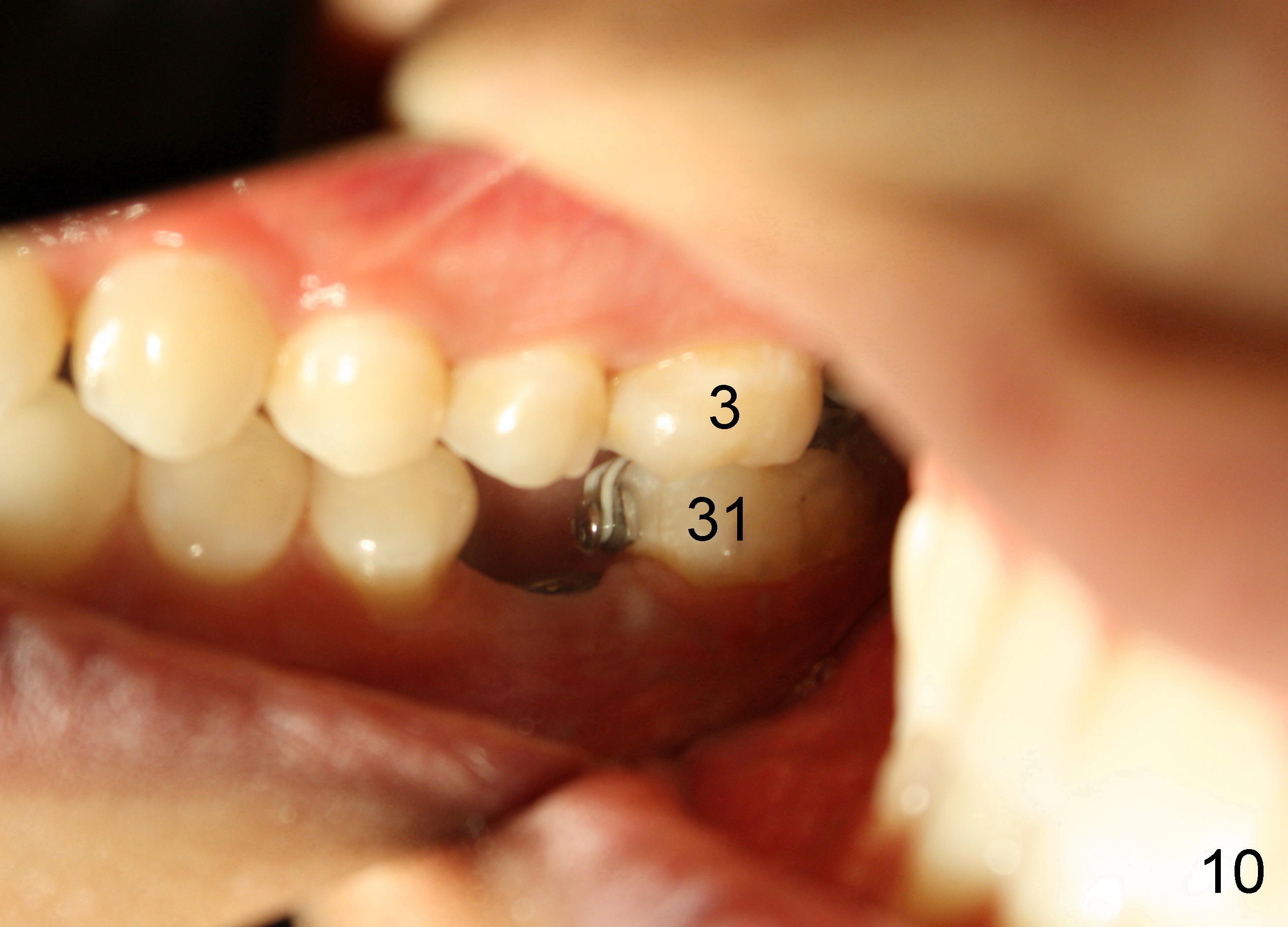
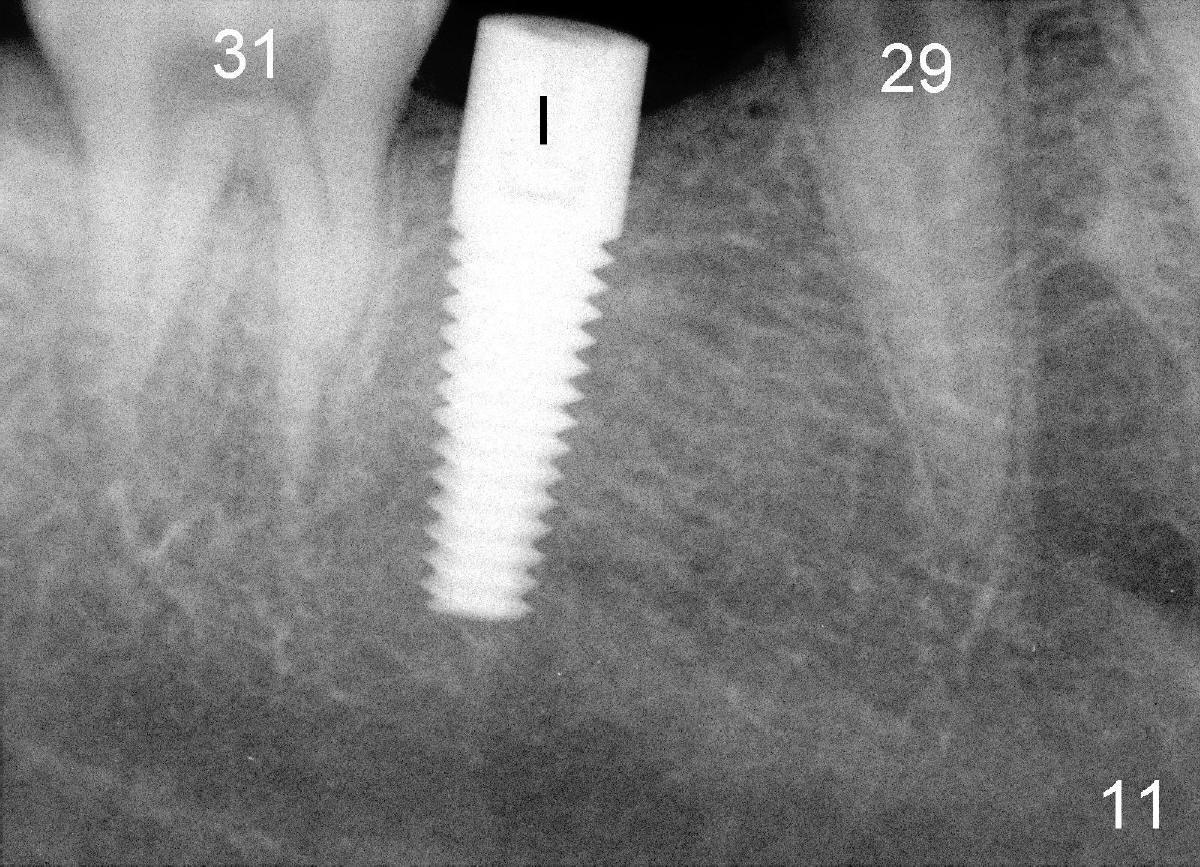
The tooth #31 is uprighted in six months (Fig.8, as compared to Fig.5). The edentulous space increases from 6 mm to 9 mm mesiodistally, which is still not enough. The M-D width of #19 is 12 mm. In fact, the tooth #2 has been intruded substantially (Fig.9. Compare to Fig.3). The possible reason for resistance of distal movement of #31 is an interference from the tooth #3 (Fig.10). A regular implant is placed intentionally in the distal aspect of the edentulous area (Fig.11: I). The next plan is to place temporary crown on the implant once it osteointegrates to raise the occlusion efficiently so that the tooth #31 is free to move distally with retraction of power chain attached to the mini-implant (as shown in Fig.2). The regular implant may be also used as anchorage to push #31 distally. See you later.
Xin Wei, DDS, PhD, MS 1st edition 11/19/2011, last revision 04/30/2017