



|
|
|
|
|
|
|
|
|
|
Drawback of Composite Prior to RCT
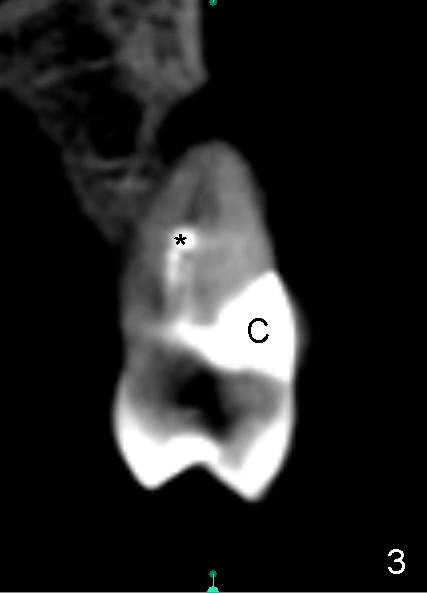
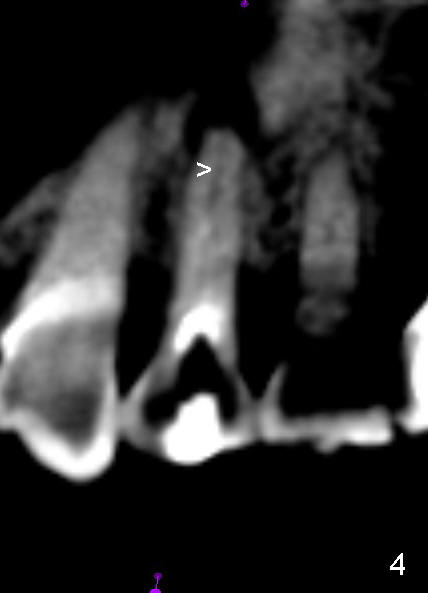
A 72-year-old lady has a deep cervical defect of the tooth #12 (Fig.1 ^) associated with buccal apical fistula (*) and periapical radiolucency (Fig.2 *). To prevent bleach leakage during root canal therapy (RCT), composite is used to repair the defect (Fig.3 (CT coronal section) C) prior to access. The buccal canal is not located probably due its own or iatrogenic (due to composite) obliteration. After thorough debridement of the lingual canal, Calcium Hydroxide paste is placed (*).
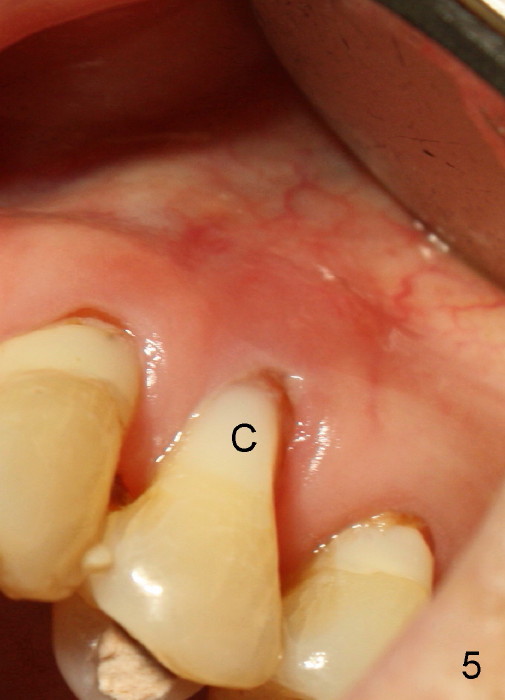
A month later, the fistula disappears (Fig.5). Effort is exerted without success to find the obliterated canal, including increasing access and removing the portion of composite which may block the opening of the canal. RCT is finished. Two months postop, the patient returns for prophy. She remains asymptomatic. There is no recurrent infection. Seven months post RCT, periapical radiolucency seems to have disappeared (Fig.6), whereas the fistula does not recur (Fig.7).
Anyway, to get the best chance of success of RCT, definitive restoration should be delayed.
Return to Professionals
Xin Wei, DDS, PhD, MS 1st edition 11/23/2014, last revision 04/13/2015