

|
|
|
|
|
|
|
|
|
|
|
|
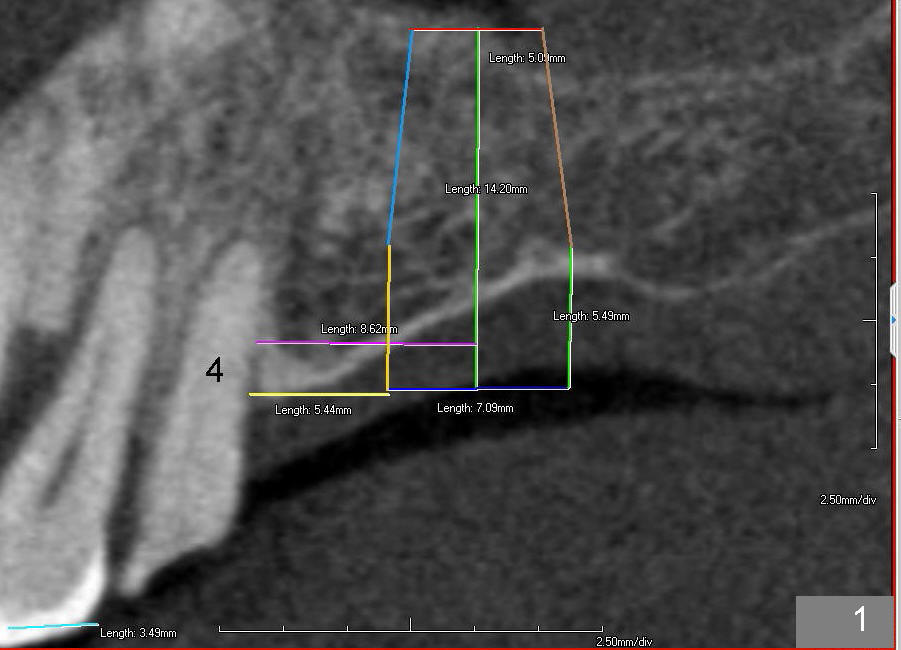
Bone Expanders for Sinus Lift
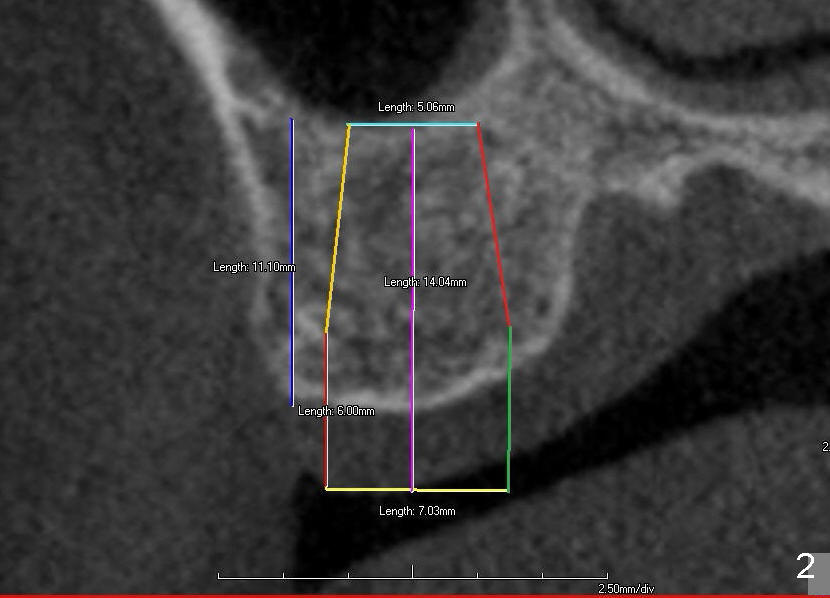
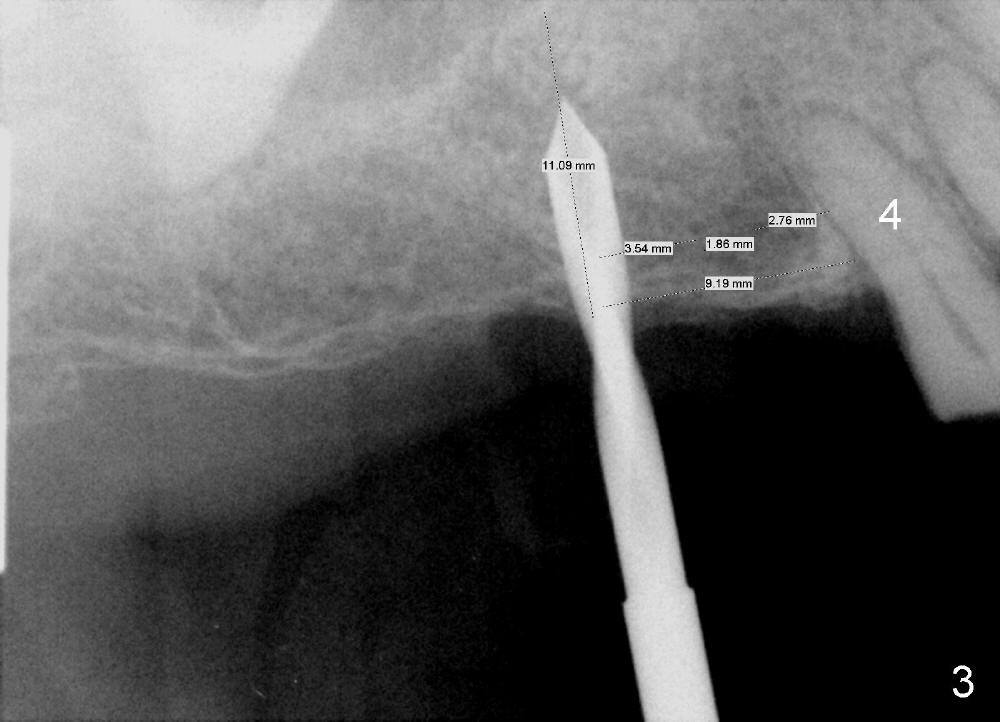
Model surgery indicates that the implant at the site of #3 should be placed 3-4 mm (half the width of a premolar) more distal (Fig.1: CBCT sagittal section). A 7x14 mm tapered soft tissue-level implant appears to be appropriate to the recipient alveolus (Fig.2 coronal section). PA is taken when a 2.0 mm pilot drill makes an initial osteotomy at the depth of 8 mm (Fig.3); the distance between the distal surface of #4 and the center of the osteotomy is equivalent to that of the design (Fig.1). The final depth of the osteotomy is then adjusted at 11 mm.
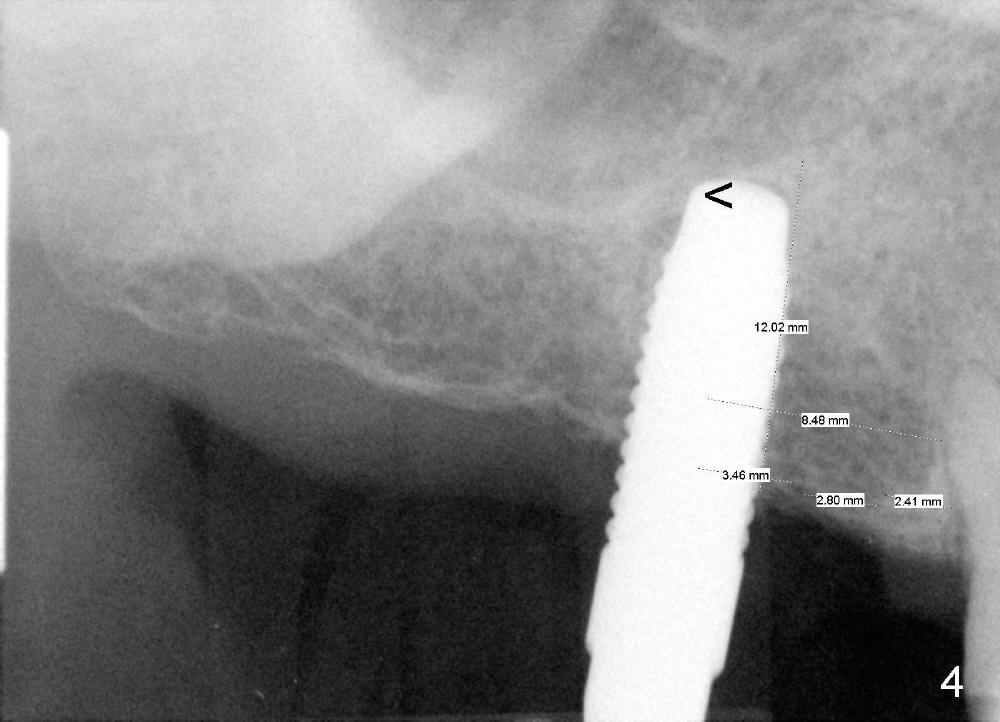
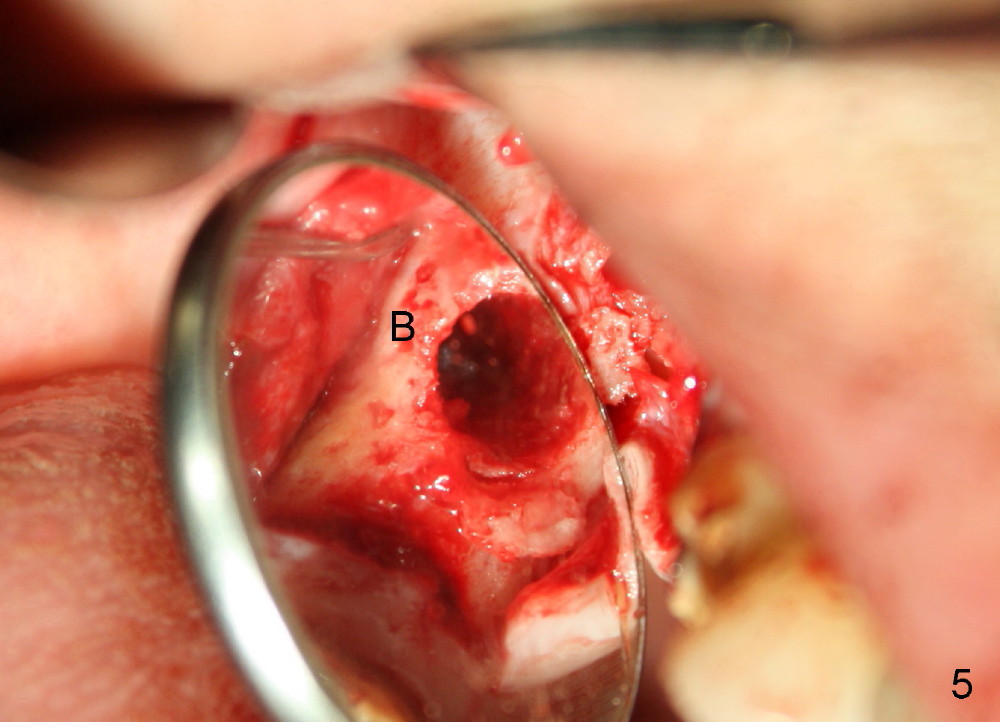
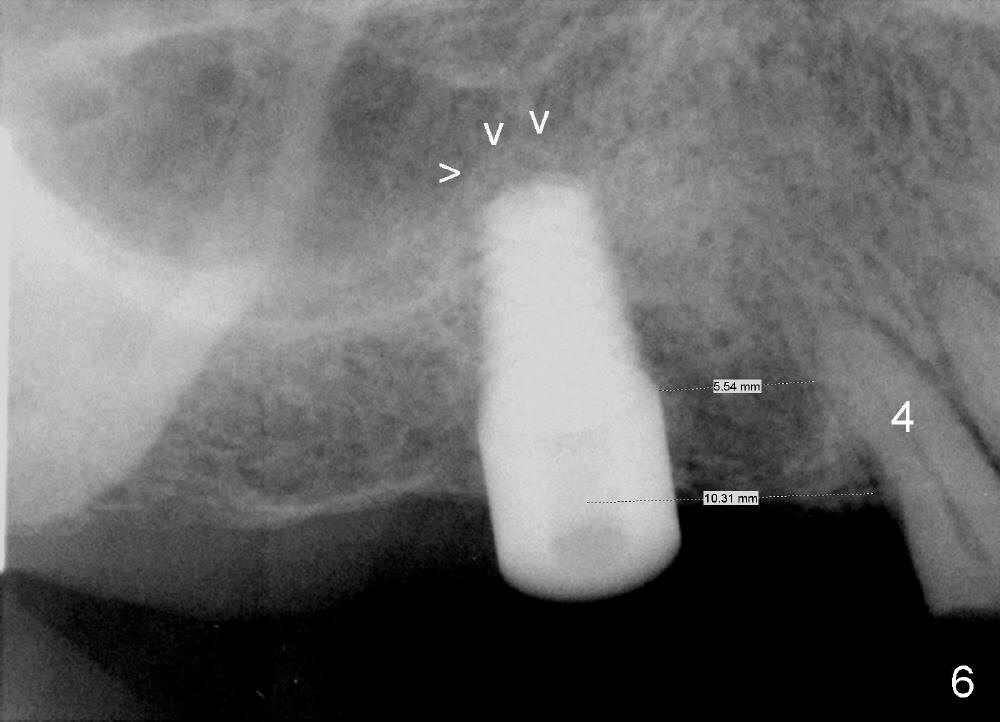
The pilot drill is easily penetrating the cancellous bone, suggesting low bone density. The remaining osteotomy is finished by bone expanders (Fig.4: 4.3 mm) and taps until 6x14 mm at gingival level. There is no sinus perforation when the 6x14 mm tap is removed from the osteotomy (Fig.5). Sinus lift is observed (Fig.6 arrowheads) when a 6x14 mm implant is placed with insertion toruqe > 60 Ncm. The distance to the adjacent tooth remains consistent to that of design.
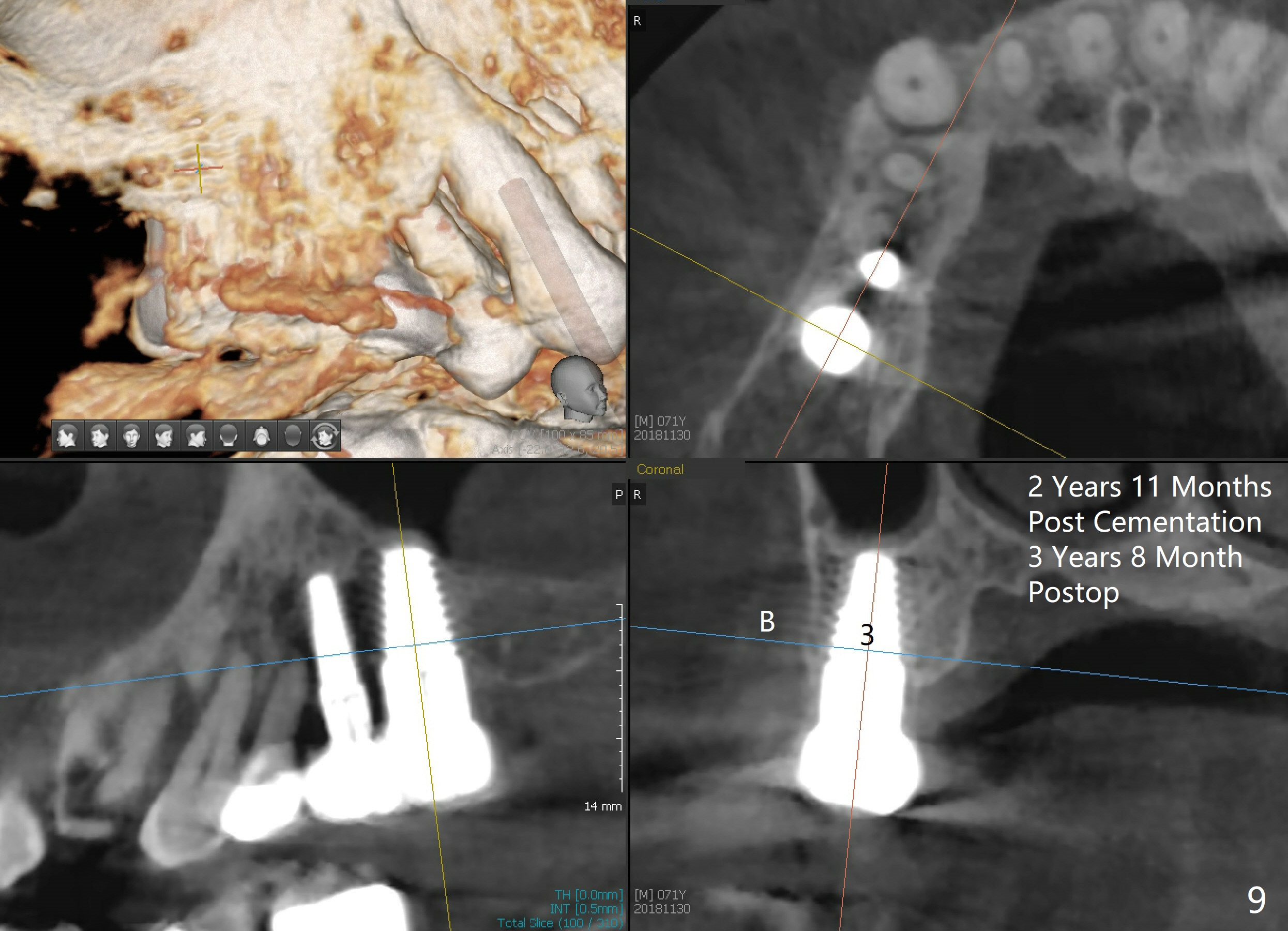
The flaps do not completely contact the implant when they are sutured. The wound needs protection during the initial postop stage. One of modes is to use perio dressing. The latter is not retentive in the distal edentulous area. Addition of a short abutment (Fig.7 A) over the implant should increase the retention of perio dressing (Fig.8) while micromovement of the implant is minimal. The tooth #30 is missing. There is no bone resorption 2 years 11 months post cementation (Fig.9).
Xin Wei, DDS, PhD, MS 1st edition 03/17/2014, last revision 12/16/2018