|
|
|
|
|
|
|
|
|
|
|
|
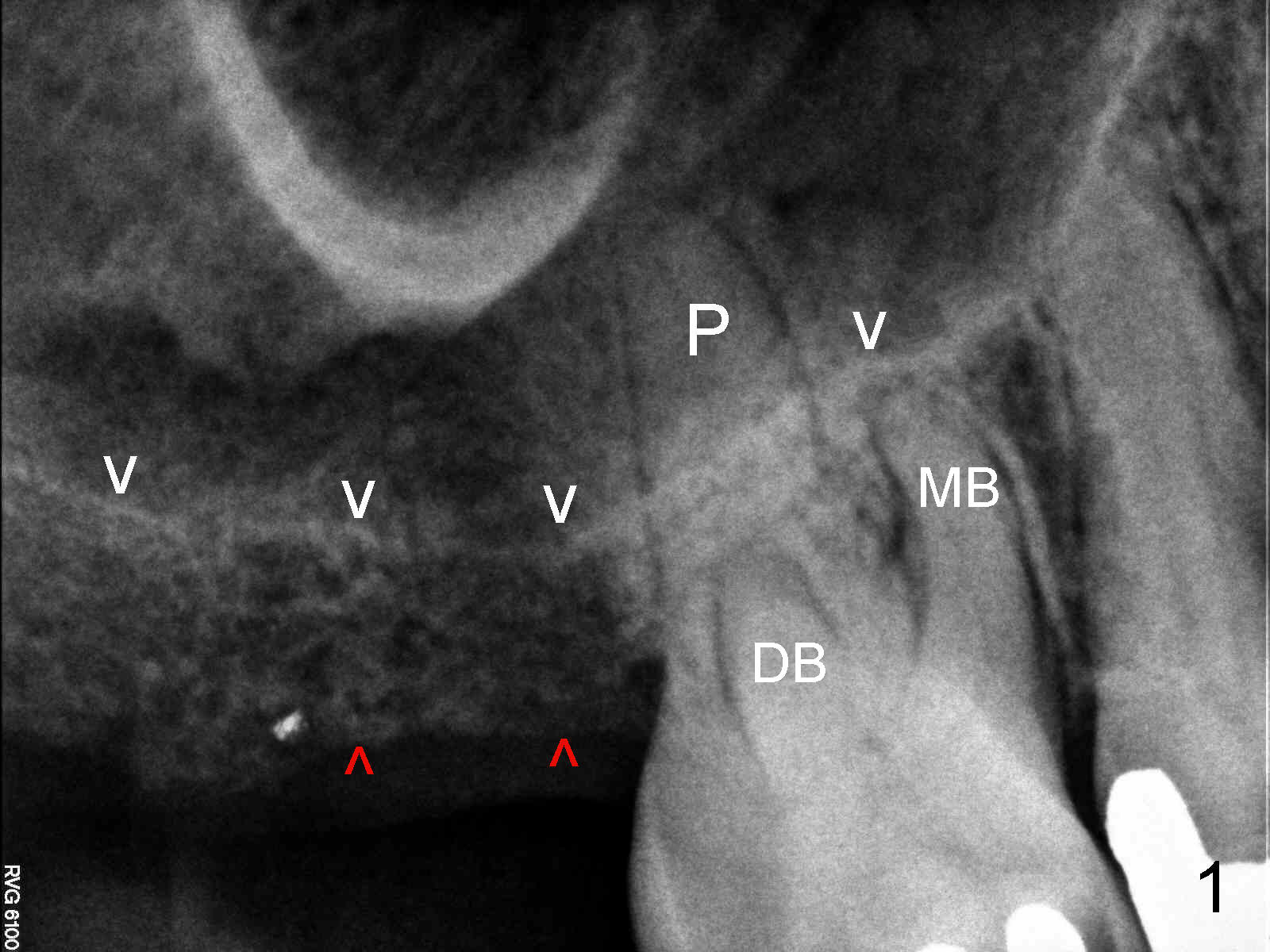
Crestal Sinus Lift
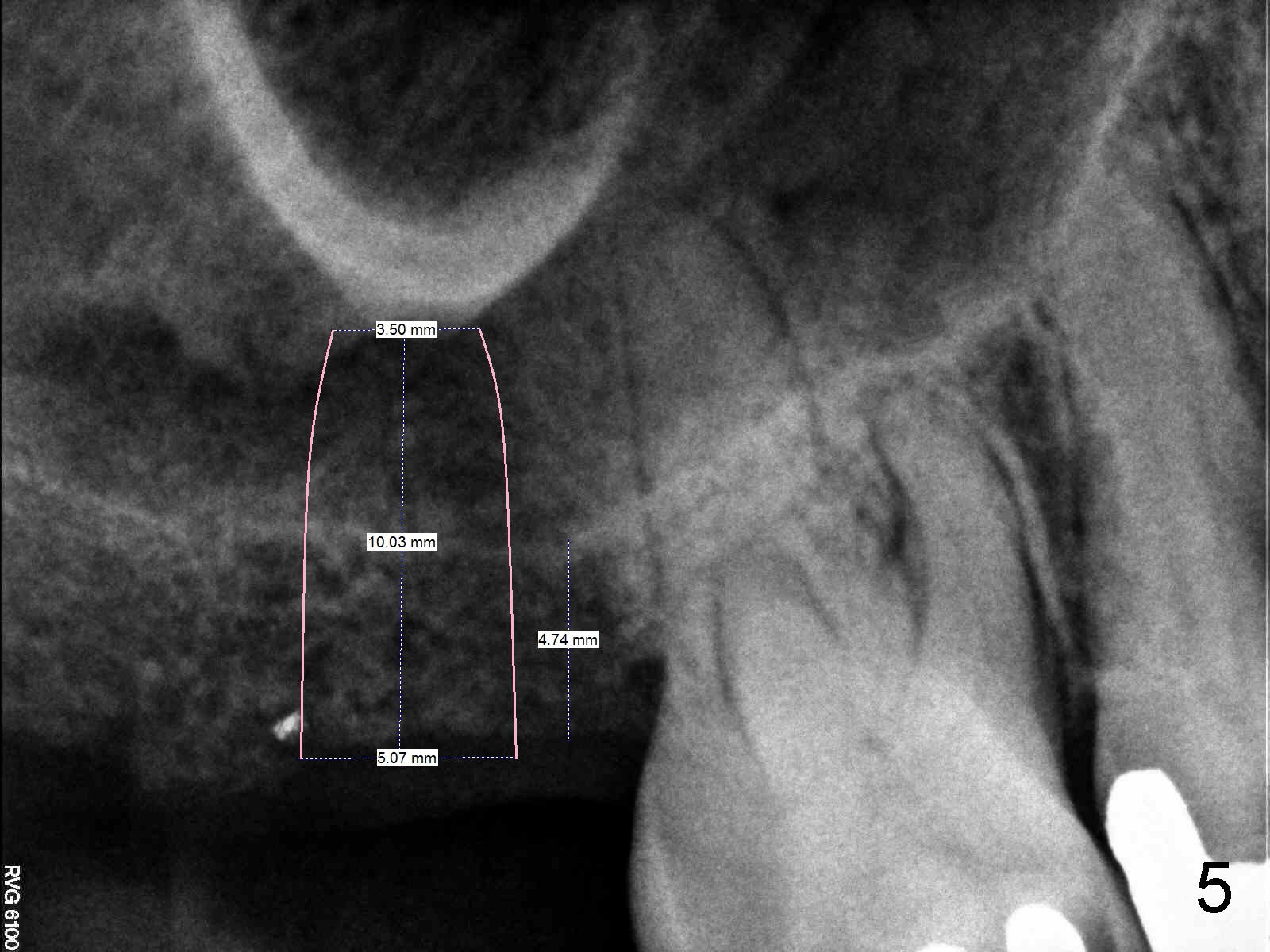
A 60-year-old man requests restoration of the missing upper right 2nd molar (Fig.1). It appears that the bone height is limited (between white and red arrowheads, approximately 5 mm (Fig.5)). Study of the sinus floor in association with the roots of the 1st molar reveals that the palatal root (P) appears inside the sinus. In fact it is not. Therefore there is bone apparently inside the sinus.
For the same reason, the root of the 2nd molar must have been above the sinus floor (Fig.2 arrowheads). CBCT may confirm the fact.
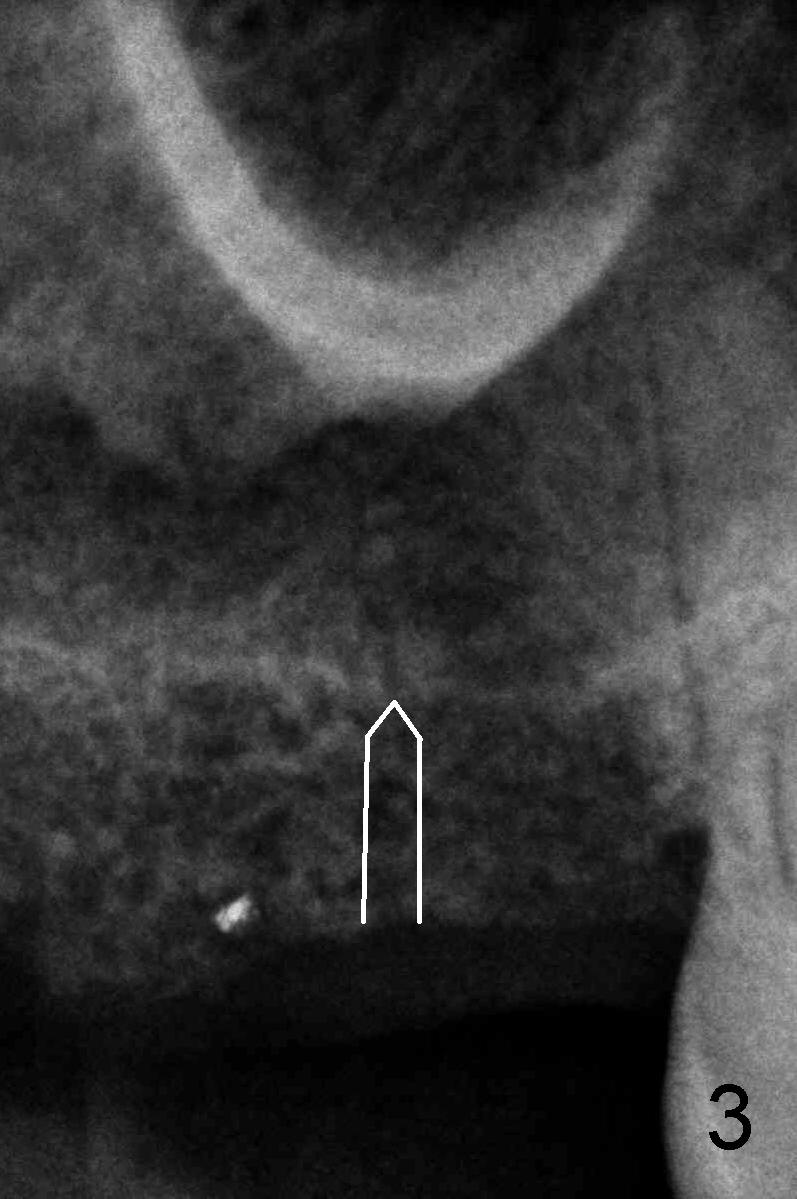
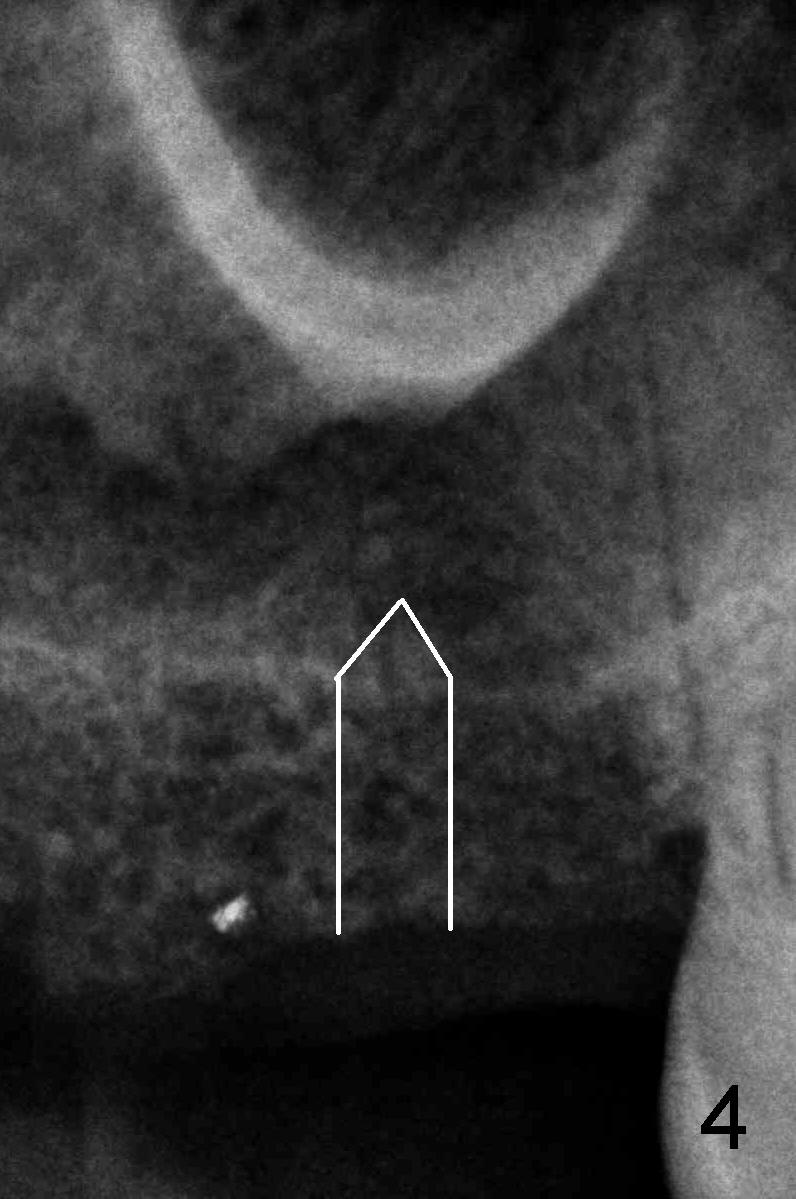
Anyway, a 1.6 mm pilot drill or 2 mm osteotome may be used to initiate osteotomy at the depth of 4-5 mm (Fig.3). An explorer is used to check whether the sinus membrane has been reached or not. As the diameter of bone expanders or osteotomes increases, the depth of the osteotomy increases (Fig.4), pushing the native bone into the sinus. Each step check sinus membrane integrity by using an explorer or doing nose blowing test. The implant can also push more bone upward when it is being placed (Fig.5). Combined lateral and crestal sinus lift is not recommended in this case because of limited access.
Prepare collagen membrane in case of sinus membrane perforation and allograft, xenograft or synthetic bone for additional lifting. How many bone expander kits do you have?
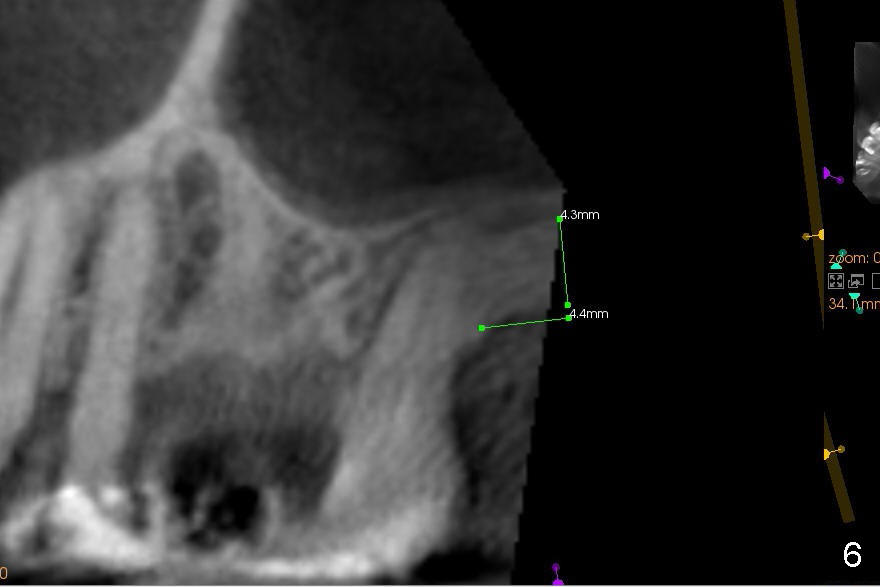
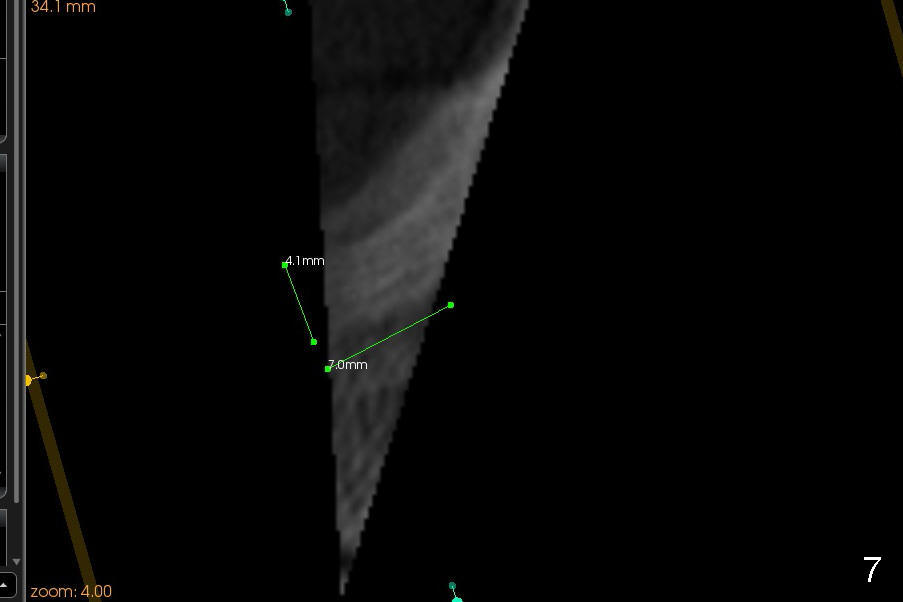
CBCT confirms the bone height (4.4 mm) (Fig.6). Bone density is 200-400 Hounsfield units. The best new is sufficient bone width (7 mm) buccolingually.
The reduction in the bone height in this case is probably due to failure of implantation. The latter is in turn due to poor bone density in the posterior maxilla. To avoid this, osteotomy should be under prepared. See below
Robert: How are you lately? I have done several DIO implants recently and found that the insertion torque is not so high. Probably the implant threads are not so aggressive and drills are relatively too big to corresponding implants. My experience tells me that in the future, I would use the final drill one size smaller than the implant for the mandible, two sizes smaller for the maxilla.
Today (04/08/2014) an immediate implant patient returns 2.5 months post implantation. To place 5.3x12 mm implant, a 2 mm pilot drill is used, followed by osteotomes and bone. expanders. Xin
Actually I prefer your summary. Last week I had to use one size bigger drill for D1 bone (Tatum implant). On safe side, it is better to use 1 or 2 sizes smaller drill, particularly for the upper jaw. If the torque is too high, remove the implant and use 1 size bigger drill. Do you have good feel of bone density? I am learning how to feel when 2 mm pilot drill is penetrating the cortex and cancellous bone now.
Xin Wei, DDS, PhD, MS 1st edition 02/24/2014, last revision 04/09/2014