|
|
|
|
|
|
|
|
Immediate Implants in Upper Anteriors
Robert: Thank for the info. The patient may be a bruxer. The implant at the site of #7 is probably too large for the bone. The buccal plate is most likely perforated. Do you have 3x20 or 23 angled one piece implant? If not, I will bring them. Immediate provisional for # 6 and 7 should be splinted. #7 may need cortical plate graft from the chin or ramus. This is the most interesting case. You must have crown forms in office.
In case bone resorption is too severe at the site of #7, place one large implant at the site of #6 and cantilever #7.
Do you have serrated bone curettes? It is useful to remove granulation tissue from the implant site. I am going to bring several of them in different sizes, $40 each (originally $50). They are still in plastic bags. Do I need to wrap them separately and autoclave now so that we do not have to hurry on Monday?
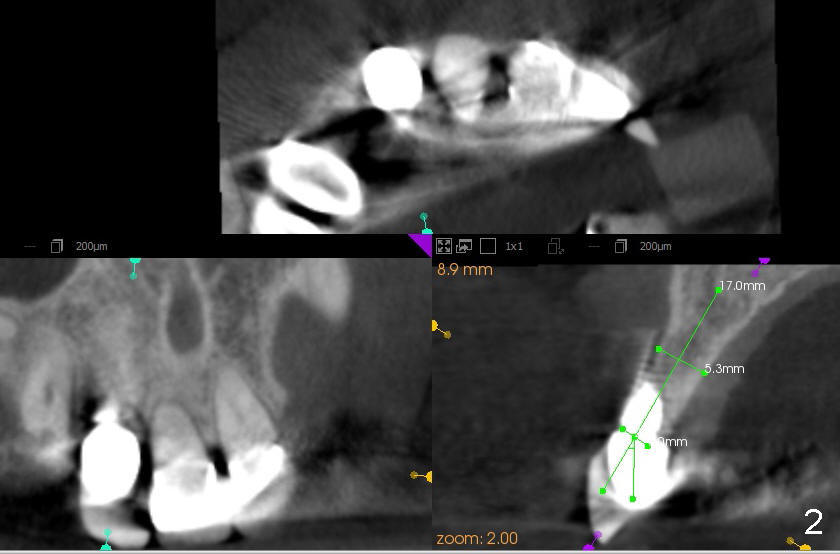
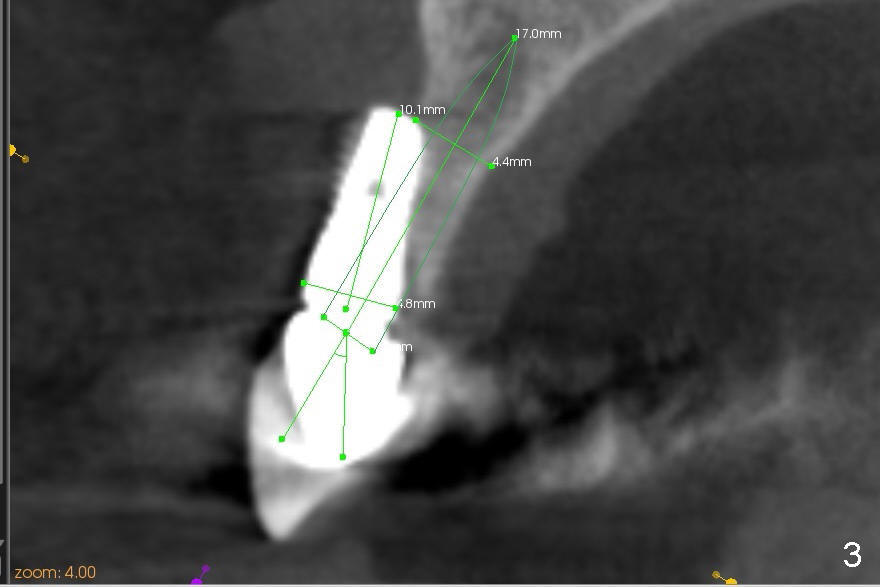
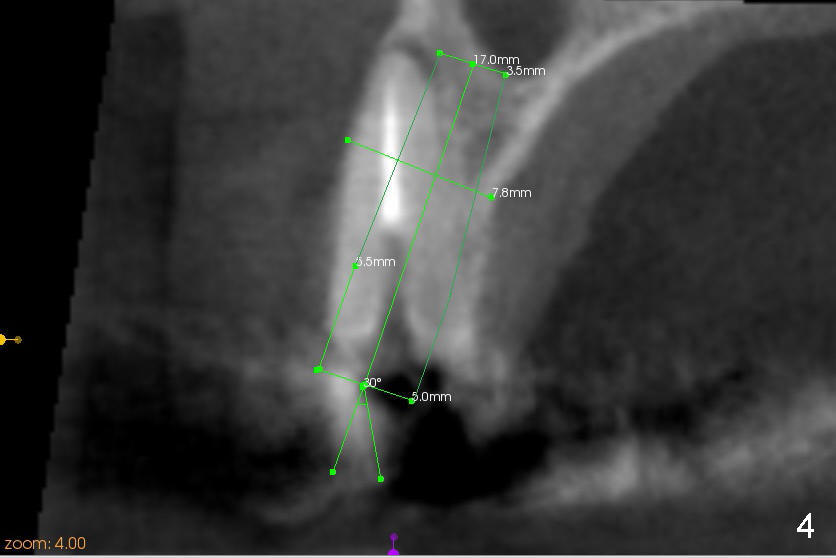
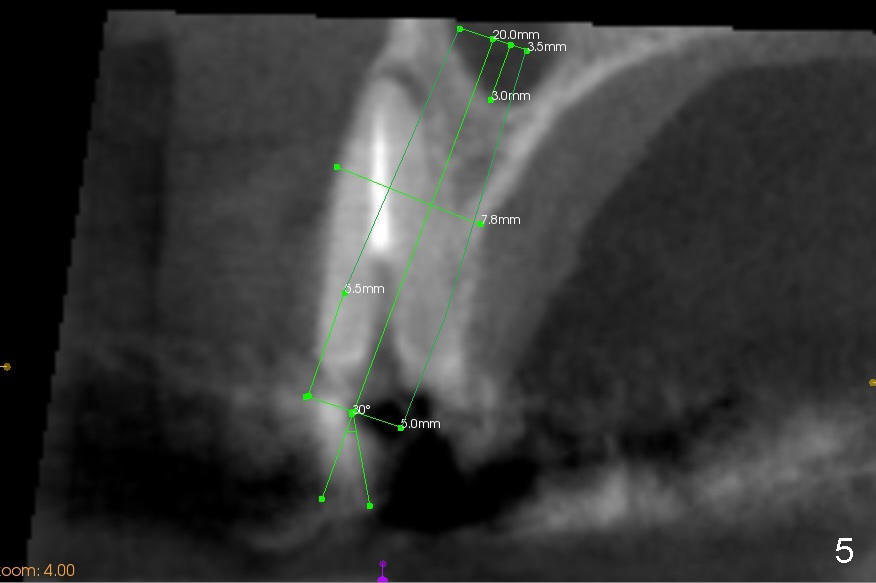
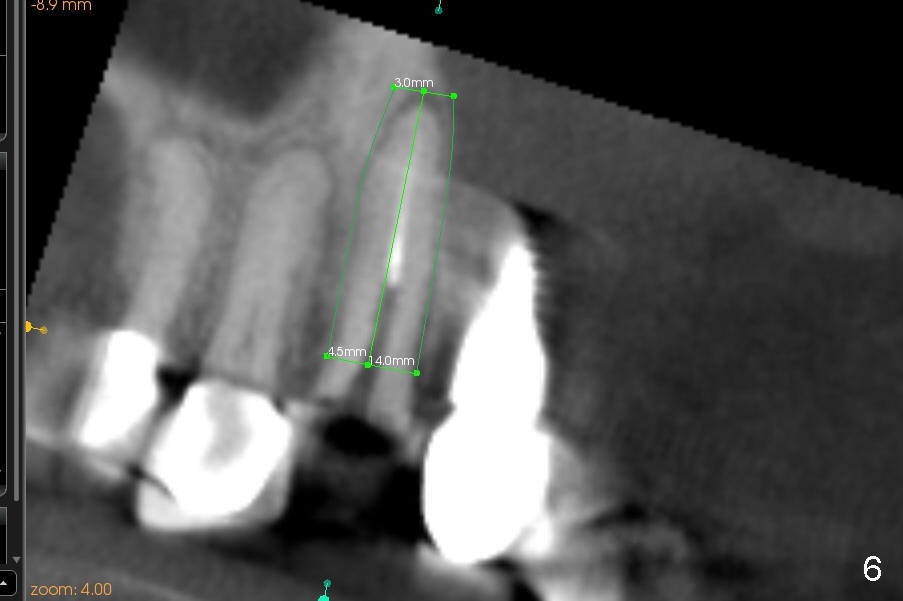
CBCT studies reveal that the implant perforates the buccal plate at the site of #7 and that there is still enough bone to support 3.0x17 mm one piece implant (Fig.2,3). There is limited bone apical to the tooth #6. The implant should be at least 17 mm for bone level and 14 mm for tissue level (Fig.4) or preferably 20 mm with sinus lift (Fig.5). The diameter will be 4.5 mm (Fig.6) or 5 mm (Fig.4.5).
For cosmetics, the tooth #6 and the implant #7 should be removed without flap. Two immediate provisionals are to be fabricated separately and bonded with composite after cementation.
Return to One and Two Piece Implants
Xin Wei, DDS, PhD, MS 1st edition 02/27/2013, last revision 03/02/2014