
.jpg)





|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|||||
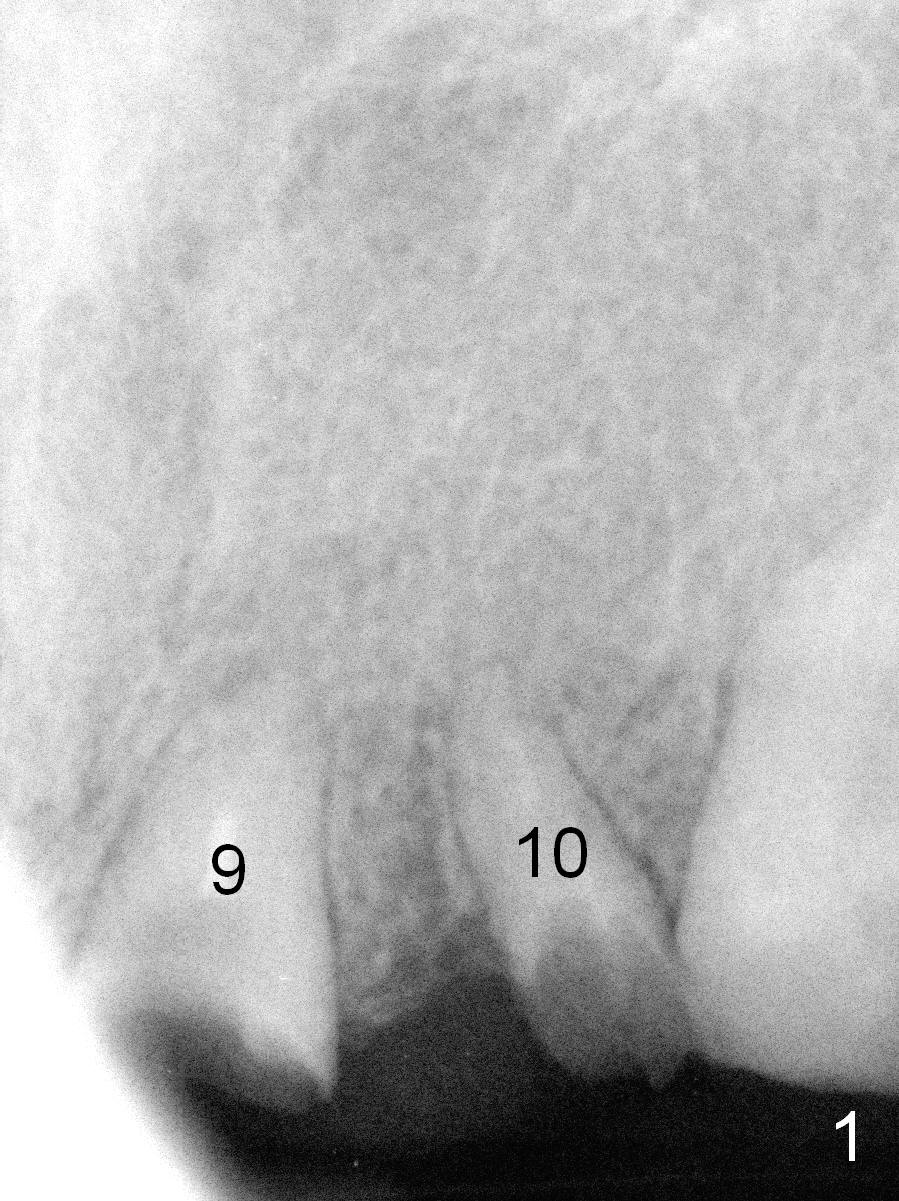
Depth and Position of Implant Placement for 2 Adjoining Incisors
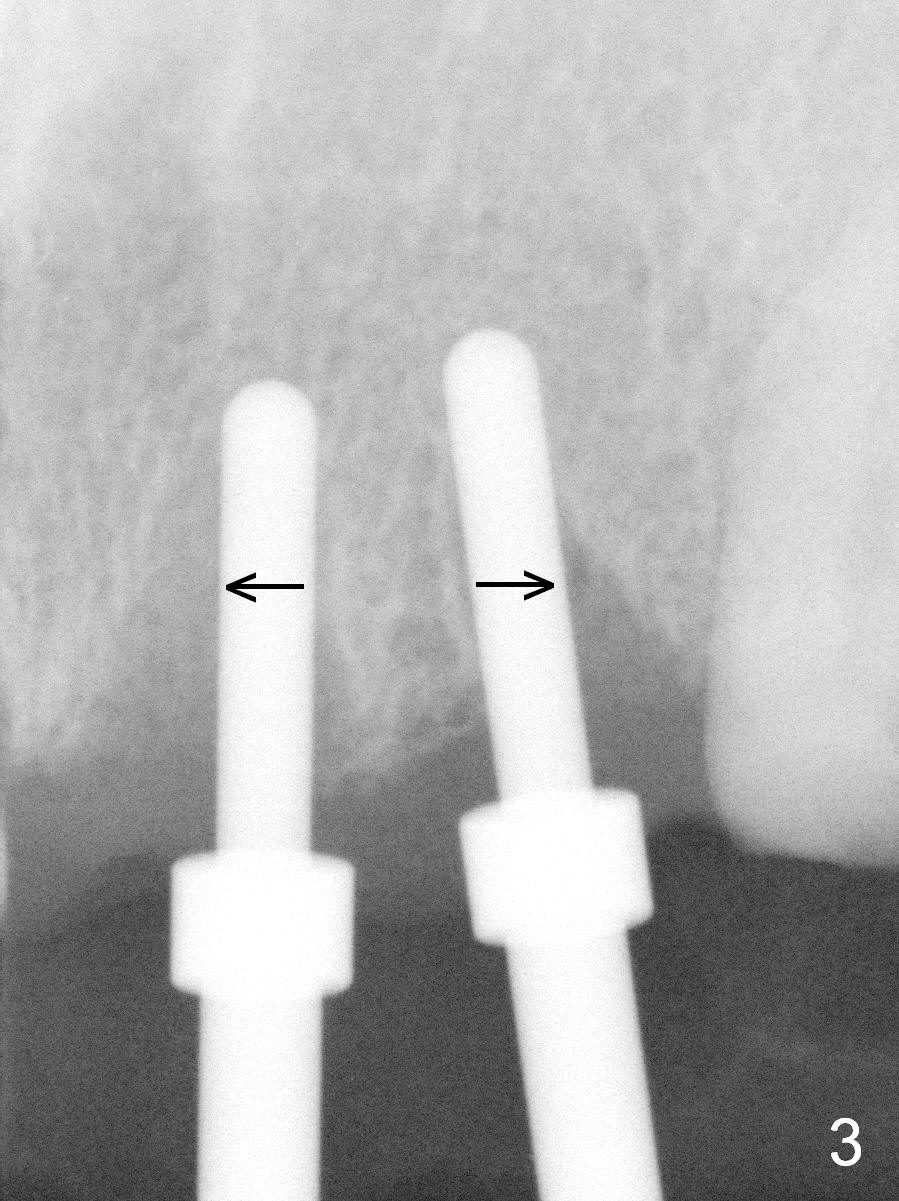
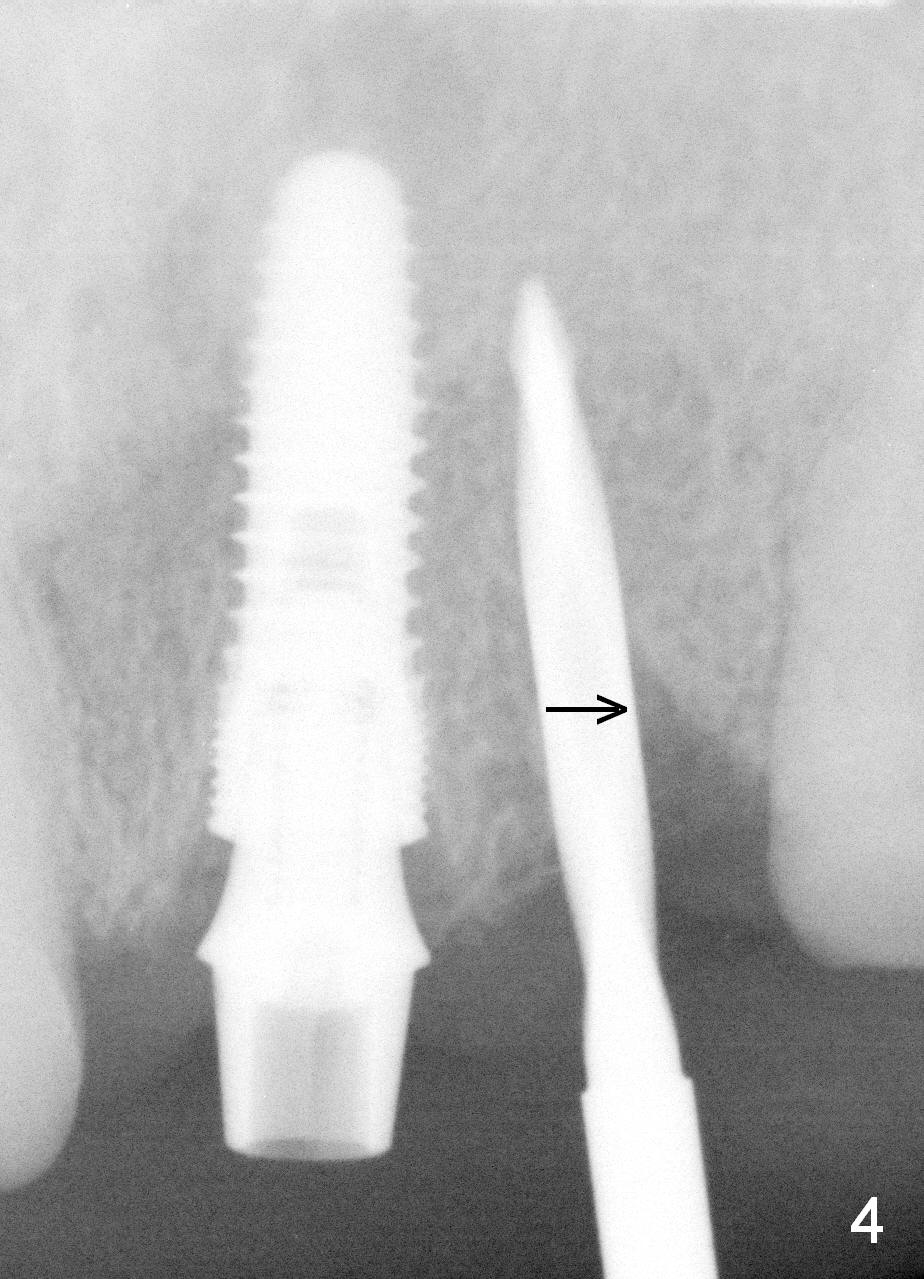
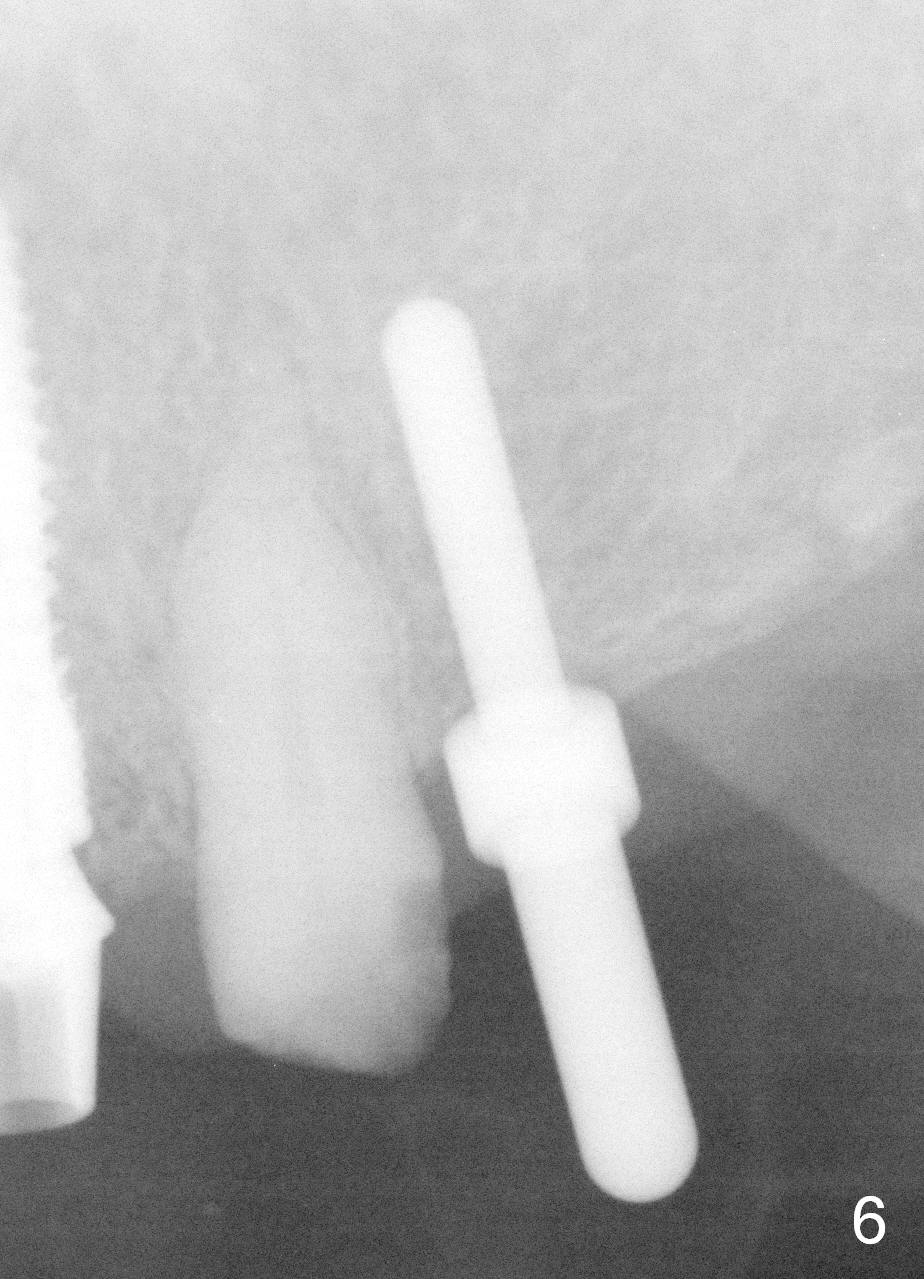
Due to limited vertical dimension of occlusion, bone-level implants should be placed a little deeper than usual. Fig.1,2 are preop PAs. After extraction of the 2 incisors, two parallel pins are inserted with the aid of a surgical stent, but radiologically, the position of the osteotomies needs to be adjusted (Fig.3 arrows). With the parallel pin/pilot drill at the site of #10, a 4.5x14 mm implant is placed at the site of #9 with placement of a 4.8x4(2) mm abutment (with barely enough occlusal clearance clinically) (Fig.4). With further adjustment of the position of the osteotomy at #10 (Fig.4 arrow), a 4.1x14 mm implant is placed with the same size of the abutment and the same amount of occlusal clearance mentioned above (Fig.5). The position of the initial osteotomy is also doubly checked (Fig.6) prior to placement of the delayed implant at #12 (Fig.7). The abutment is 4.8x4(1) mm (1 stands for the height of the cuff of the abutment). An immediate provisional bridge is fabricated at #8-12 using a restorative stent with adjustment of occlusion.
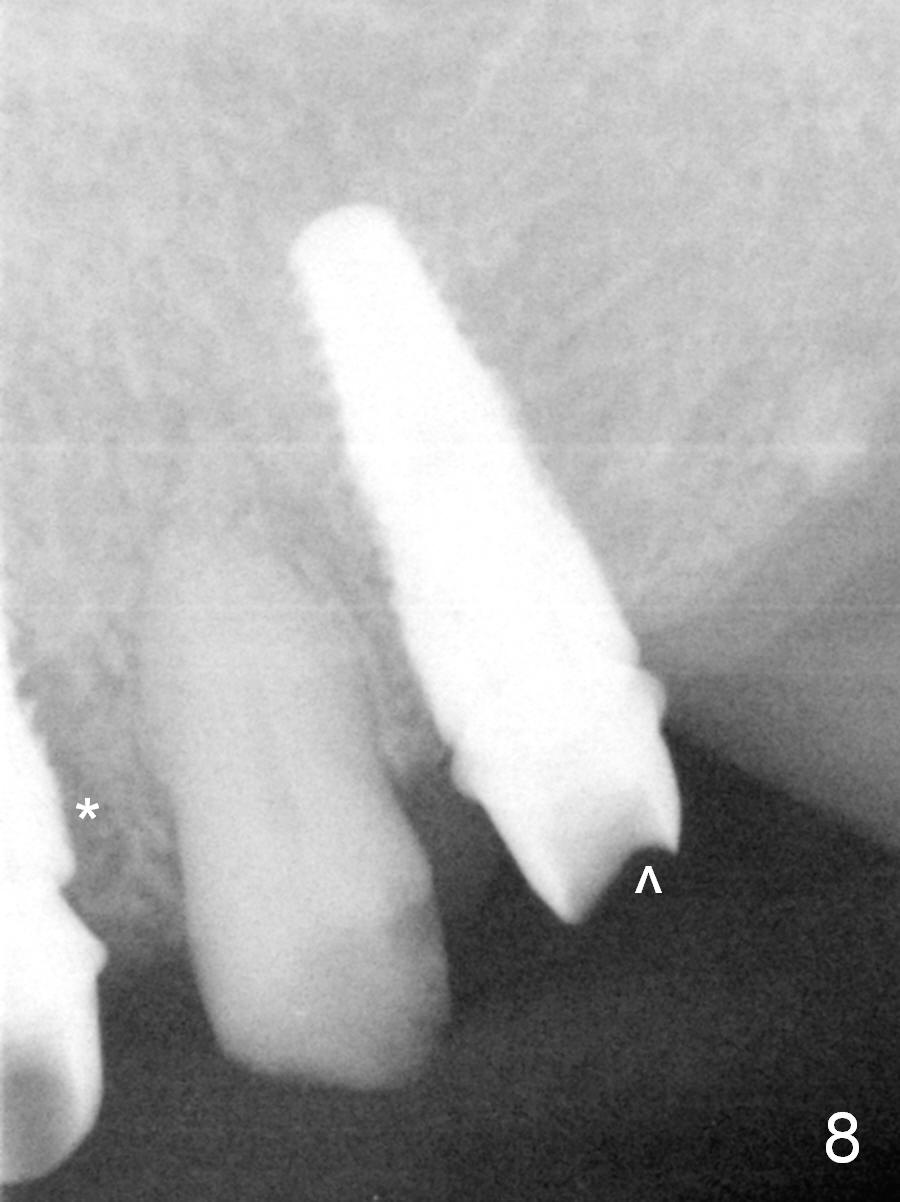
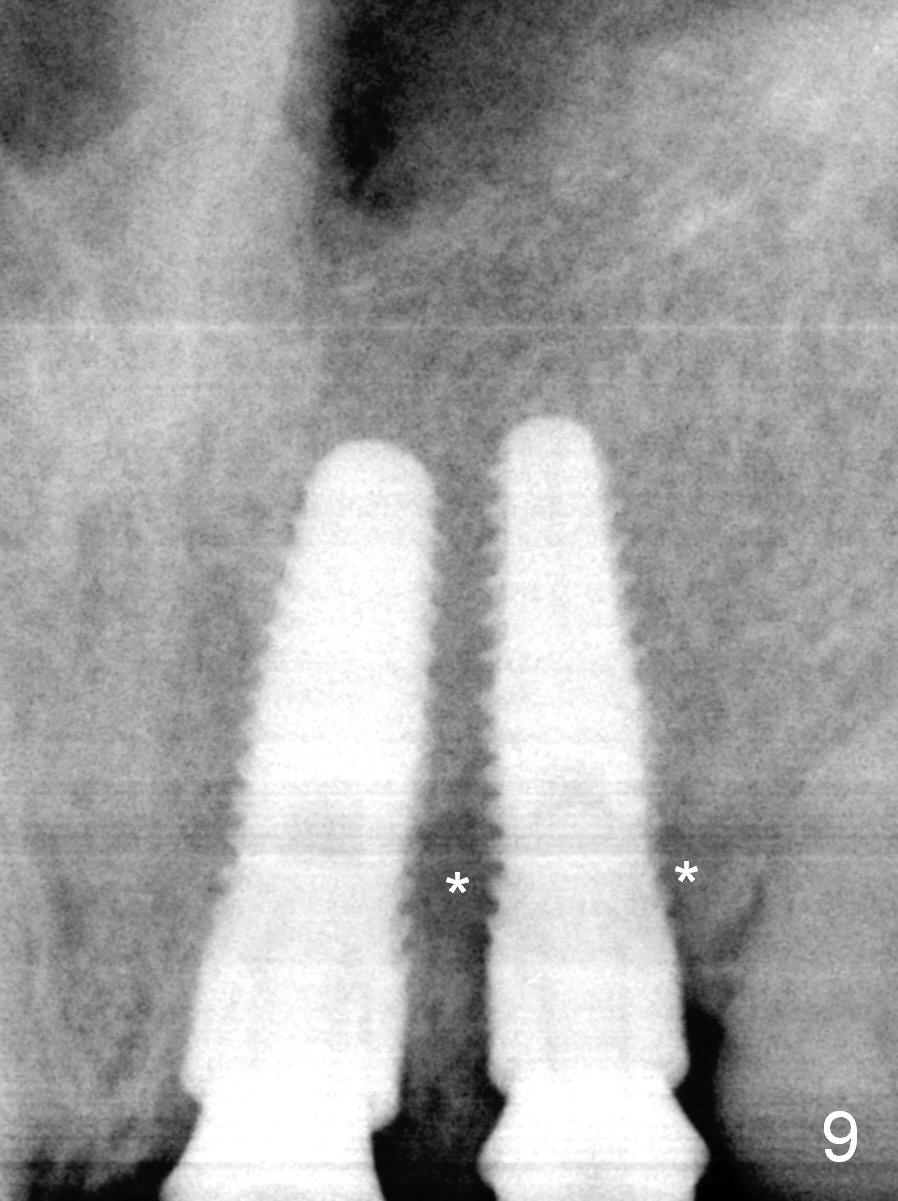
The provisional acrylic bridge cracks and dislodges postop. It is repaired several times. One month 12 days postop, bone apparently heals normally around the implants (Fig.8,9). The provisional is removed for final impression so that the provisional will not be dislodged so easily. When the abutment at #9 is being torqued at 35 Ncm, it turns slightly. In contrast, the abutment at #10 spins while being torqued. When un-torqued, the implant is removed together. A larger implant (4.5x14 mm) is immediately placed with insertion torque at 35/40 Ncm (Fig.12). The same abutment returns to the site with hand tightening. The abutment at #12 is not torqued. The final impression is taken as planned. Retrospectively, there is radiolucency around the implant at #10 (Fig.8,9 *). It appears that primary stability has reduced from 50/60 to <35 Ncm one month postop at #10. It may be alright to leave the spinning implant in place.
Two weeks later, gingiva heals with maintenance of the interdental papillae (Fig.10,11 *). The crowns at #8 and 11 are cemented permanently, while splinted crowns at #9,10 and single crown at #12 are cemented temporarily.
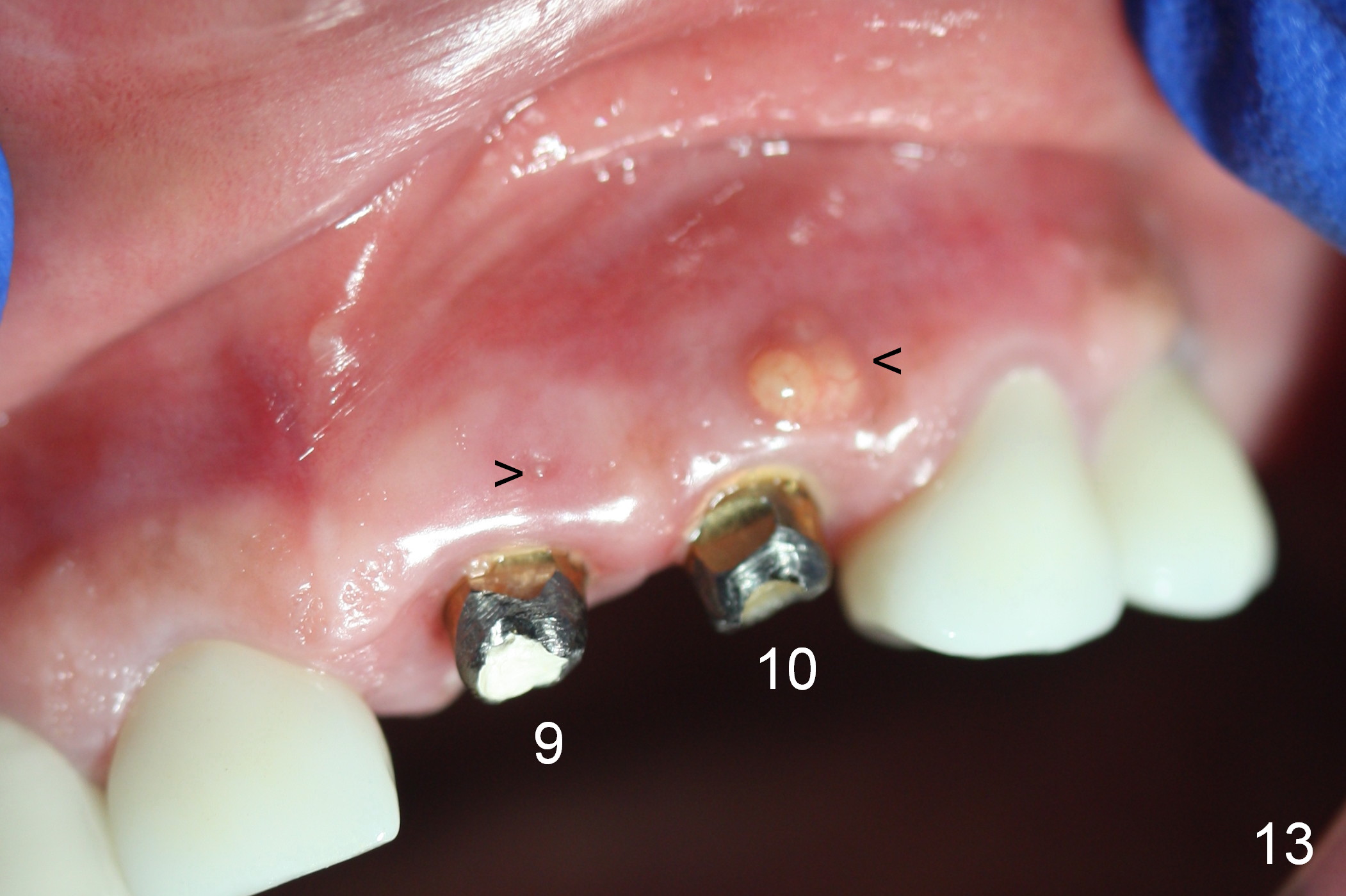
Four months later (i.e., 6 months postop), the splinted crowns dislodge. There is sign of chronic infection buccal to the implants at #9 and 10 (Fig.13 arrowheads, Fig.15 *). When the abutment at #9 is being torqued, it turns and sinks. It appears that the implant does not osteointegrate. The splinted crowns recement twice and still dislodge. A few days later, the crowns are permanently cemented.
When the patient returns, an incision (Fig.14 black line) is going to be made to expose the implants. After debridement and Metronidazole treatment, bone graft is placed if necessary. Or 1 or 2 implants are removed and replaced with longer ones (Tatum, 20 mm).
Return to Upper Incisor Immediate
Implant,
Periimplantitis
Xin Wei, DDS, PhD, MS 1st edition 04/10/2015, last revision 01/19/2018