








|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
|
|
|
|||
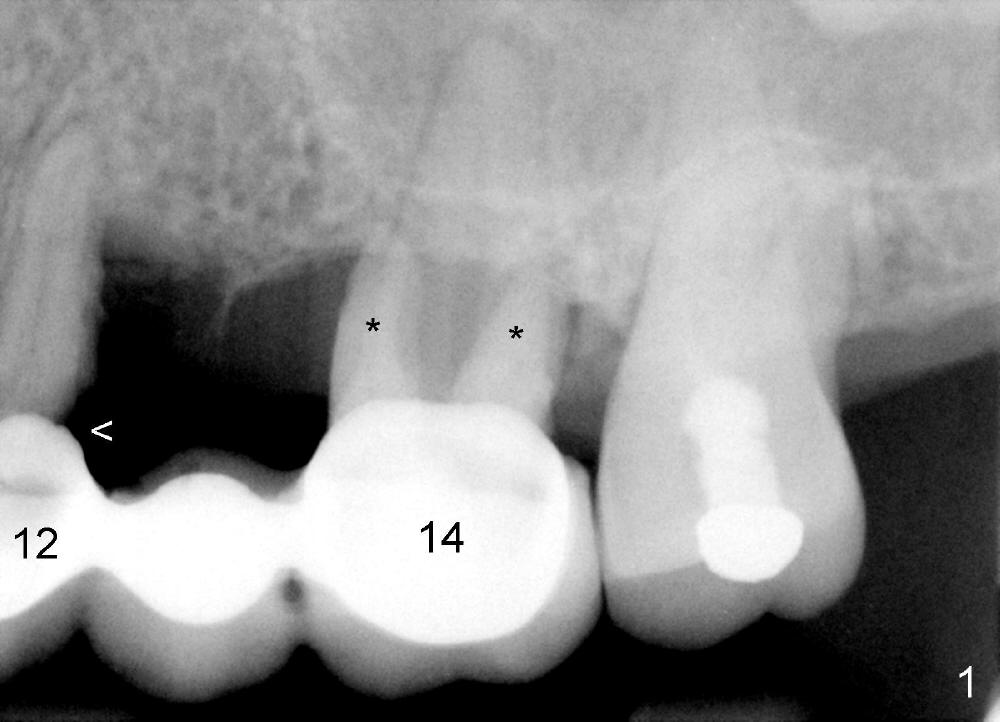
Immediate Provisional Closes Sockets
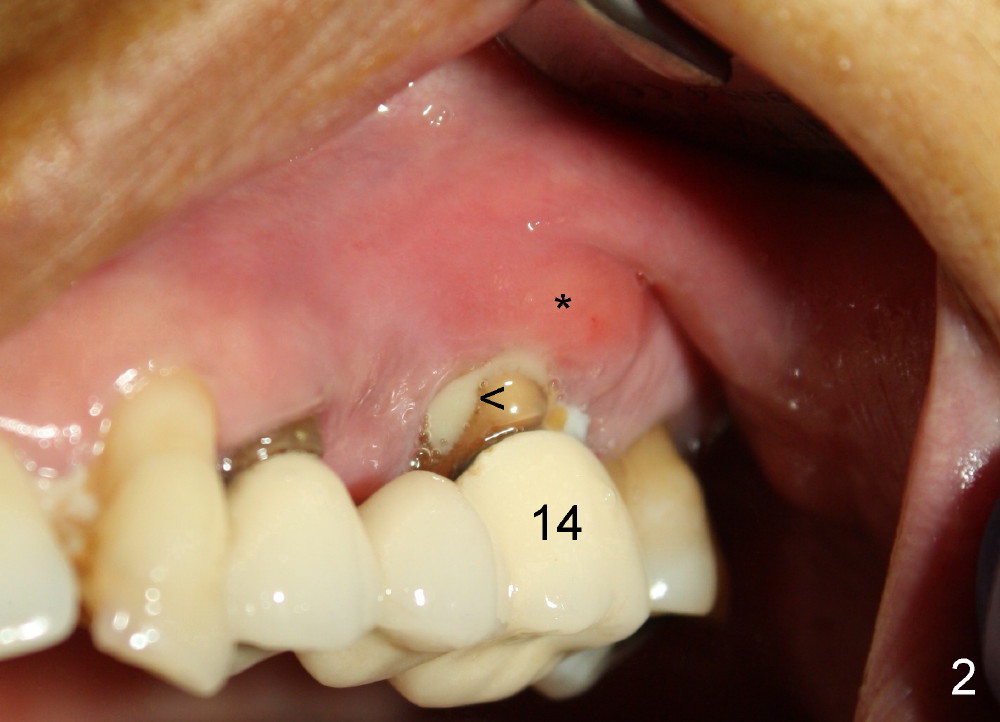
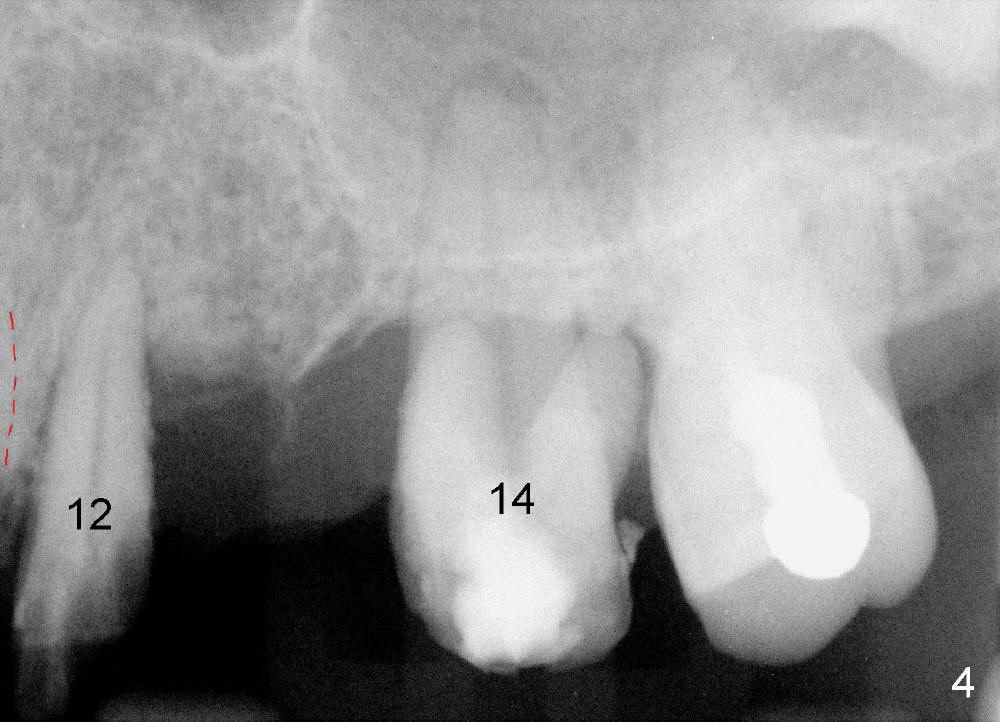
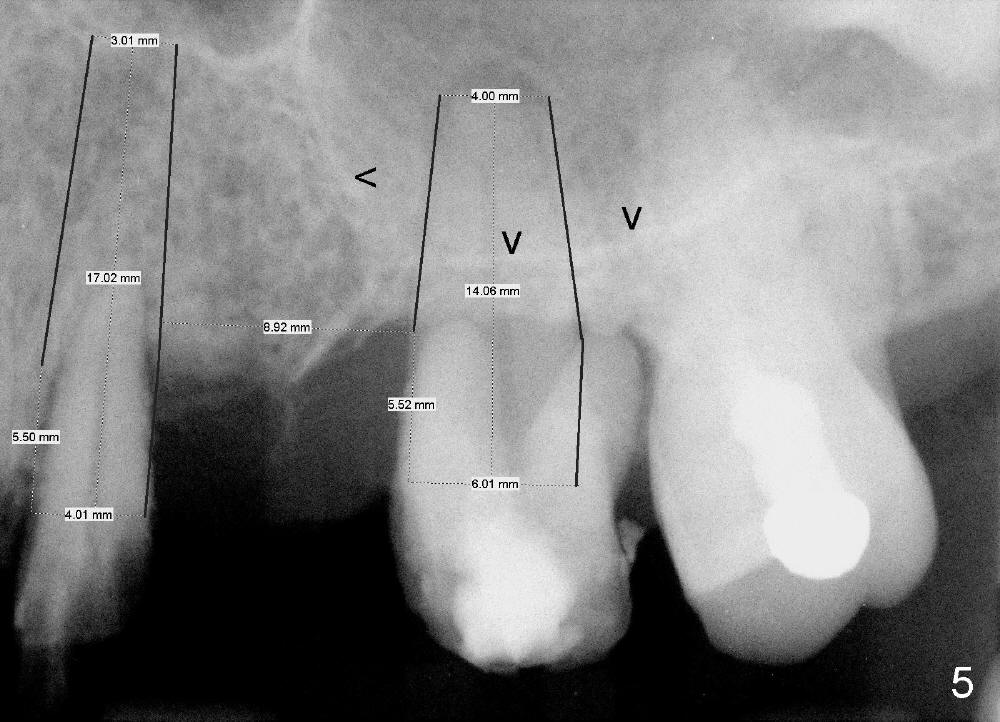
A 53-year-old lady has a failing bridge (Fig.1). There is severe bone loss around the buccal roots of #14 (*). Purulent discharge is from the gingival sulcus (Fig.2 <) with localized gingival erythema and edema (*). When the bridge is removed, the tooth #12 is found nonsalvageable (Fig.3,4). These two teeth are to be replaced by immediate implants (Fig.5). Although the sinus floor is low buccally (arrowheads), a 6x14 mm gingiva-level implant can be placed in the septum close to the palatal socket or in the palatal socket at the site of #14.
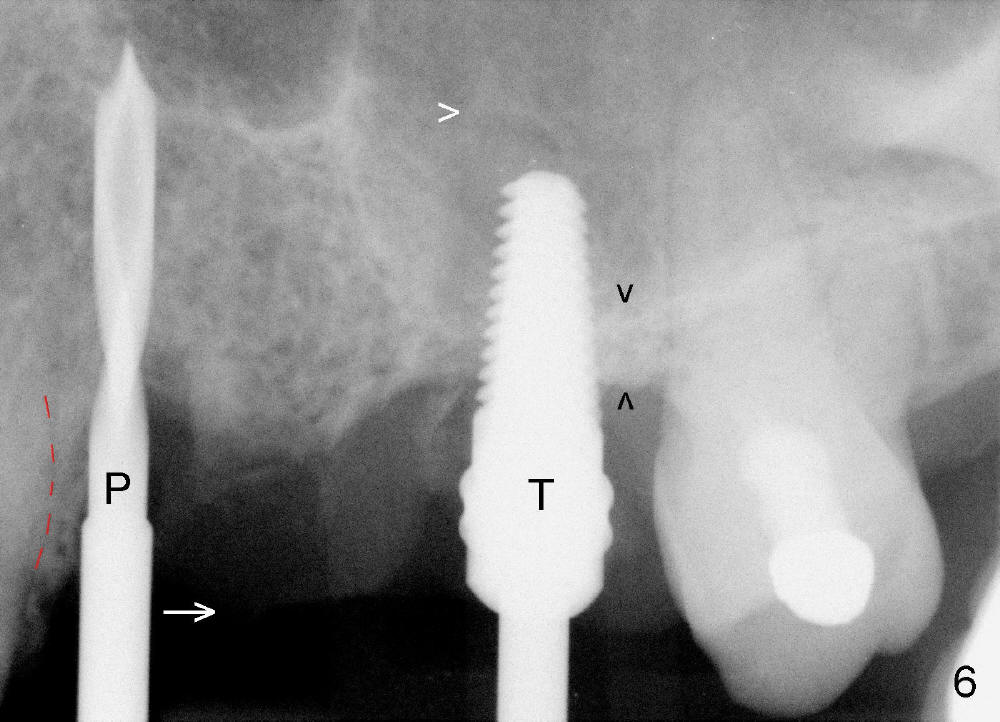
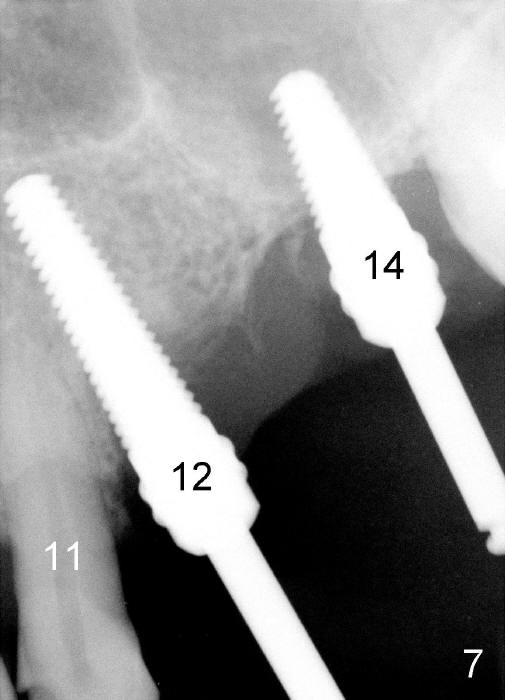
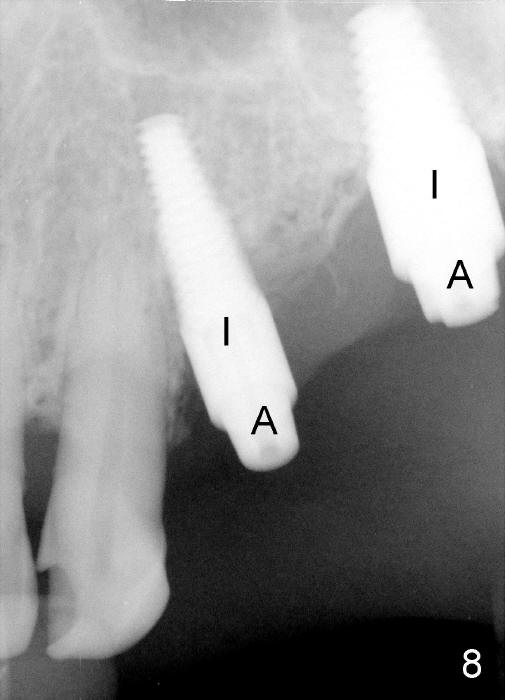
Initially the osteotomy is established with drill/reamers alternated with taps in the septum near the palatal socket. When a 4.5x14 mm tap (Fig.6 T; Fig.7: #14) is inserted, the sinus floor is perforated, but the sinus membrane is intact. When 7x14 mm tap is inserted, the sinus membrane is perforated in the buccal aspect of the osteotomy. The latter is repaired by placement of collagen dressing and then bone graft and membrane again (sandwich). The osteotomy is shifted to the palatal socket by using 5x14 and 6x14 mm taps. When the last tap is removed, the small area of the buccal aspect of the osteotomy is also found to be perforated, but the membrane is intact. When a 6x14 mm implant is placed (Fig.8), the coronal end is close to the middle of the socket (buccopalatally, due to angulation of the palatal socket).
Placement of immediate implant at the site of #12 is relatively easy. Adjustment is more or less mesiodistal. A 2 mm pilot drill (Fig.6 P) is found close to the root of the tooth #11 (red dashed line). The osteotomy is then moved distally (Fig.6 arrow). When 4.5x20 mm tap (Fig.7: #12) and 4.5x17 mm implant (Fig.8 I) are placed, there is distance from the root of the neighboring tooth. Insertion torque of the both implants is >60 Ncm. Abutments are placed (A in Fig.8) for immediate provisional.
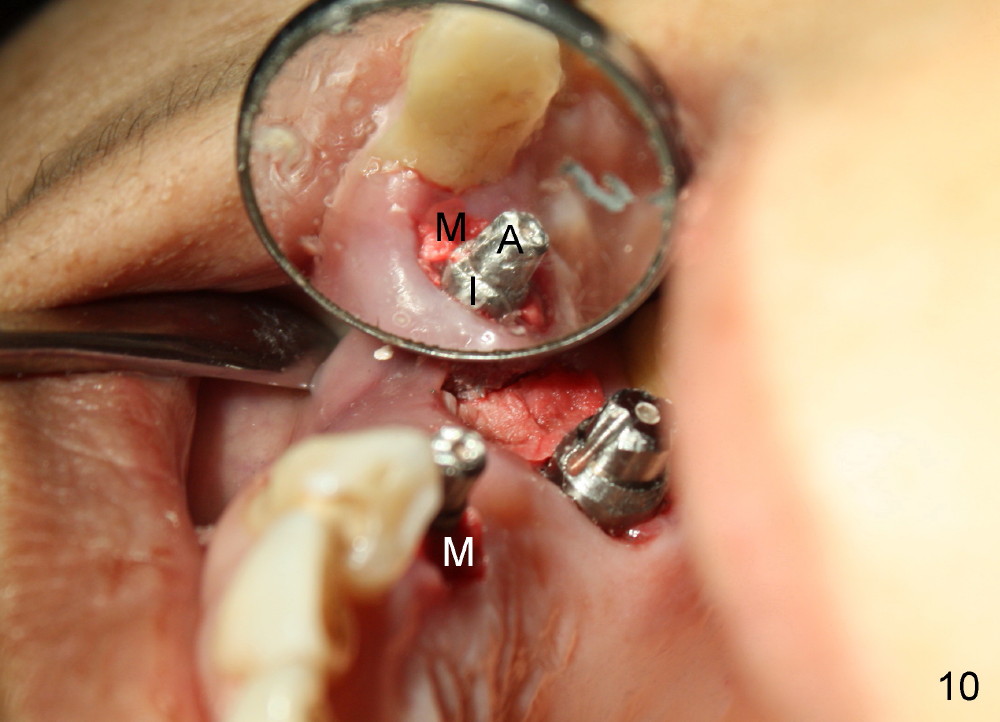
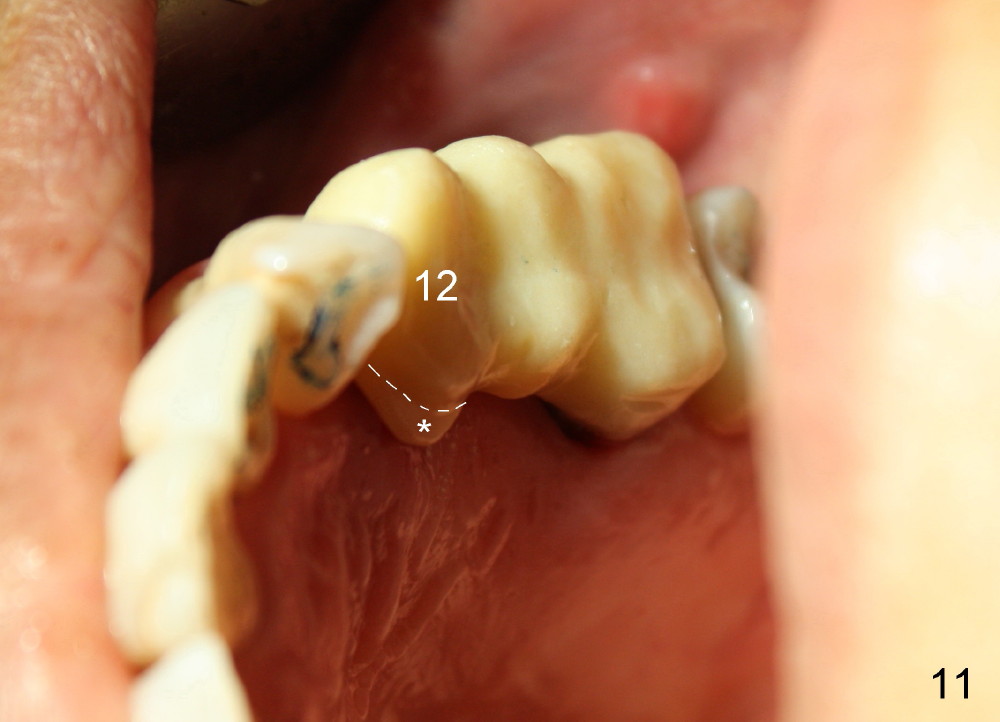
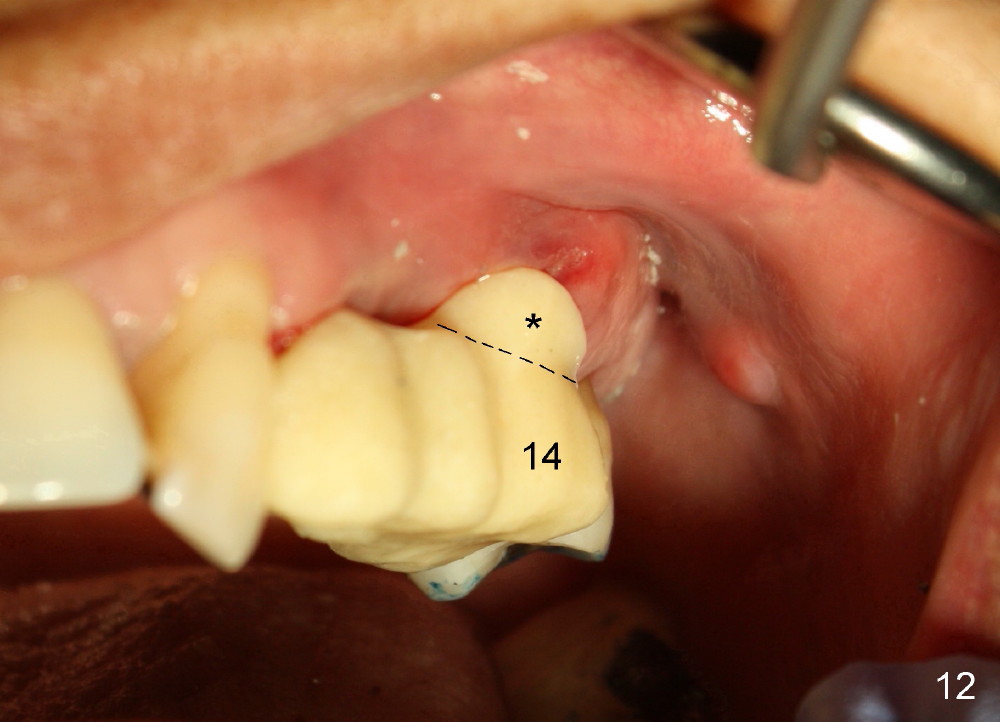
Buccal to #14 implant/abutment is a large defect, which is filled with allograft and Osteogen and covered by collagen membrane (Fig.9 M). The defect at the site of #12 is mesiopalatal, which is repaired in the same fashion (Fig.10: M). The collagen membrane is in turn protected by the "overhang" (extension) of the immediate provisional bridge (Fig.11,12 *). Once the wounds heal (Fig.13, 9 days postop), the extension is trimmed (Fig.14).
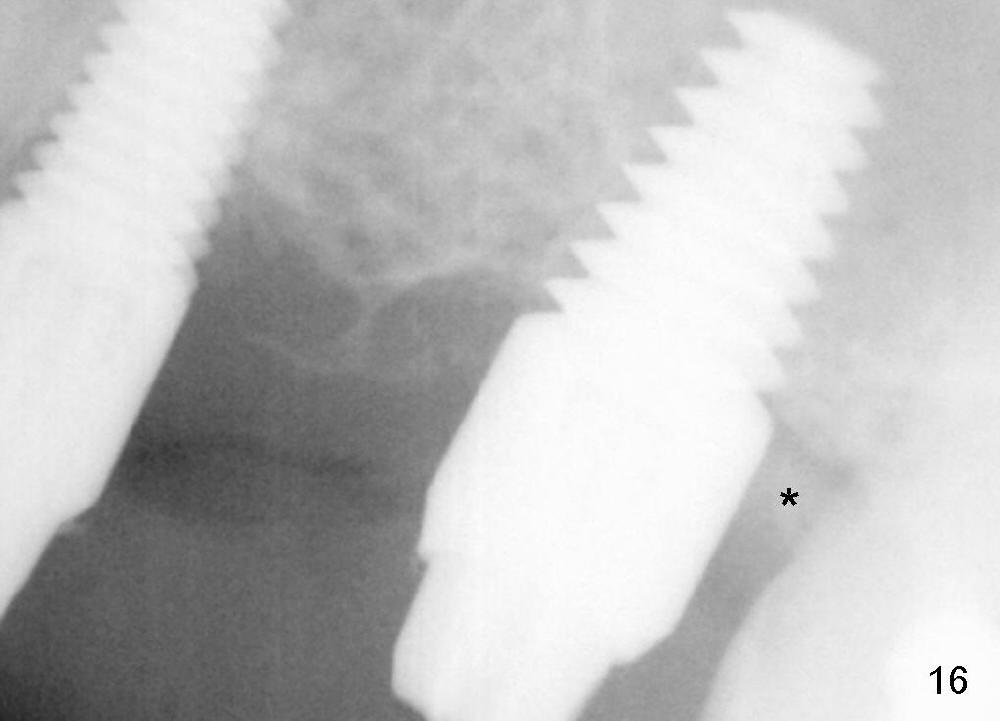
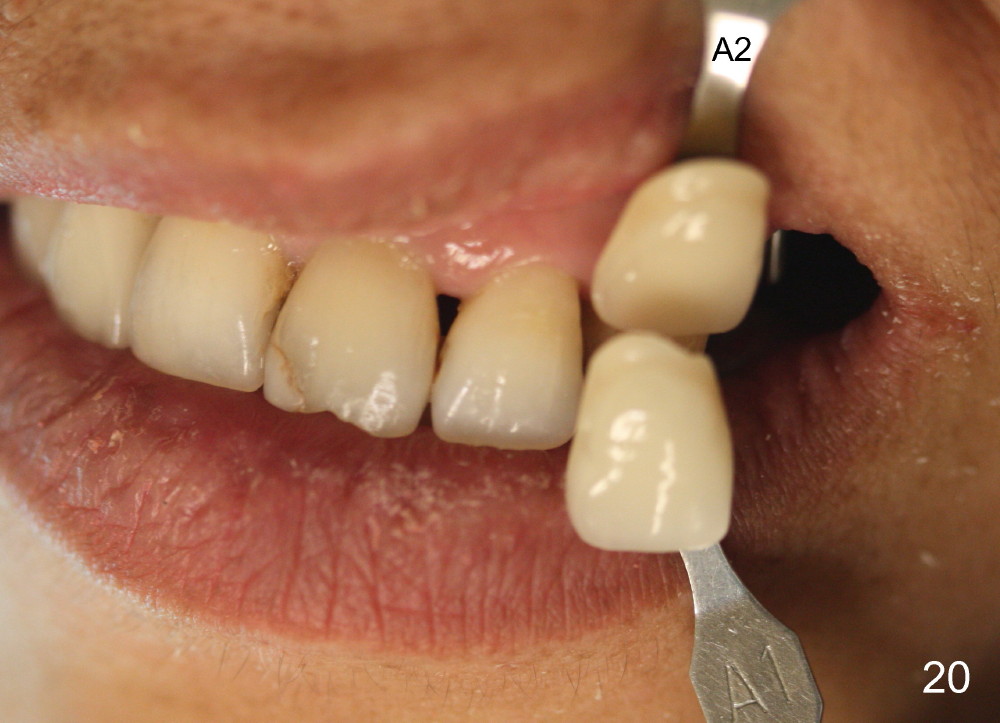
Two PAs are taken 5 months postop (Fig.15,16). Patterns of bone graft (*) between these PAs are different, which suggests presence of the graft buccal to the implant at the site of #14. Another piece of evidence of the graft is that the buccal socket heals (Fig.17 B) without implant thread exposure (Fig.19). These two implants are ready for definitive restoration (Fig.18-20). Fig.21 shows the final restoration 5 months post cementation.
Return to Upper Bicuspid,
Molar Immediate Implants,
Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 08/20/2014, last revision 01/19/2018