
.jpg)

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
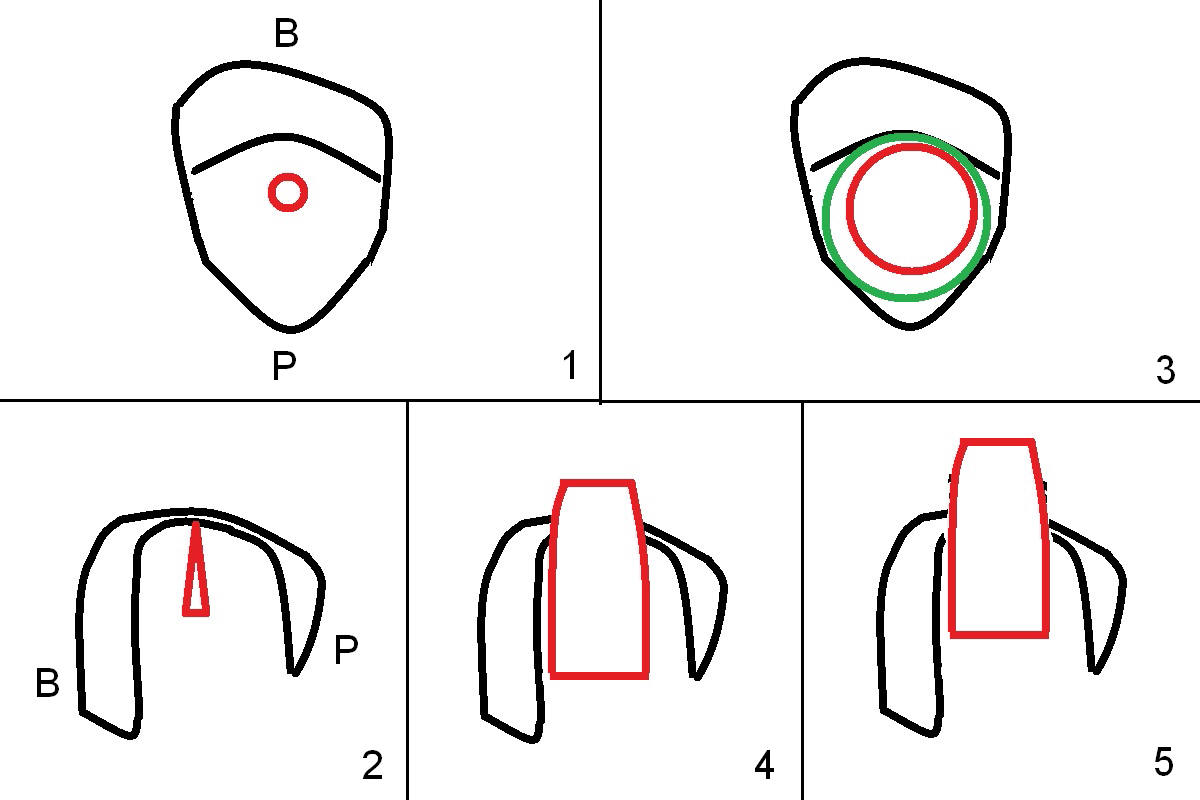
When Sinus Floor is Thin, Place Implant as Large as Possible
When the affected tooth is extracted, the suitable site for implantation is the large palatal socket. Osteotomy is initiated with Magic Expander 3.0 mm (red circle or arrow in Fig.1 (occlusal view), 2 ((coronal section)) as buccally as possible, since the palatal plate (P) is shorter than the buccal one (B in Fig.2). The sinus floor turns out to be thin. When the osteotomy at the sinus floor increases equivalent to the apical diameter of a 5 mm implant, a 5x9 mm dummy one is placed (Fig.6). There are two errors, one recognized immediately, the other not. The implant is placed too apically, but the sinus membrane remains intact. After placing 2 pieces of PRF membrane and allograft (.5-1.0 mm), a larger implant is placed (5.5x9 mm IBS) is placed at the palatal crestal level (Fig.4) with minimal stability. When a 6.5x4(4) mm abutment is being placed, it turns the underlying implant so that the latter is placed more apically (Fig.5,7). Ideally, a much larger implant should have been chosen (6.0 or 6.5 mm, Fig.3 green circle). In the future, tap drills should be used prior to implantation if the sinus floor is thin. The abutment in this case (Fig.7 A) is close to the tooth #15. The latter is the 2nd error not recognized earlier (Fig.6). The trajectory should have been corrected when a more definitive implant is being placed (from black line to red line).
The most encouraging news is that there is no nasal hemorrhage or graft discharge postop, thanks to use of PRF membrane and gentle placement of bone graft.
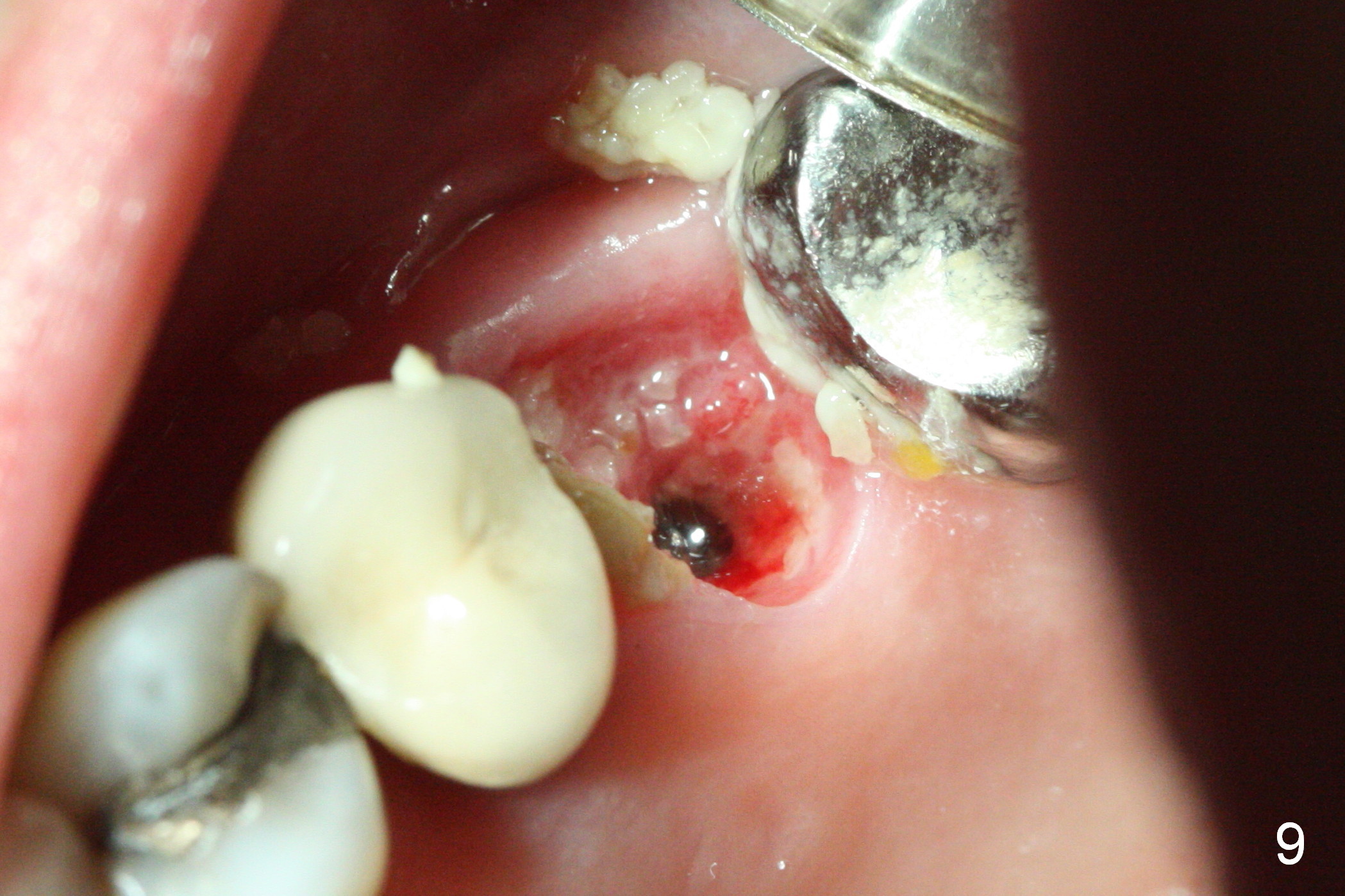
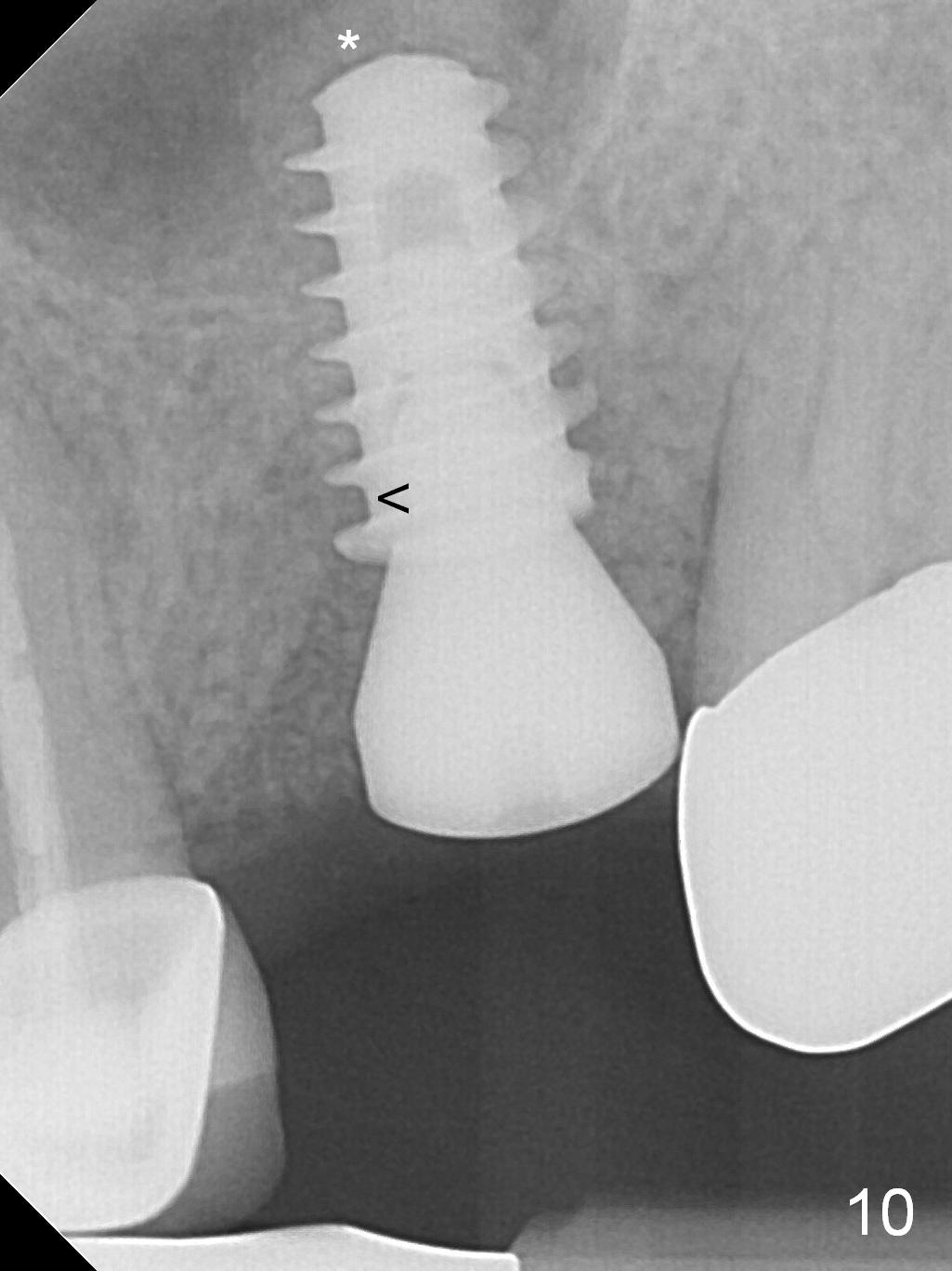
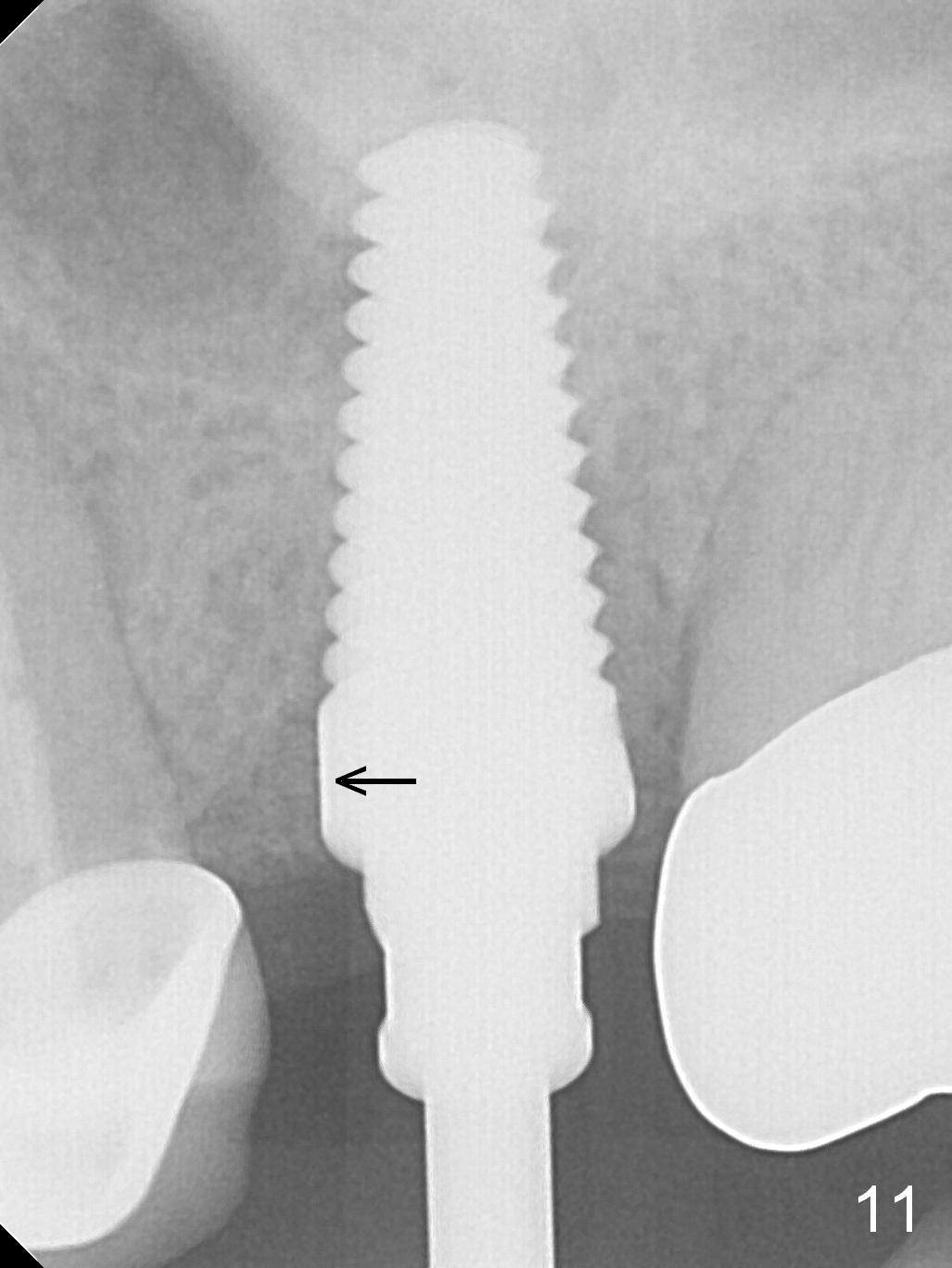
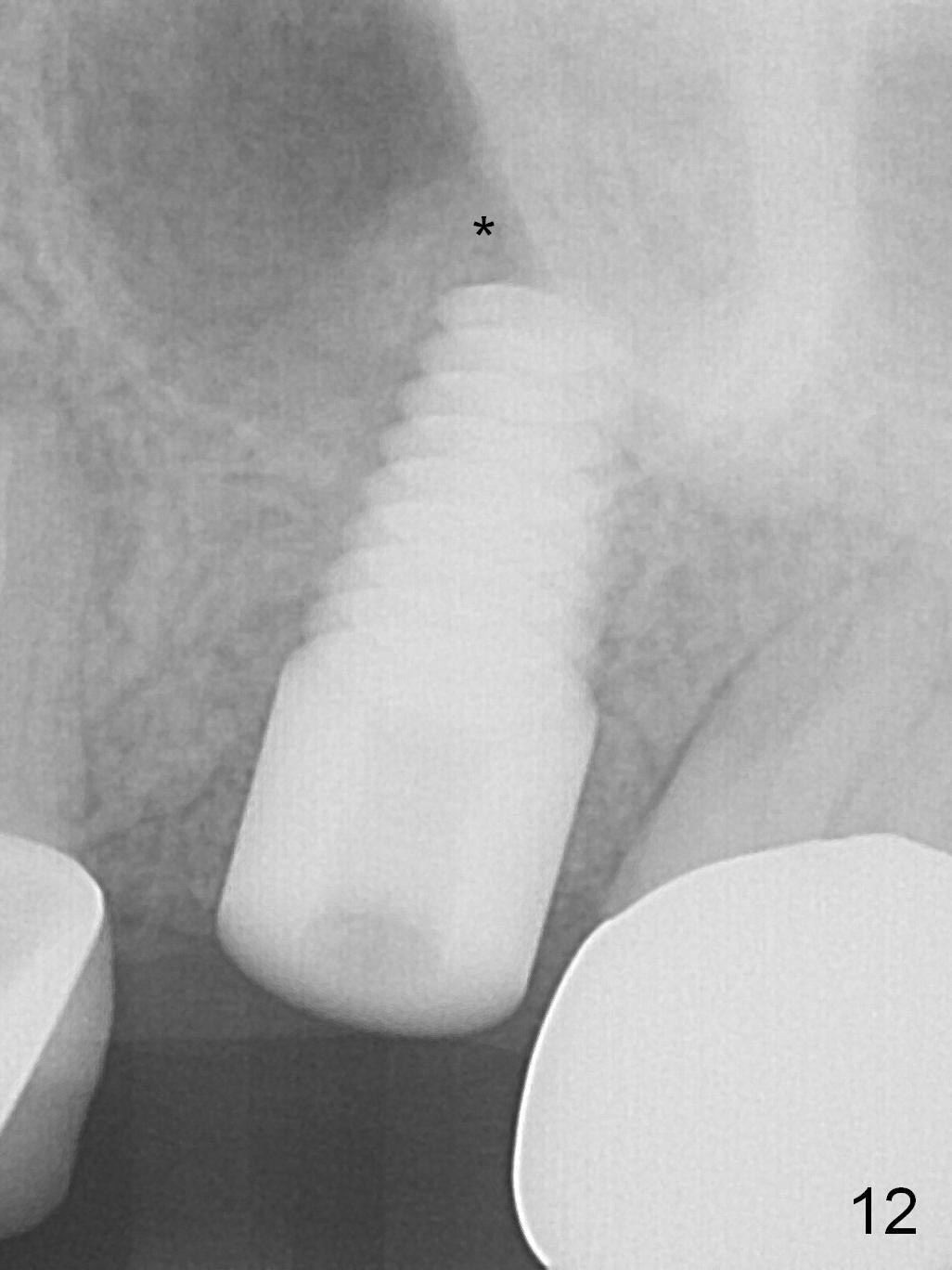
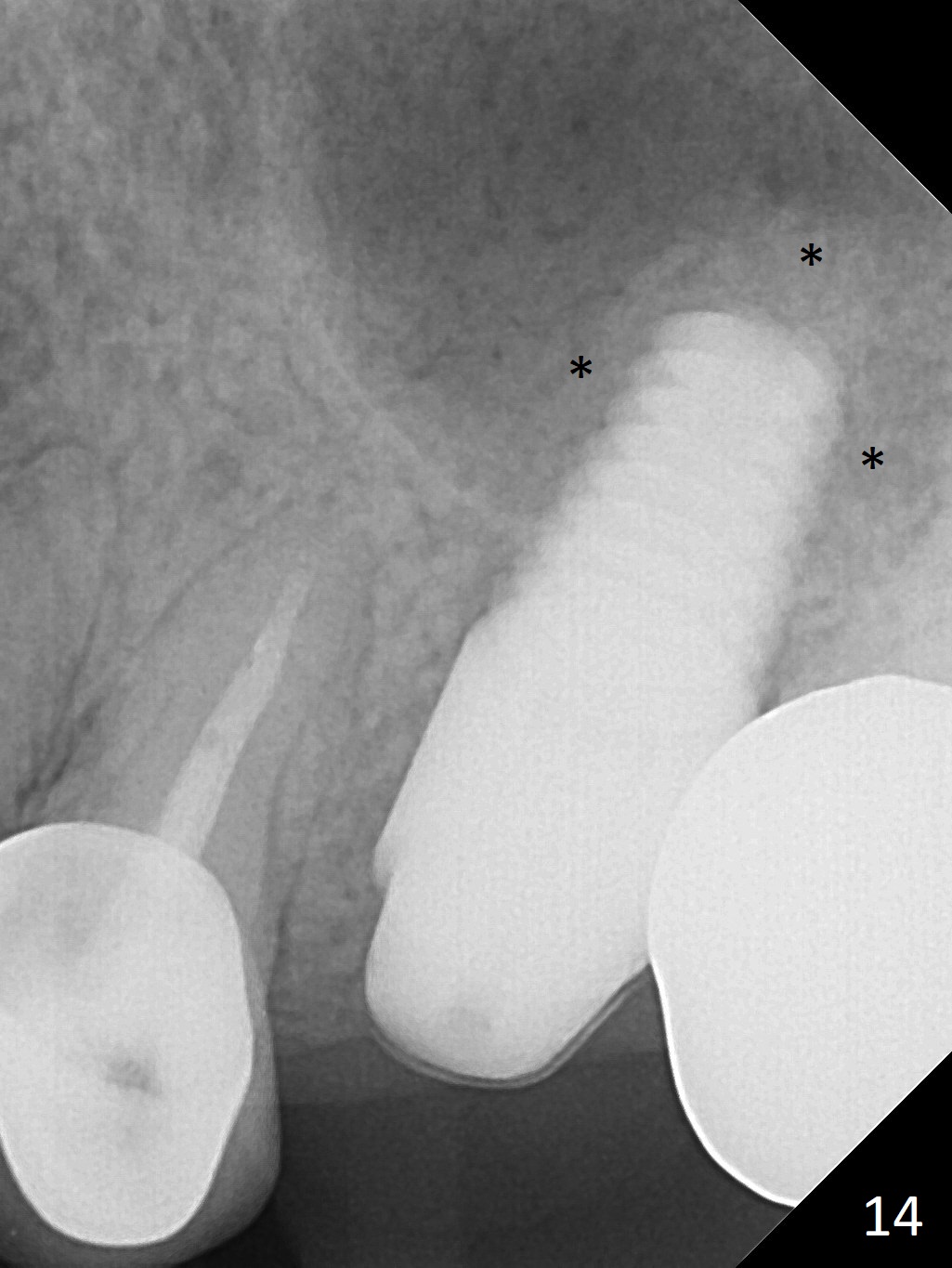
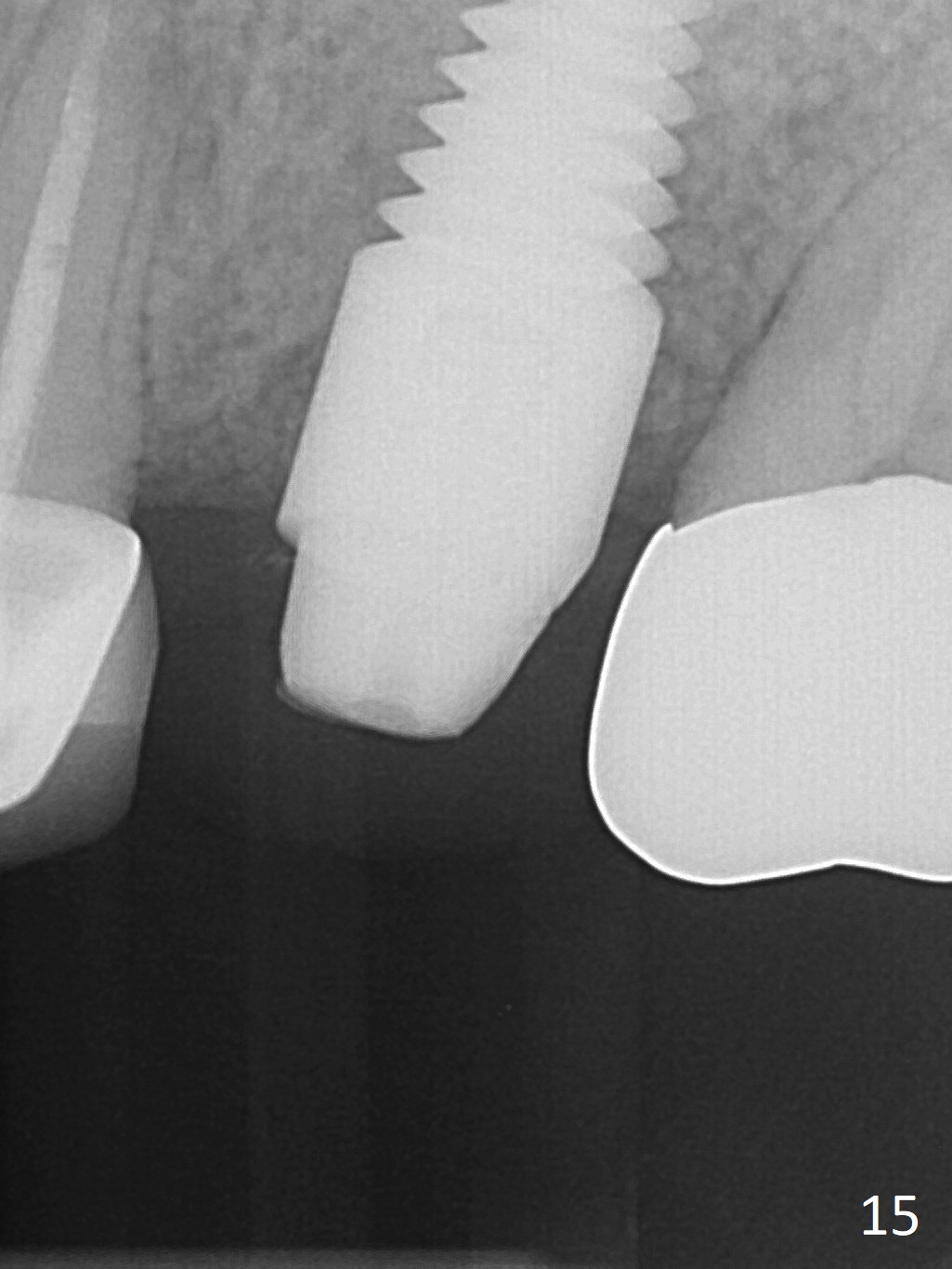
The patient is doing well 9 days postop. The immediate provisional is loose and over-sized. It is removed for trimming and reline; the socket and bone graft (Fig.8 *) are healing. It appears that an angled abutment is required next time of provisional revision. When an angled abutment is being placed 23 days postop (Fig.9), it appears to wiggle the implant due to its long leverage. Instead a healing abutment is placed. The implant is unstable 4.5 months postop with seemingly excessive bone-implant gap (Fig.10 <). The 5.5x9 mm implant is removed. A 5x17 mm tap is used to change the trajectory and sinus lift, followed by 6x17 one (Fig.11). Finally a 6x14 mm tissue-level implant is placed with insertion torque > 50 Ncm (Fig.12; vs. <20 Ncm (Fig.7,10)) and improved trajectory. An immediate provisional is fabricated to prevent the mesial drifting of the tooth #15 (Fig.13 P (*: occlusal clearance)). By using the taps and placing the longer implant, the sinus lift is more obvious (compare Fig.10 and 12 (*)). Sinus lift remains evident 3.5 months postop (Fig.14) with apparently osteointegration (Fig.15).
Return to
Upper
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table),
Dr.
Wang's Response
Xin Wei, DDS, PhD, MS 1st edition 10/24/2016, last revision 01/19/2018