












|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
<1 mm Bone Height with Soft Bone
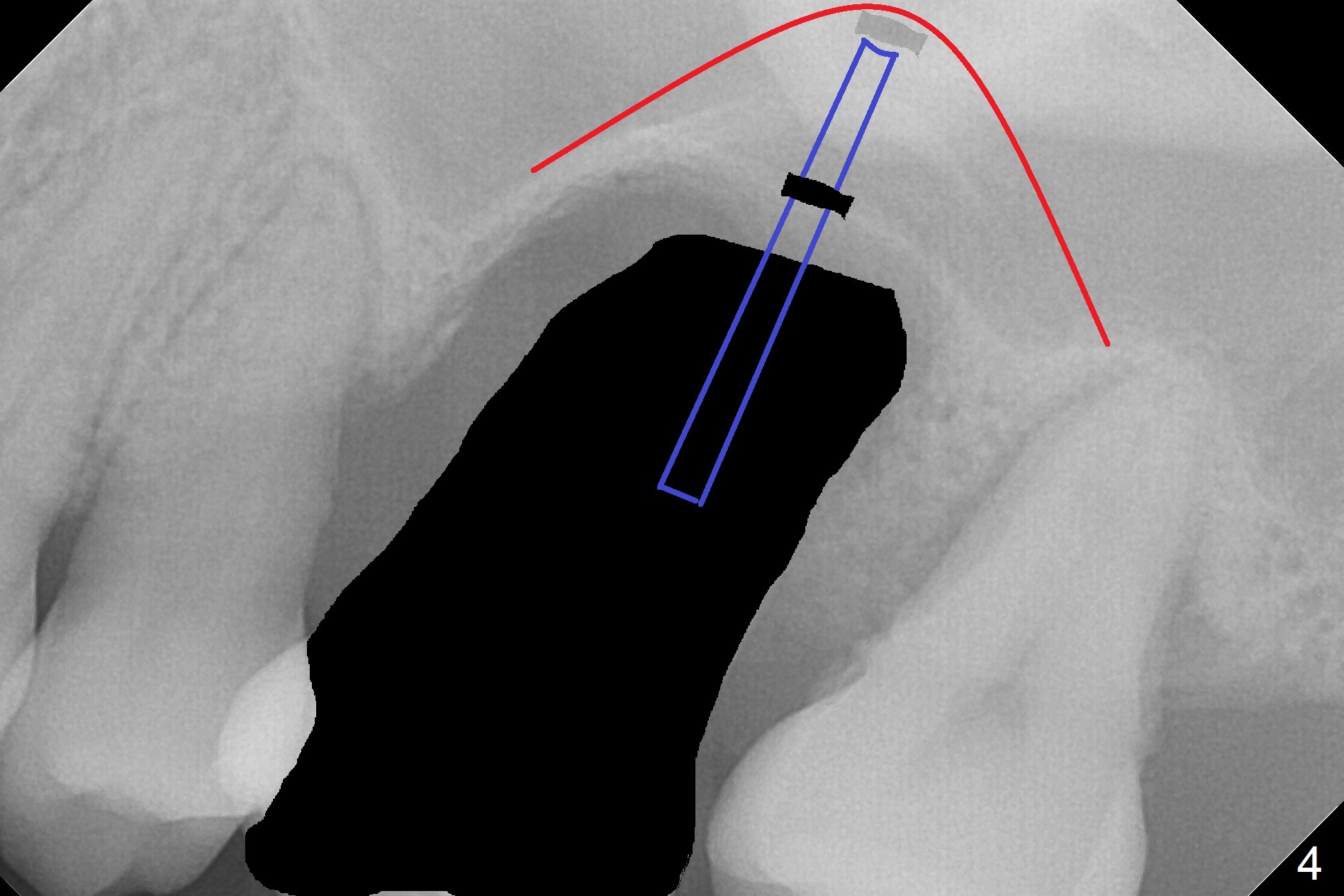
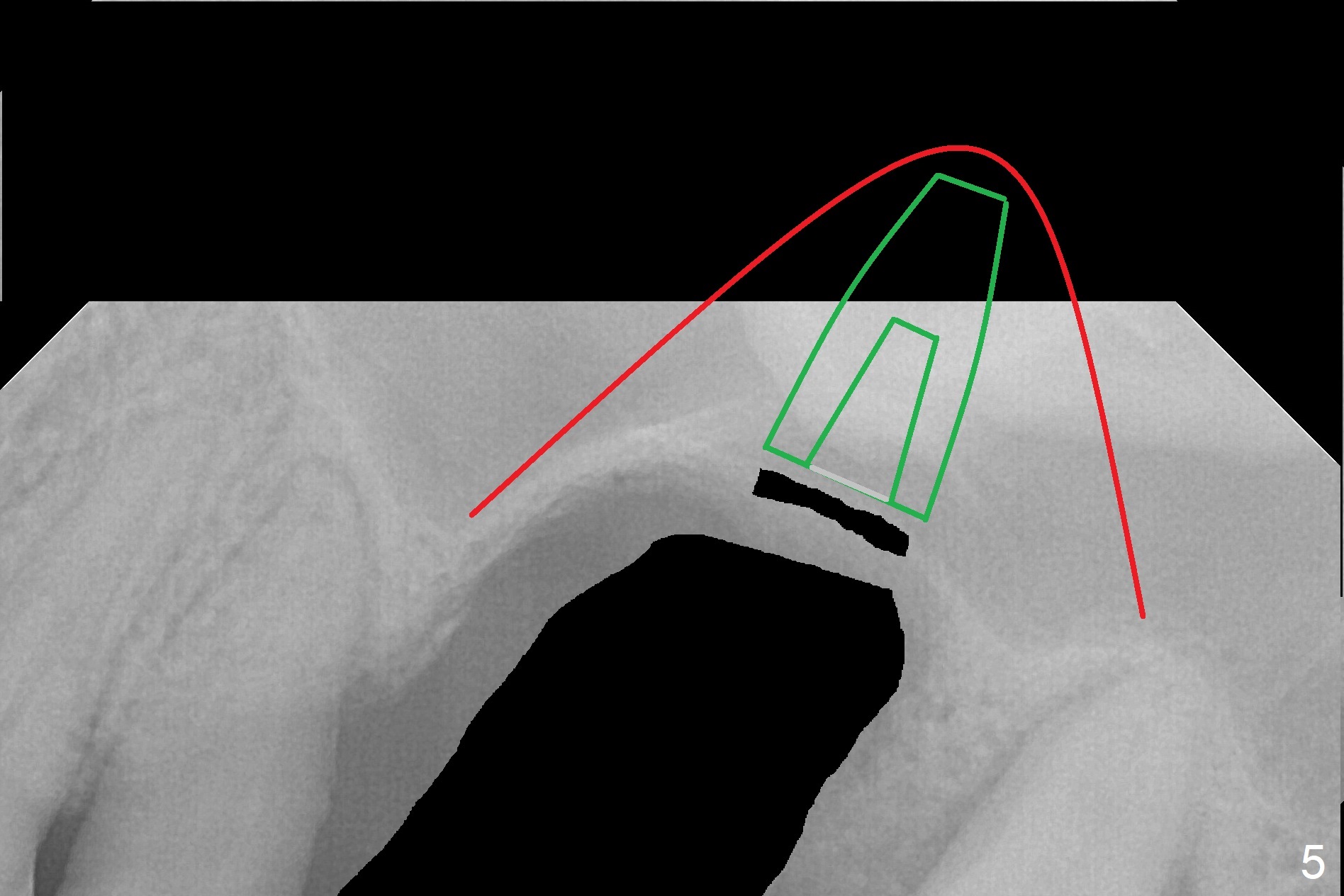
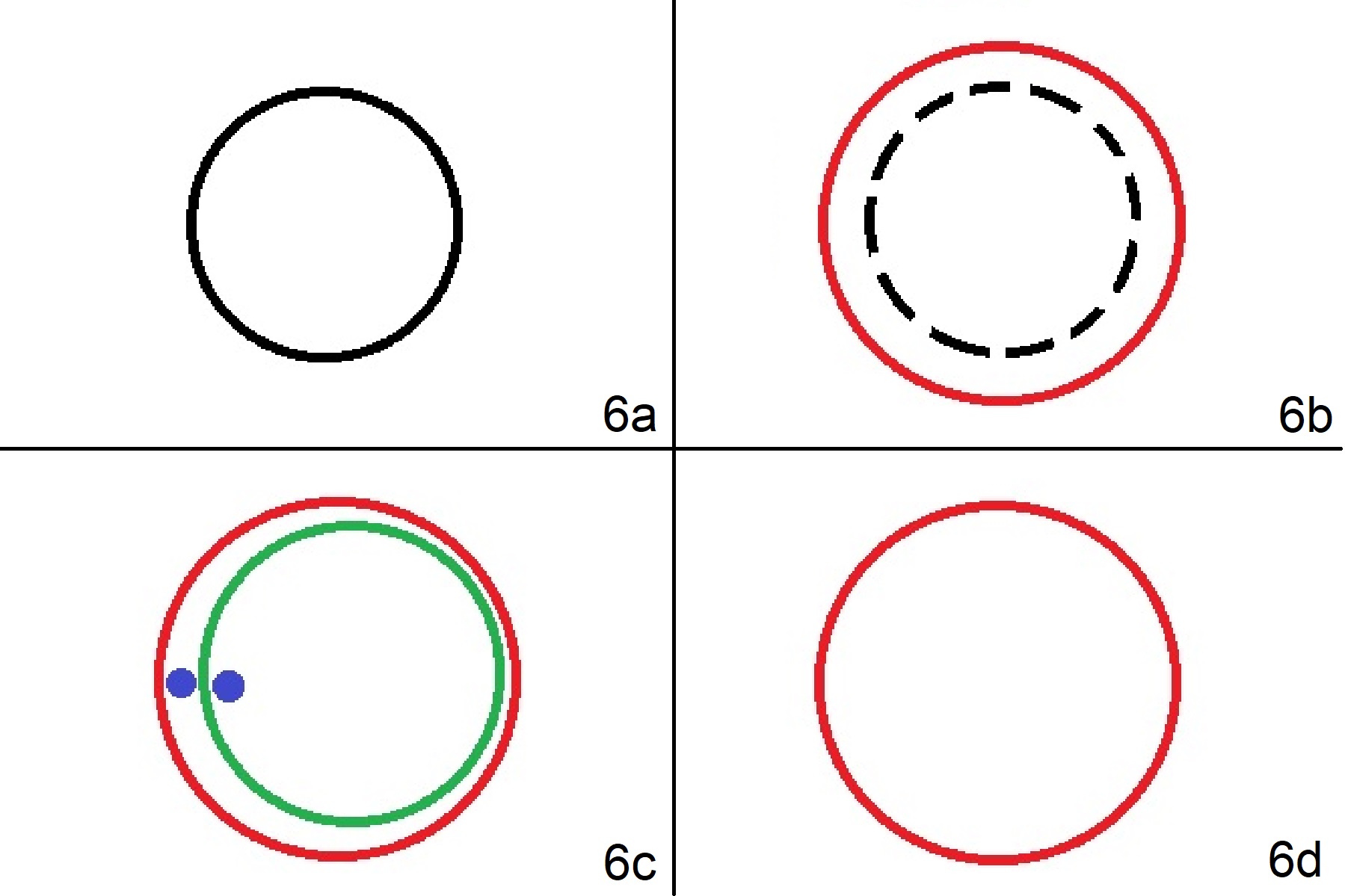
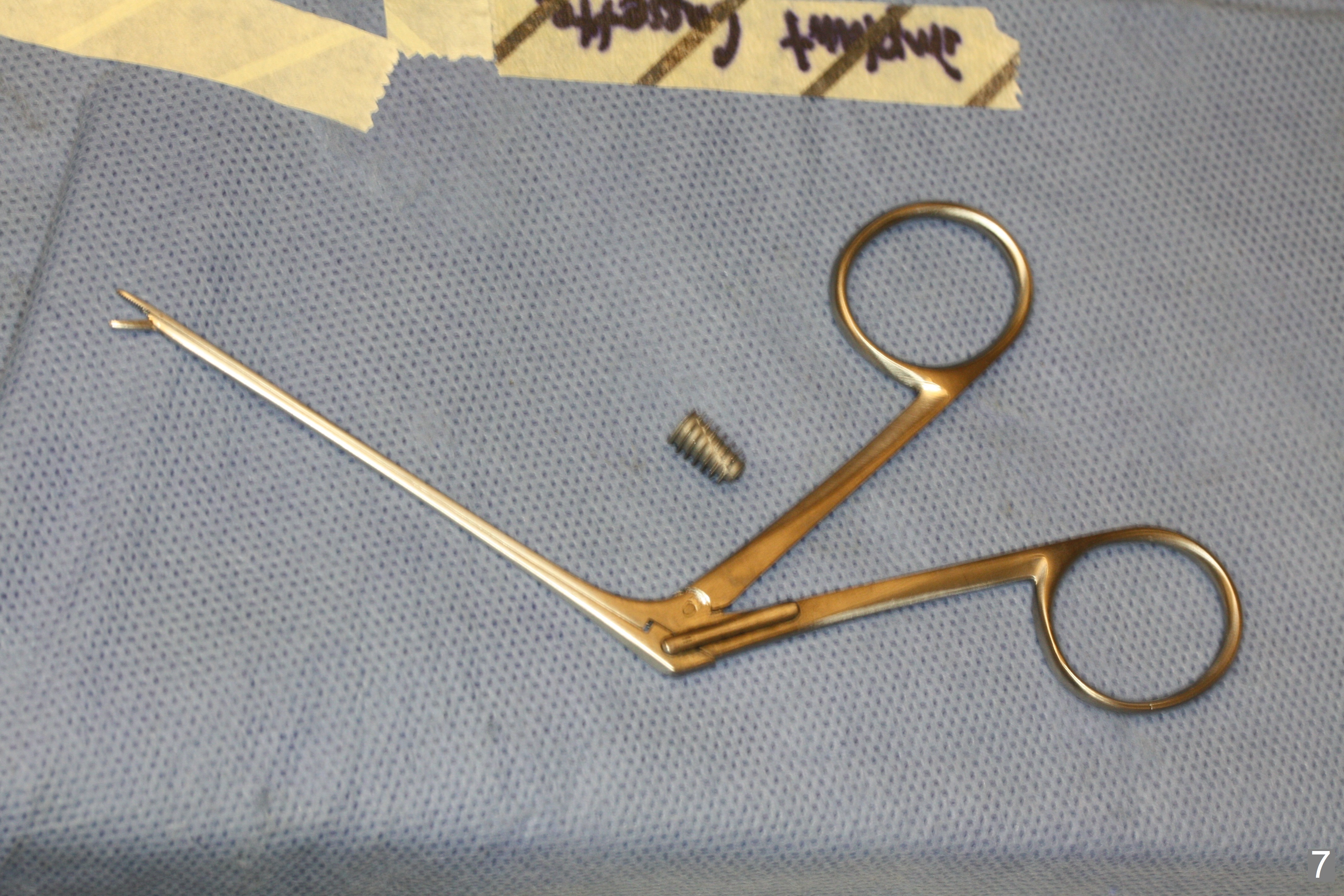
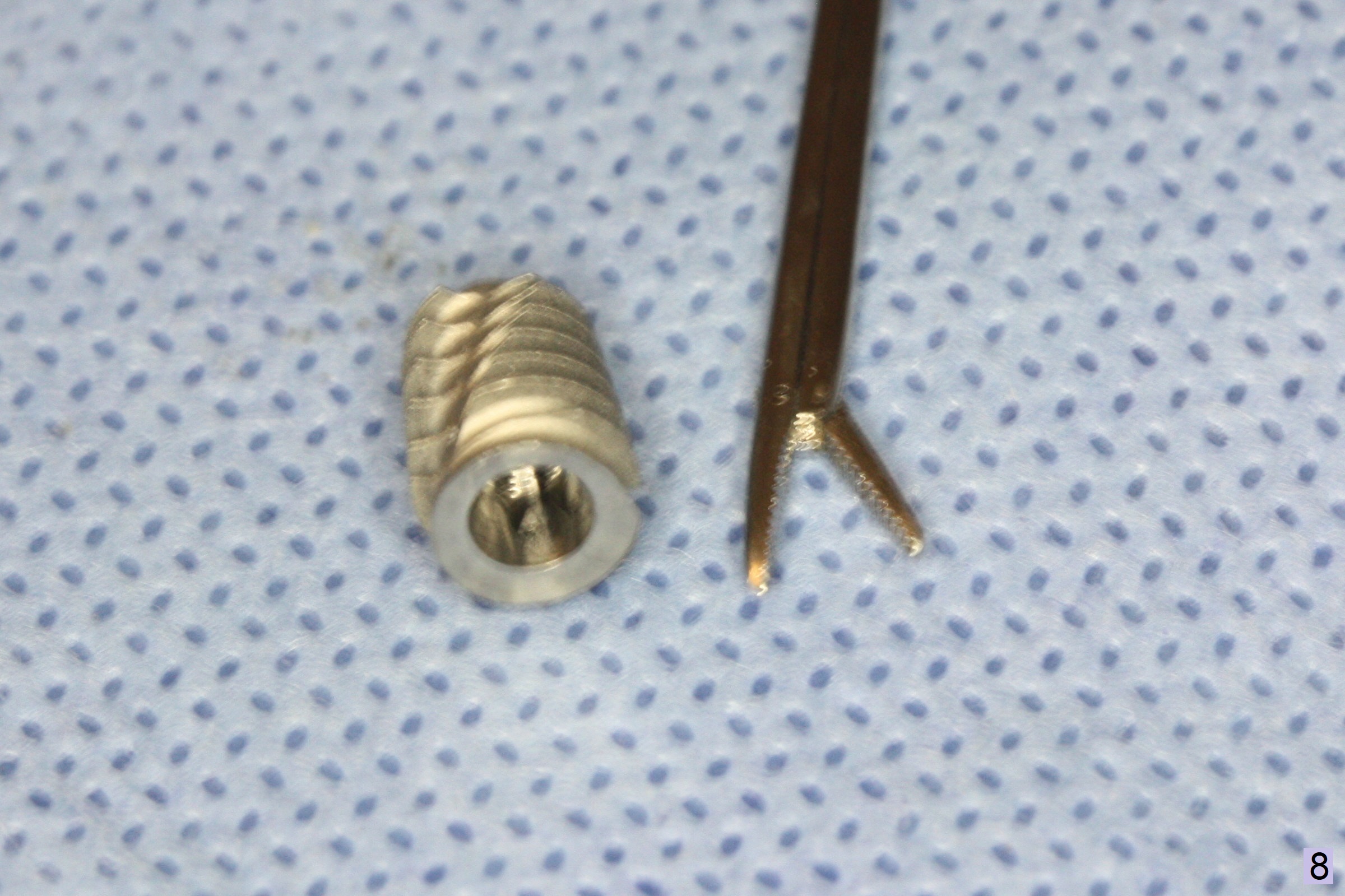
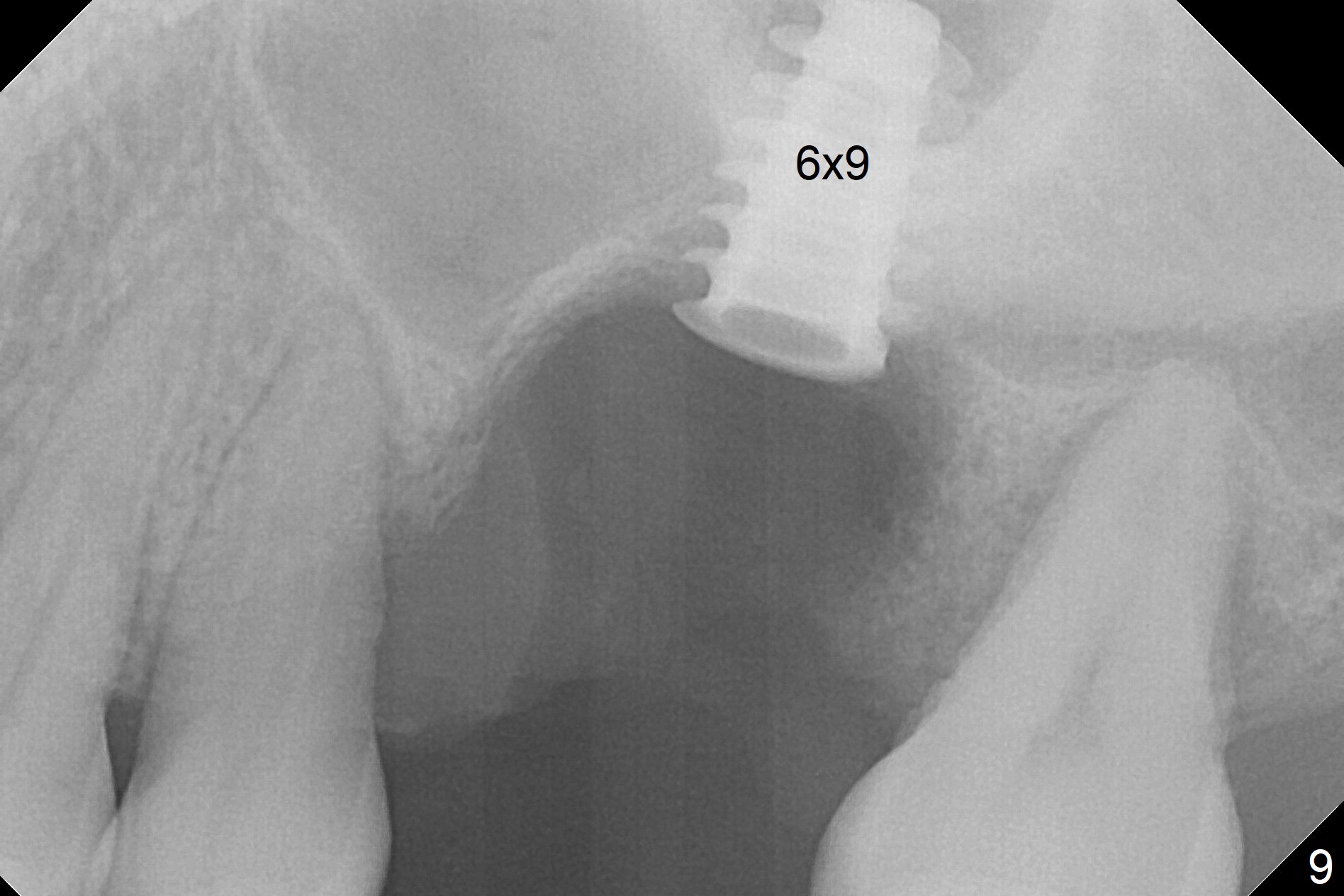
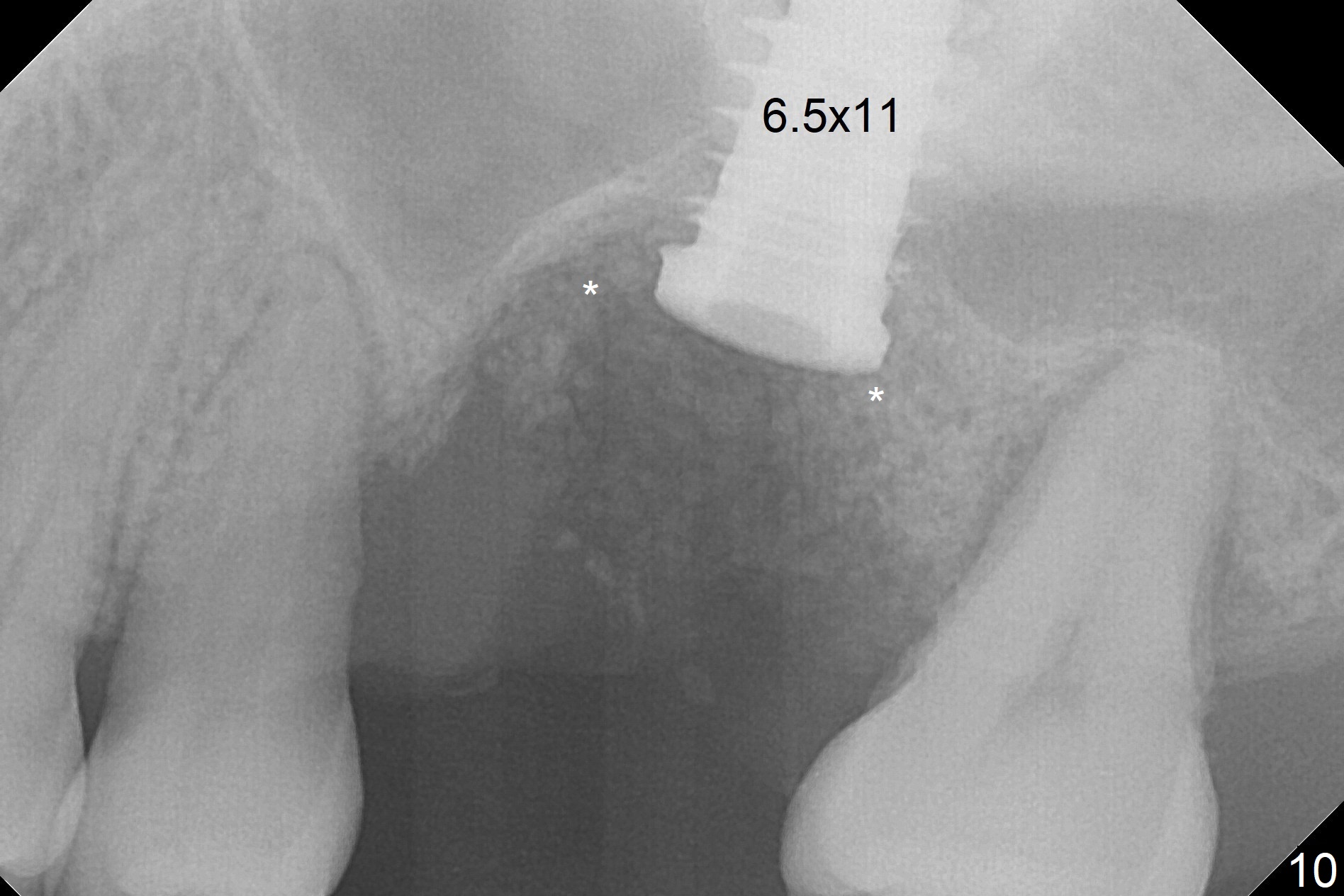
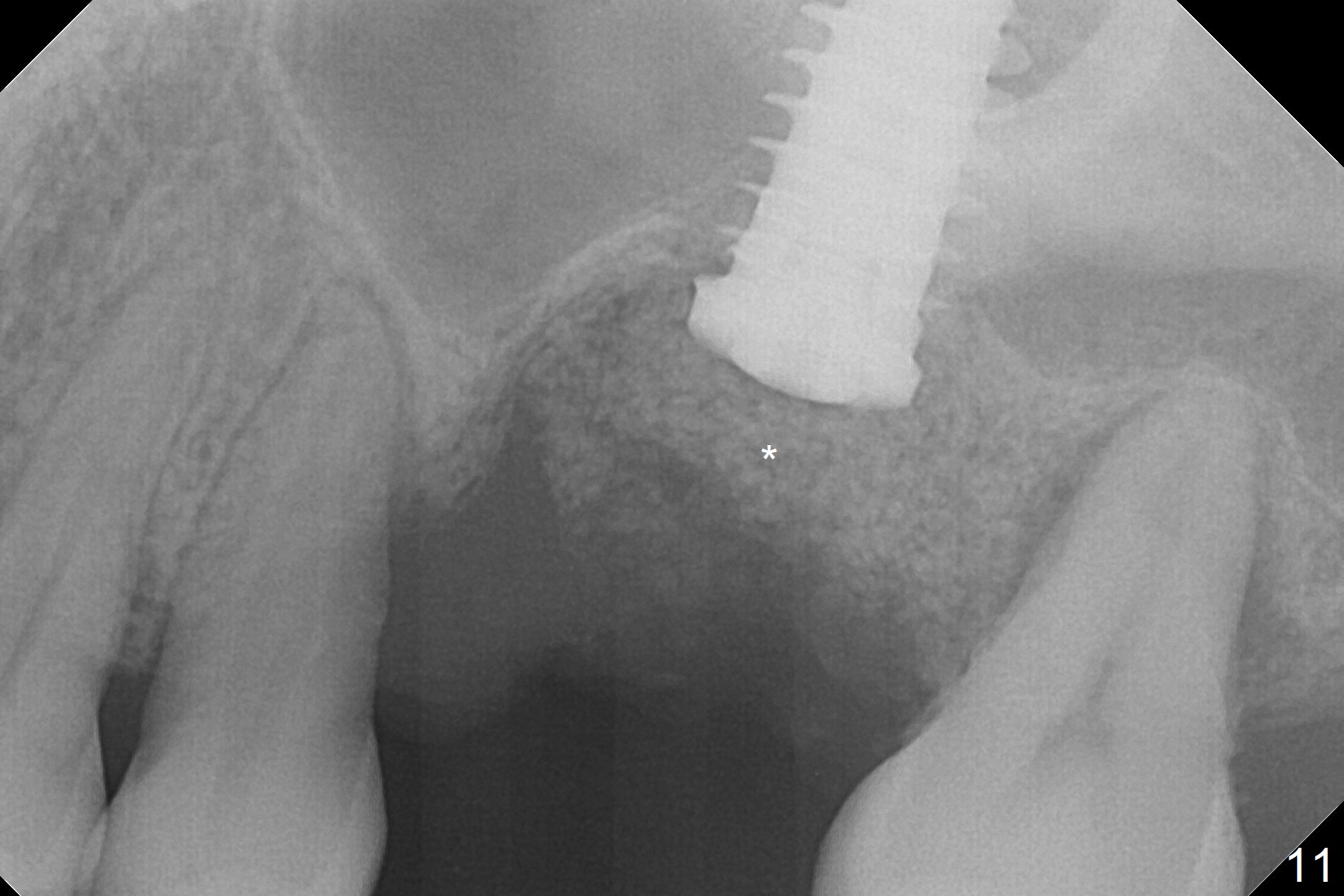
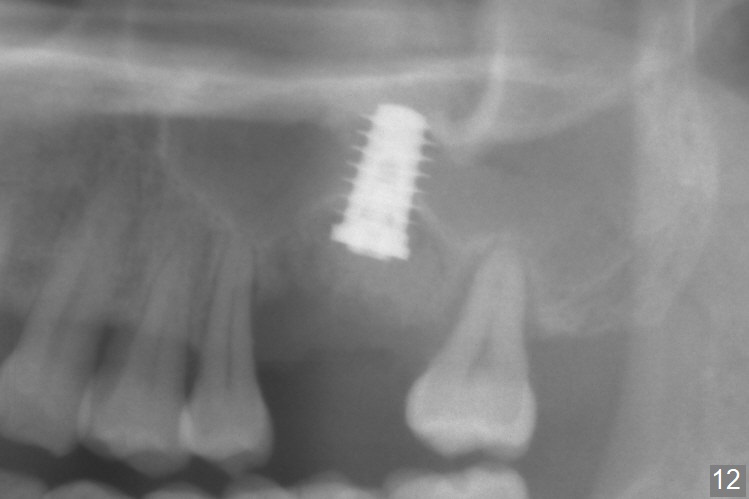
When the displaced tooth #14 (Fig.1) with palatal gingival recession (Fig.2) is extracted, the buccal plate is low, while the palatal one is lost. Osteotomy is initiated in the bottom of the large socket with Marking Drill. The bone turns bluish, suggesting thin bone (in fact less than 1 mm as well as low density). Magic Sinus Lifter (Fig.3 *, Fig.4 blue area) is used for sinus lift (Fig.4 (red curved line: lifted sinus membrane; grey area: a portion of the lifted sinus floor), followed by insertion of a piece of PRF plug and Vanilla bone graft for sinus lift. The osteotomy is enlarged lightly with 4.8 mm Magic Drill (compare black strips between Fig.4,5). A 5x9 mm dummy implant (Fig.5 green) is dislodged into the sinus. The lifted sinus membrane holds the implant in place. The black thin strip in Fig.5 and black circle in Fig.6a (occlusal view) represents the osteotomy. After increase in the osteotomy with Lindamann bur (Fig.6b red circle), the implant (Fig.6c green) is retrieved with endodontic forceps (Fig.6c two blue dots (beaks of the forceps); Fig.7,8). With the enlarged osteotomy (Fig.6d), a 6x9 mm dummy implant is placed deep (Fig.9). The definitive implant is 6.5x11 mm with insertion torque ~ 15 Ncm (Fig.10). With placement of a healing screw and further placement of allograft (Fig.11 *), the socket is closed with PRF membrane and collagen plug (Fig.12).
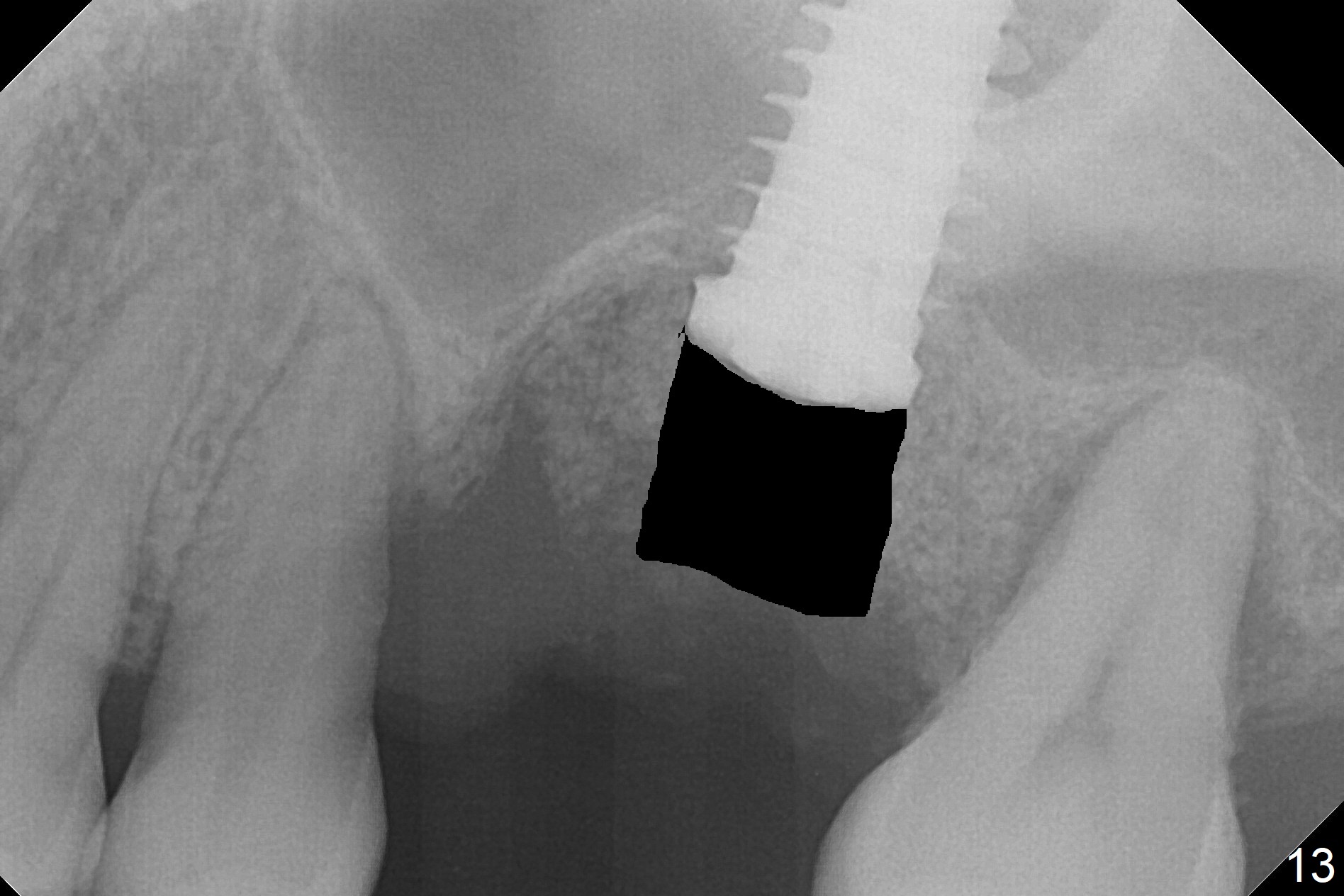
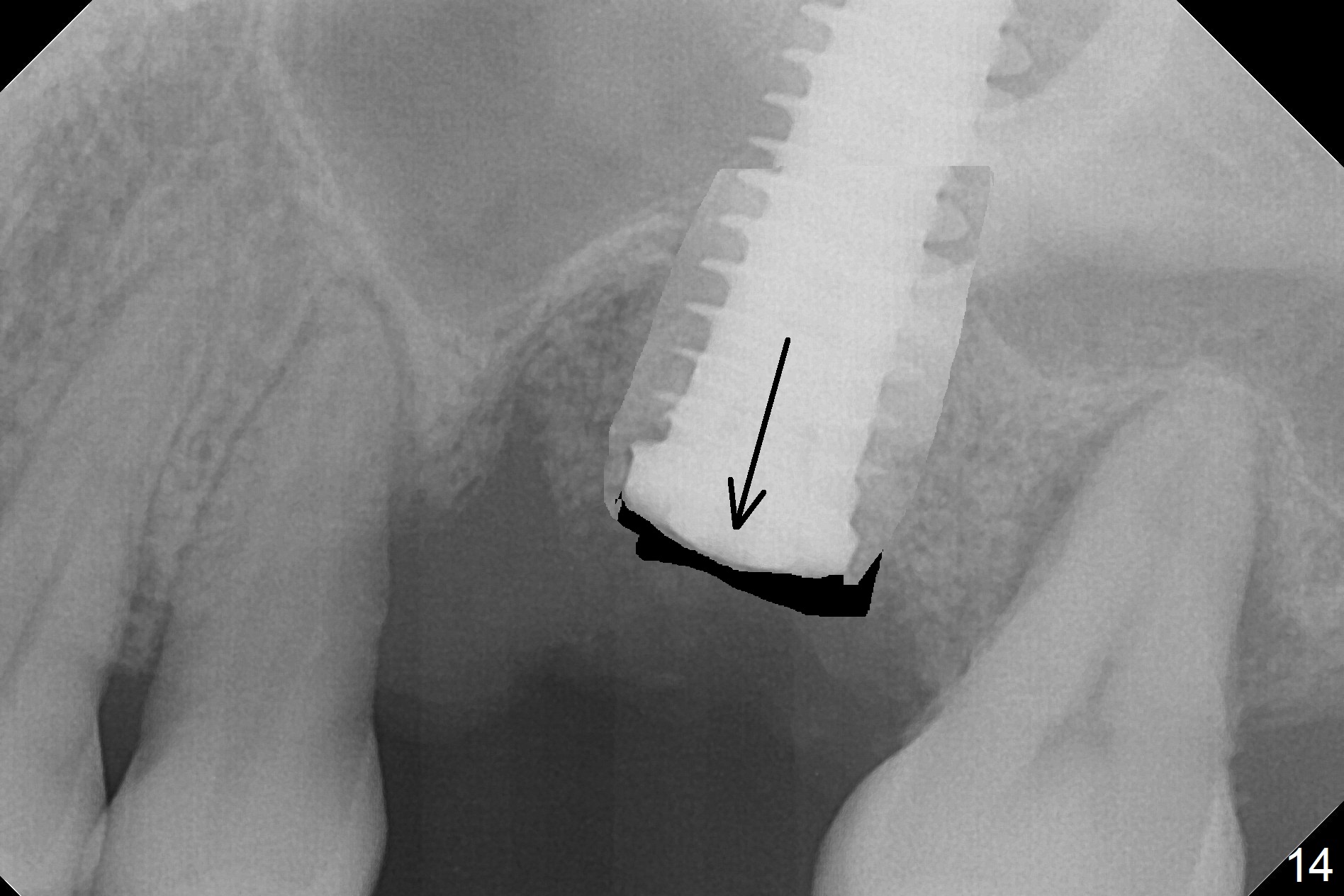
Questions for Dr. Wang: Can we remove the coronal portion of the bone (Fig.13) and back up the implant (Fig.14 arrow) 4-5 months postop for easy restoration? If it is not a good option, can we produce pair abutments with 5 and 7 mm cuffs?
Dr.Wang's comments
2. I predict that the bone above the implant will only be about 1-2 mm. In other words, your idea of backing up the implant will only be about 1-2mm possible.
3. Assuming that 1-2mm of backing up the implant will be sustainable, since stability will still be secure, let heal a month more after backing up, then use cuff 4 abutment to restore.
Poor visibility for immediate implant in the molar region is another contributing factor for the dislodgement. The patient returns for follow up 15 days (Fig.15) and 1 month (Fig.16) postop. Bone graft seems to be stable around the implant. The socket heals 4 months postop (Fig.20). The implant seems to have been osteointegrated (Fig.17,18). It will be backed up for ~ 3 mm to improve implant/crown ratio (Fig.19, as compared to Fig.14). If it cannot be done, take impression immediately and make a subgingival provisional before suturing.
In fact, there is no coronal bone for the implant to be backed up. Therefore, impression is taken after uncover and insertion of a 5.5x5.7(4) mm abutment.
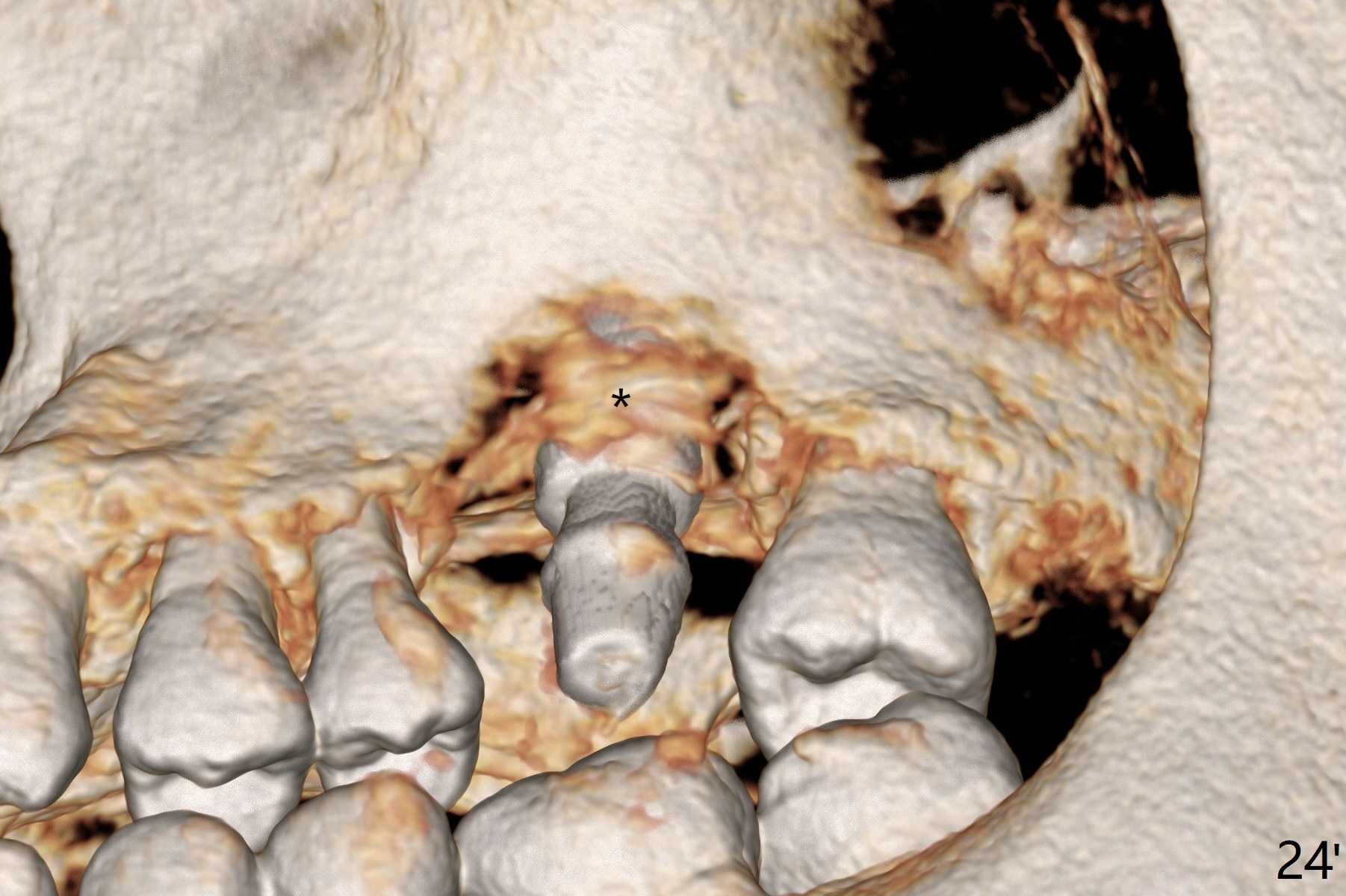
There is a mushroom around the implant nearly 5 months postop/immediately before cementation (Fig.21). The bone density around the implant is low (Fig.22-24' *).
Return to
Upper
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table), IBS,
#3,
MAGIC
FC 植入方法, Course
1
2
3
4
Xin Wei, DDS, PhD, MS 1st edition 09/07/2017, last revision 04/14/2019