





|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
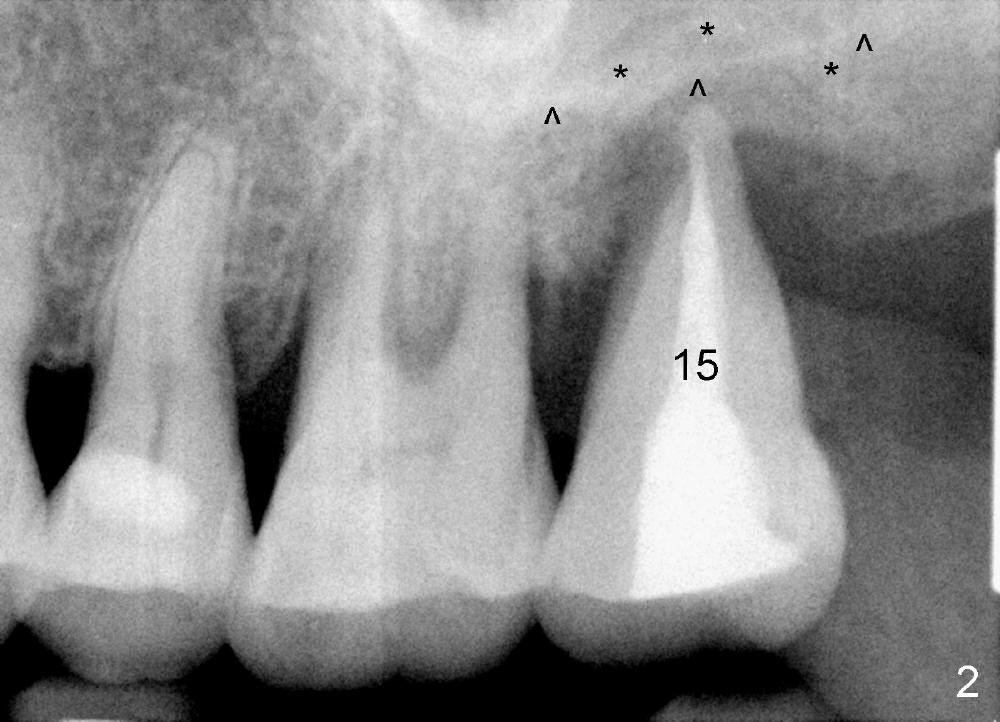
Gingival Recession
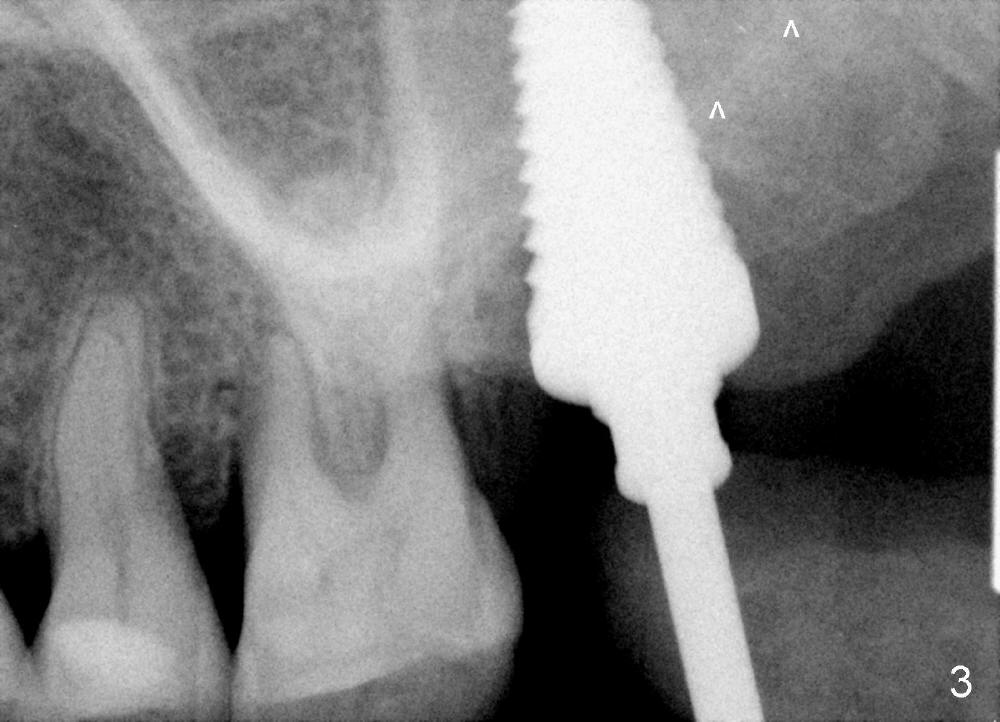
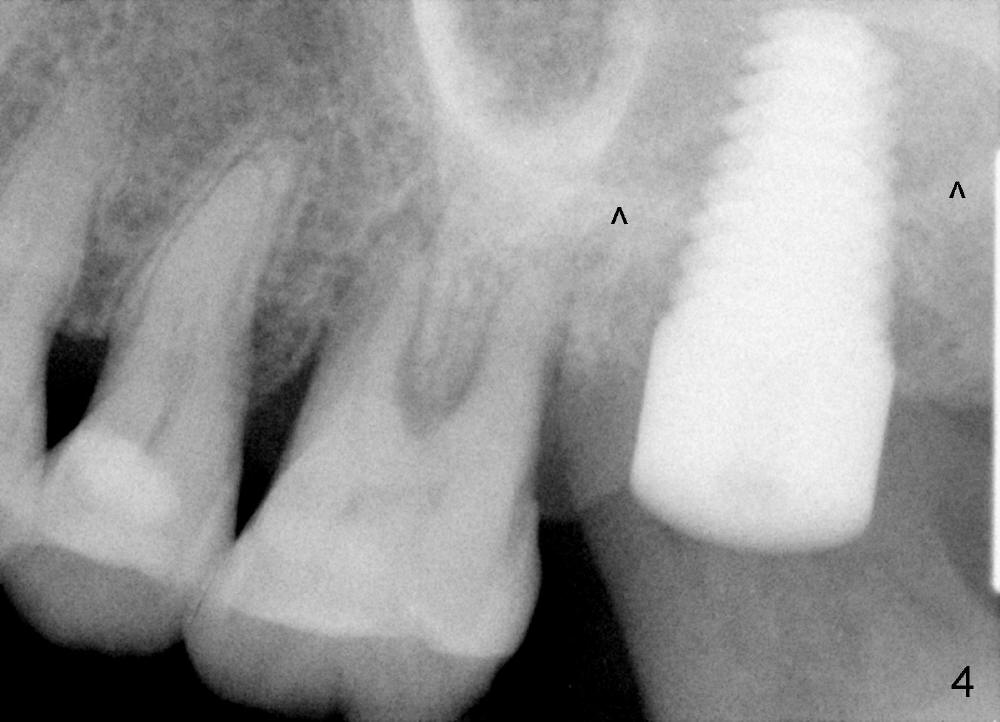
A 56-year-old female has recurrent infection and buccal gingival recession (Fig.1 *) after root canal therapy in the upper left 2nd molar (Fig.2). The extraction socket is single and large. Osteotomy forms by using a series of osteotomes (2-5 mm in diameter) mesiopalatal to the center of the socket. The sinus floor is thin (approximately 2-3 mm). The osteotomy is further enlarged by inserting 4.5-8 mm taps at the depth between 14 and 17 mm from the gingival margin. The last tap has barely achieved stability (Fig.3). It appears that the tap has almost obliterated the socket. Allograft is pushed into the sinus before placement of a 8x17 mm implant. The insertion torque is between 15 and 20 Ncm (Fig.4). The gingiva-level implant is slightly subgingival except buccal (Fig.5). To facilitate buccal gingival re-growth and cover the exposed implant surface, bone graft is placed subgingival (Fig.5 ^). The gingival sulcus is closed partially by placement of a thin strip of collagen membrane (not shown). The wound is protected by applying perio dressing.
Sinus membrane integrity is checked several times intraop: there is no air leakage. There is no nasal hemorrhage or obstruction intra- or post-op. The patient returns for follow up 12 days postop; the perio dressing remains in place (Fig.6).
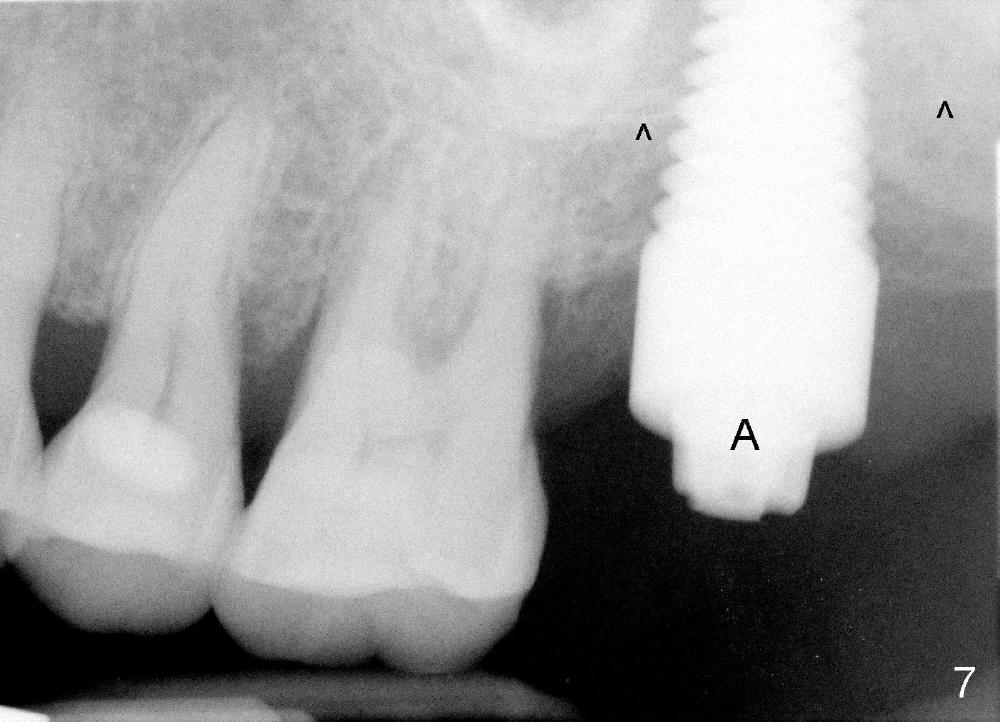
Next time she returns 4.5 months postop, bone looks normal around the implant (Fig.7), whereas the buccal gingival recession appears to get worse with 1-2 implant thread exposure (Fig.8 >). To avoid this complication, the initial osteotomy should be placed as palatal as possible; when the implant is placed with gingival recession (Fig.5), soft tissue graft should be performed. The implant should be smaller.
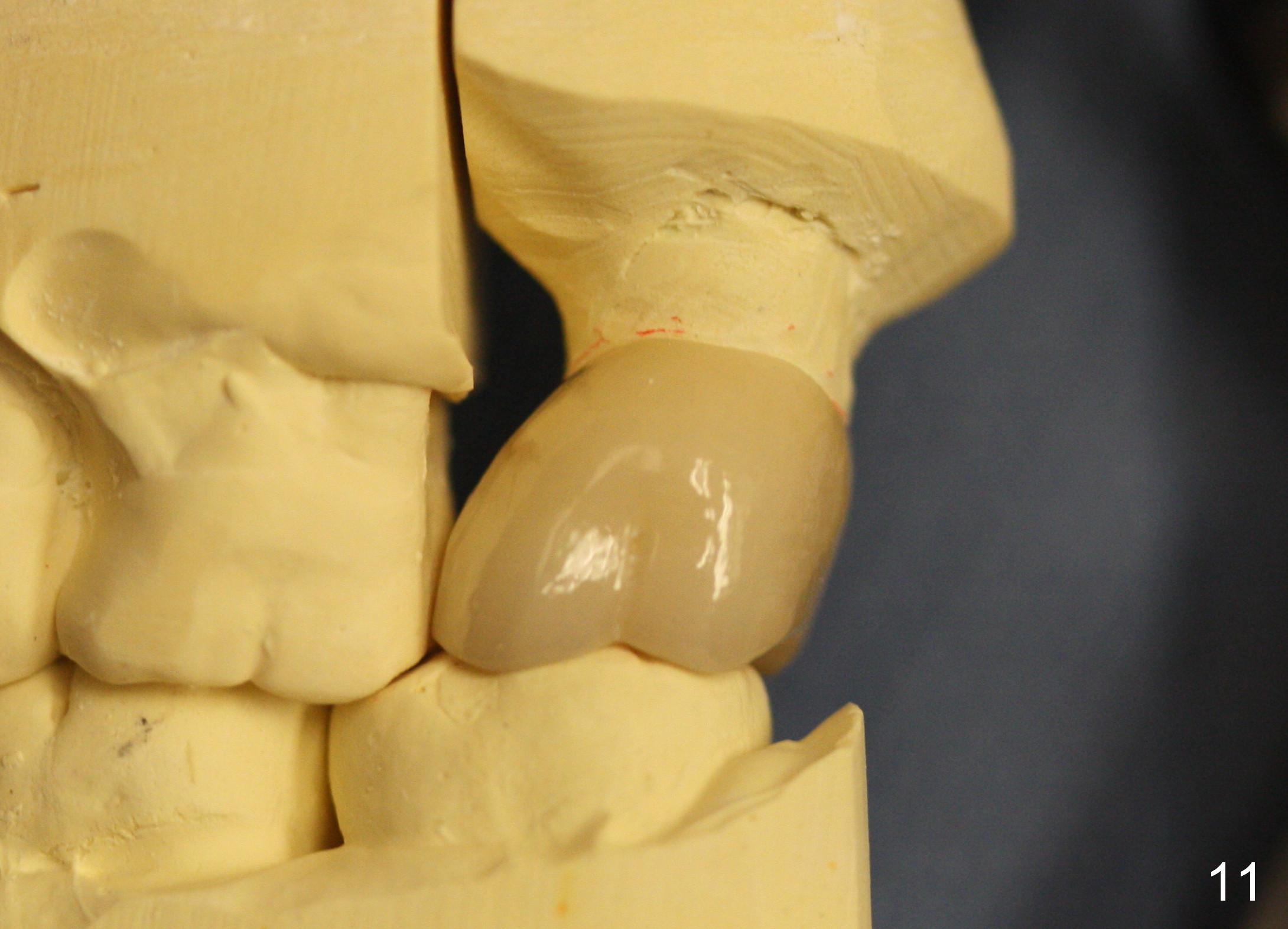
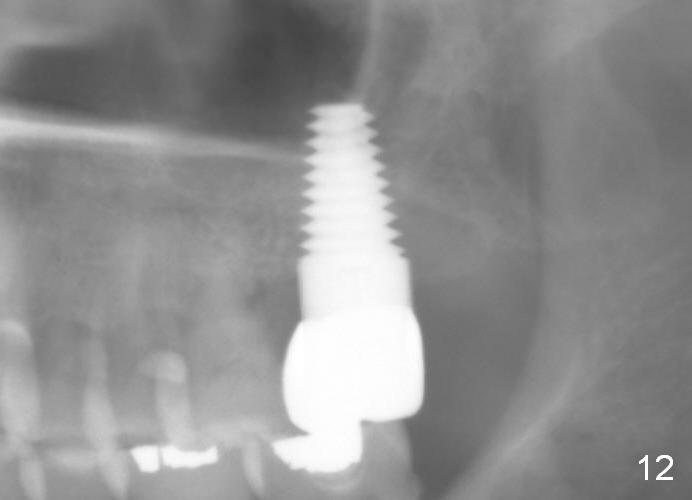
Model study shows that the implant is placed distally (Fig.9,11) in addition to buccal implant exposure (Fig.10 arrowheads). Postop, the patient complains of upper left discomfort, which is more likely associated with furcal infection of the tooth #14. The symptom disappears after use of water pik. Panoramic X-ray is taken 6 months post cementation (Fig.12).
Return to
Upper Molar Immediate Implant
31
14
18
Xin Wei, DDS, PhD, MS 1st edition 06/06/2014, last revision 02/28/2020