

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Prevent Tooth Shifting During Osteointegration
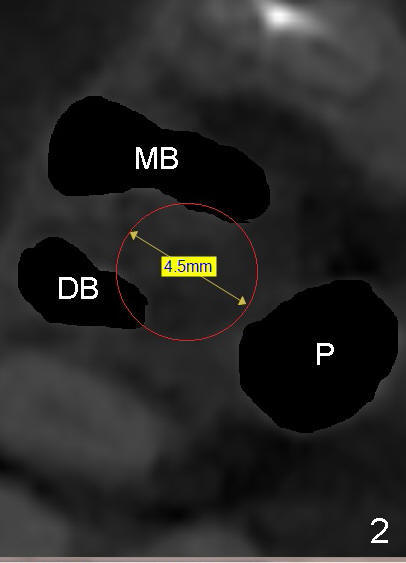
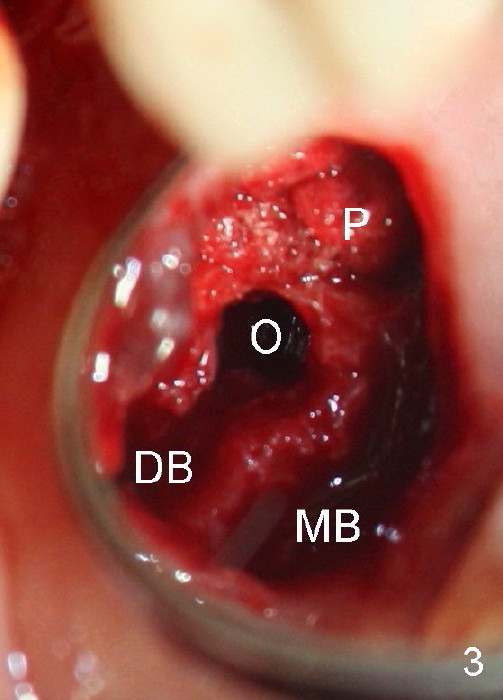
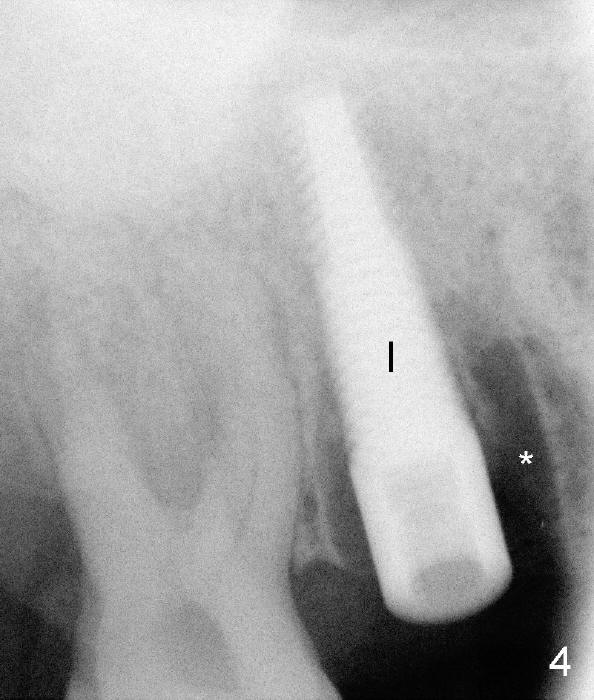
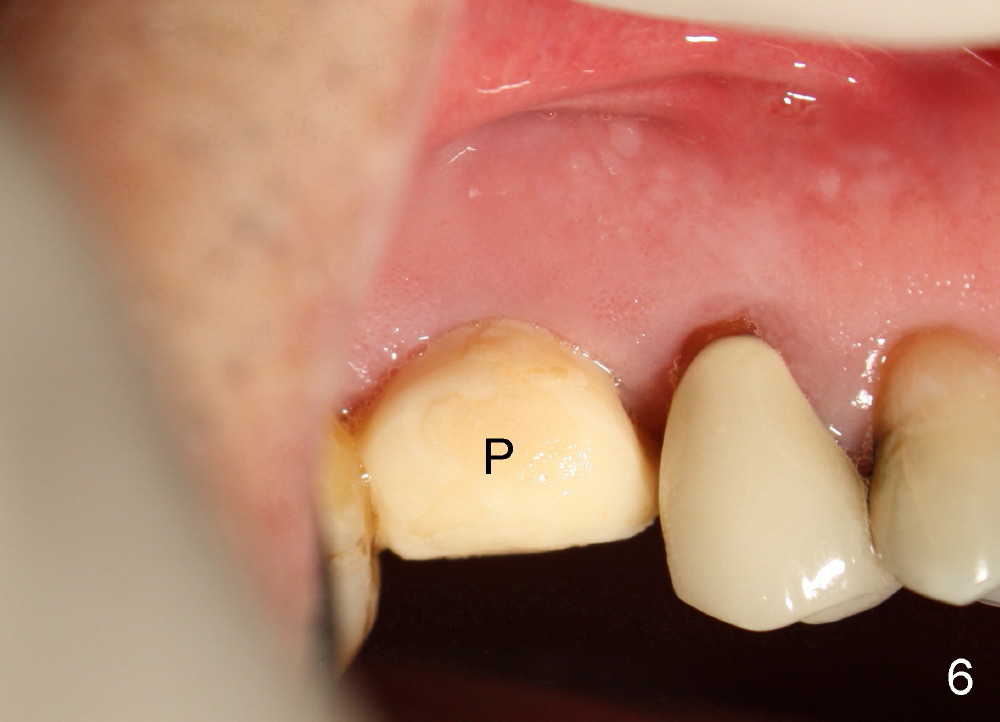
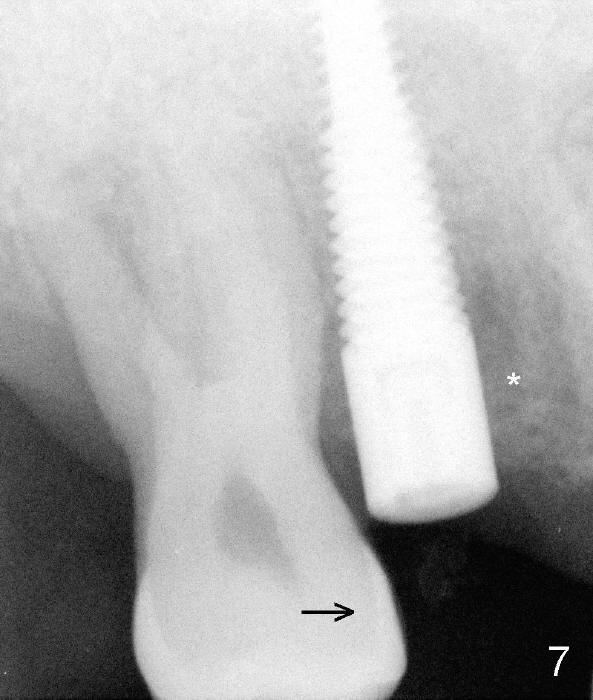
A 51-year-old man requests taking care of hemorrhage and odor associated with the tooth #3 (Fig.1). Due to religious and financial issues, the neighboring teeth will be treated later (supraeruption of #2 (arrow) and periapical radiolucency of #4 (*)). CBCT reveals that the septum of #3 is large enough to hold 4.5 mm implant (Fig.2). In fact osteotomy is created as planned in the septum using drills and taps (Fig.3 after removing 4.5x20 mm tap). Primary stability is obtained with a 4.5x20 mm implant (> 60 Ncm, Fig.4). The gap (*) is bone grafted; an abutment is placed (Fig.5 A); an immediate provisional is fabricated and cemented to cover the socket (Fig.6 P). When the socket heals in 3 weeks postop, the provisional and the abutment are removed for easy oral hygiene. Bone regenerates around the implant 3.5 months postop (Fig.7 *), but the 2nd molar has shifted mesially (arrow), presenting a restoration challenge.
Solution? An abutment is placed and a provisional crown with occlusal contact with the opposing is fabricated. A separator is placed between #2 and 3. Once a space forms, acrylic will be added the distal surface of the #3 temporary crown, which is then recemented. A new separator is used to create more space between these two teeth until #2 is distalized.
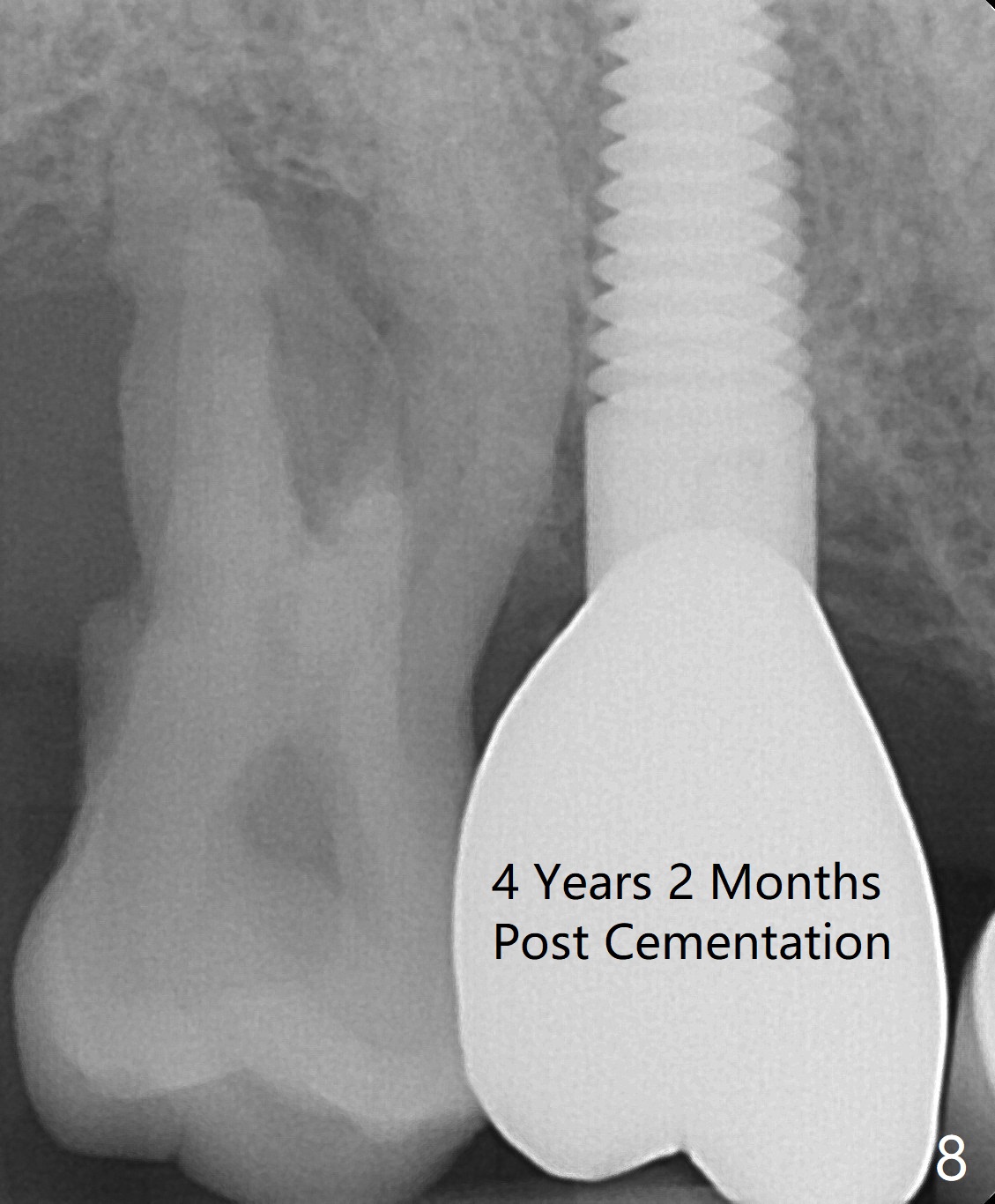
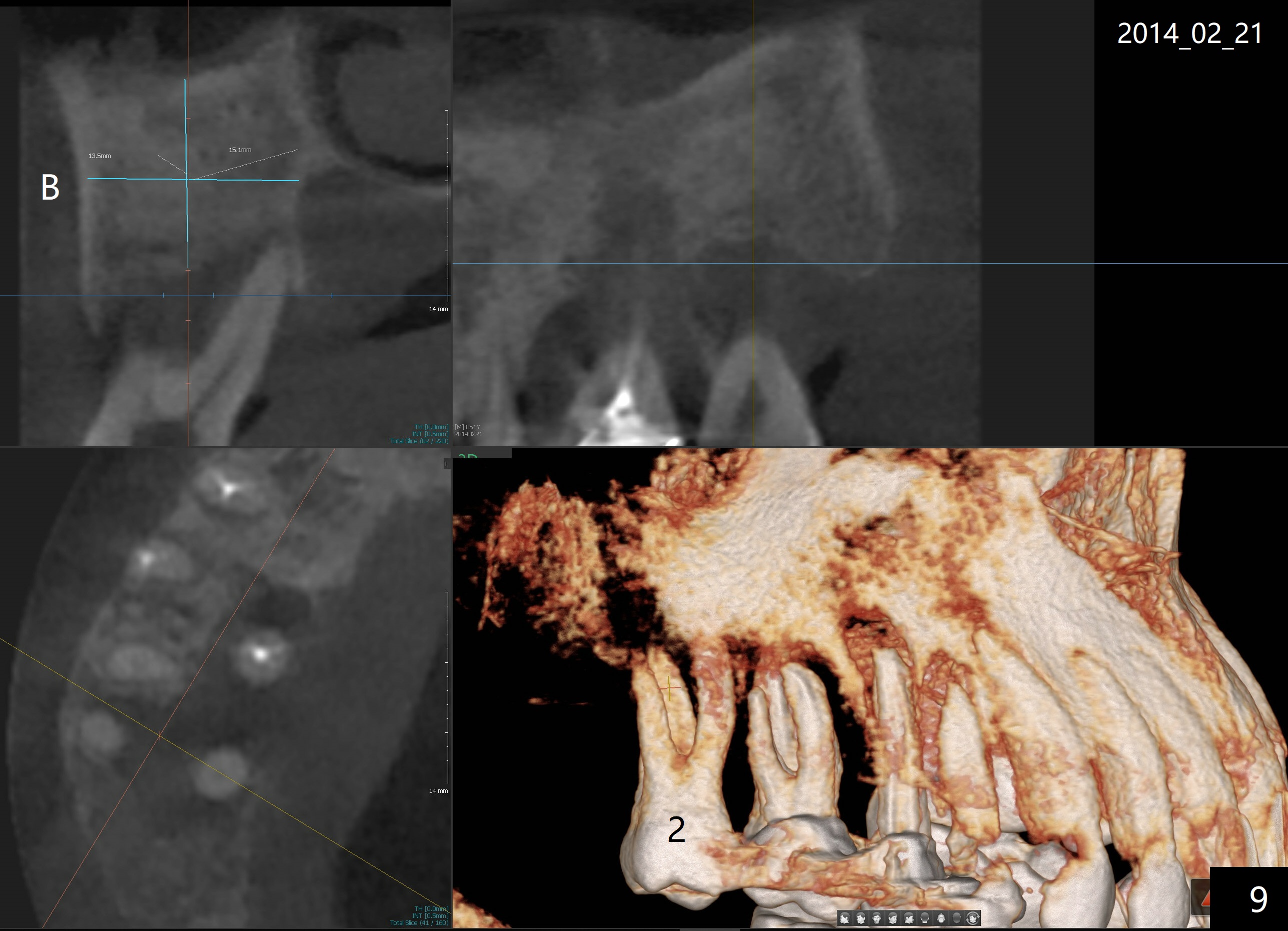
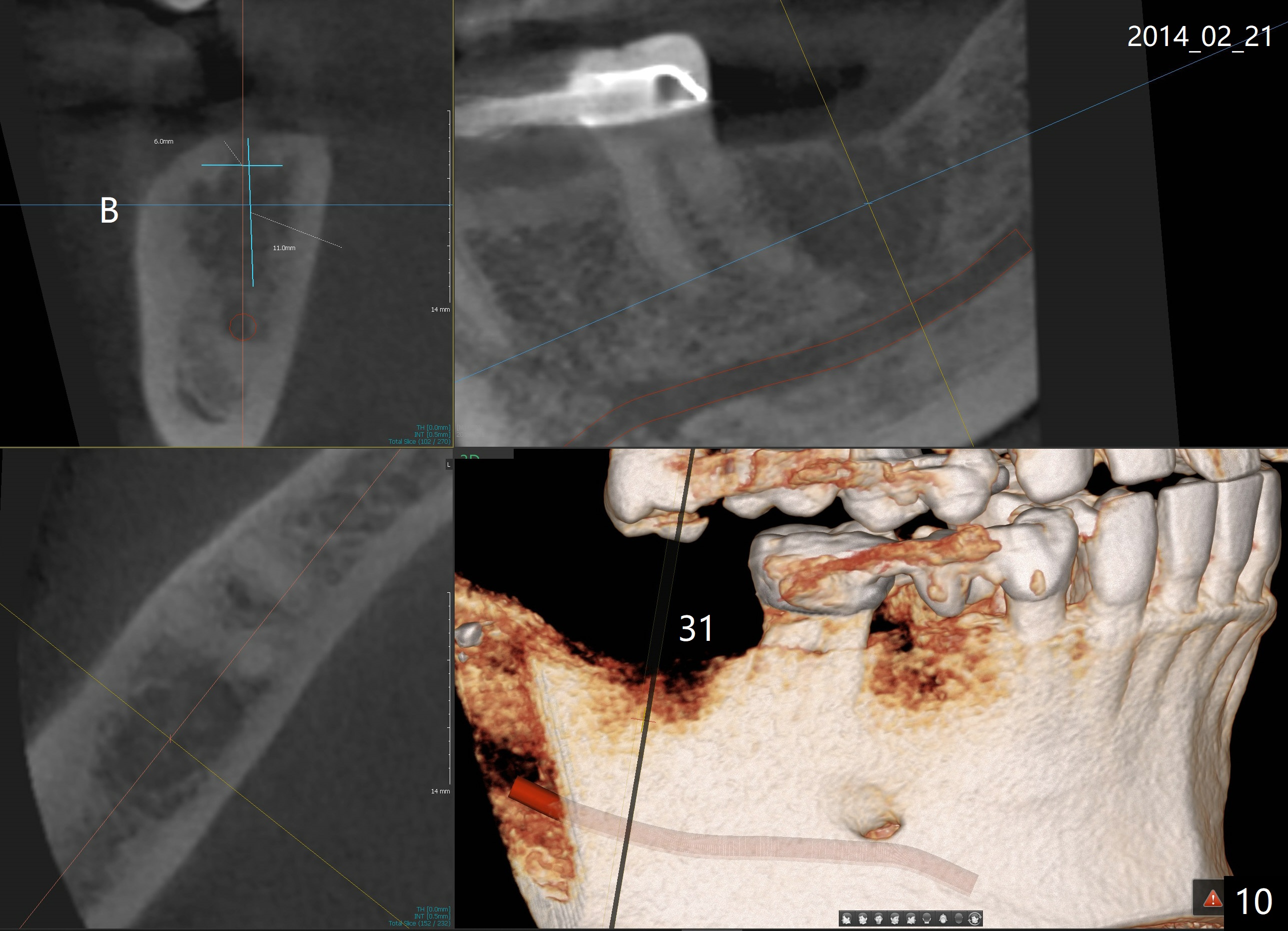
It appears that the upper molar shifting is quite common (6 7), probably due to less dense bone in the maxilla. It is the best to fabricate and keep an immediate provisional to hold the mesiodistal dimension and ask the patient to improve local oral hygiene during osteointegration. The implant crown is functioning 4 years 2 months post cementation while there is severe bone loss at #2 (Fig.8). An immediate implant could be placed at #2 (Fig.9), while a wide delayed implant will be placed at #31 (Fig.10).
Return to
Upper Molar
Immediate Implant
Posterior Immediate Provisional
Implant & Ortho
2
Xin Wei, DDS, PhD, MS 1st edition 09/28/2014, last revision 05/12/2019