

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Change Trajectory While Immediately Implanting
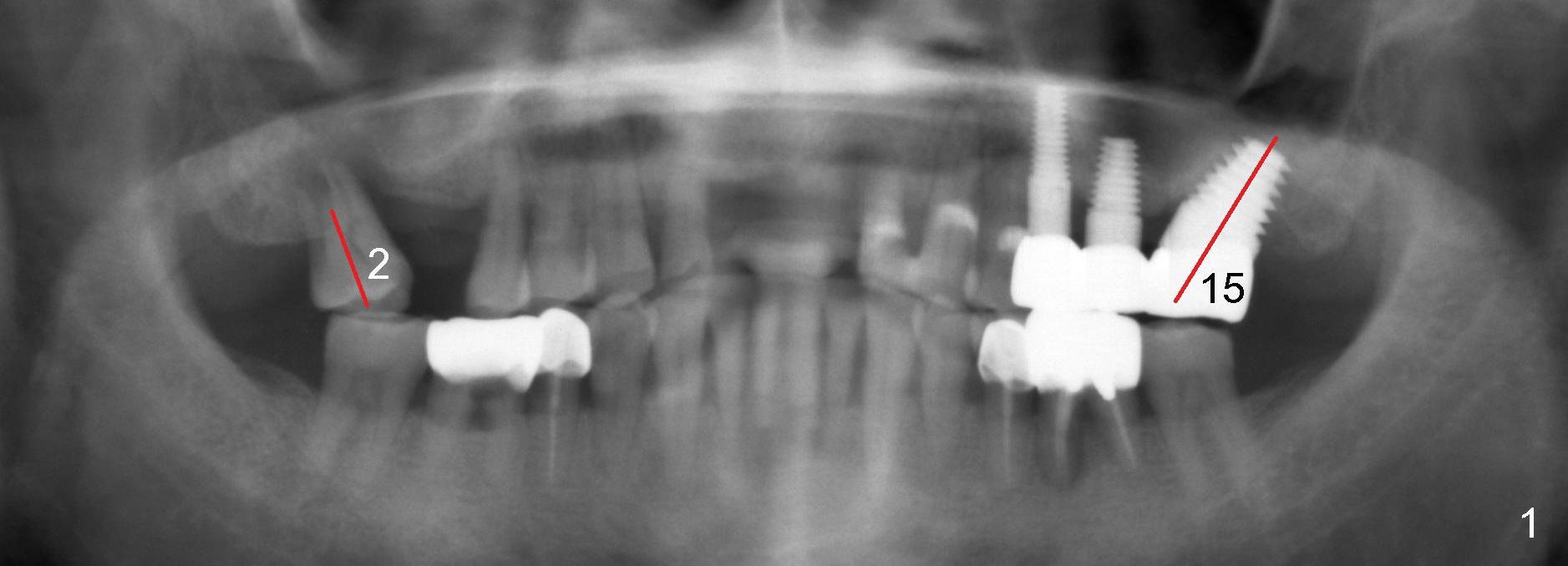
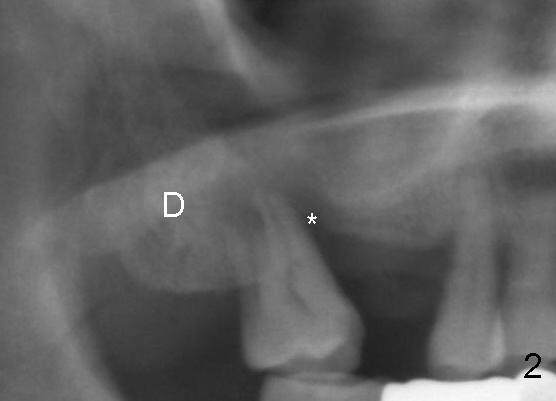
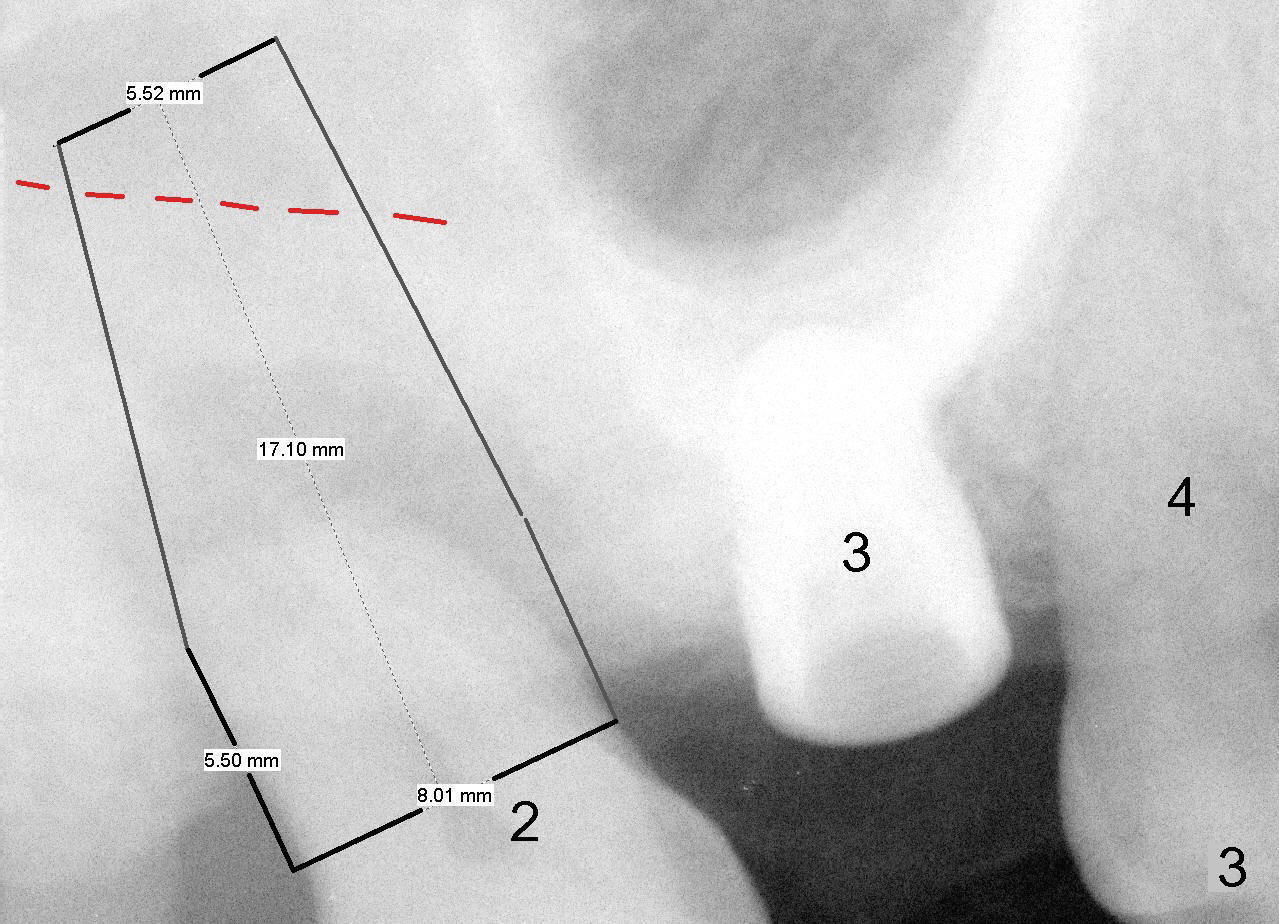
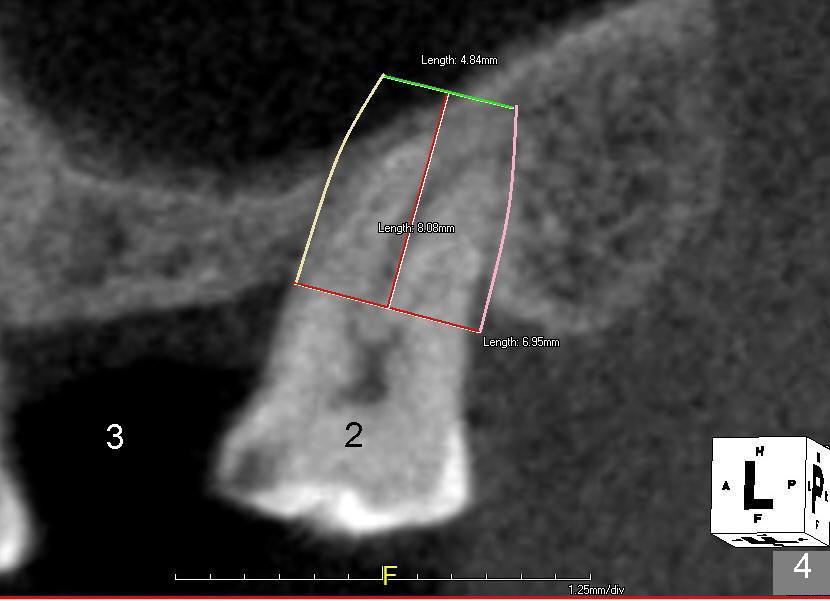
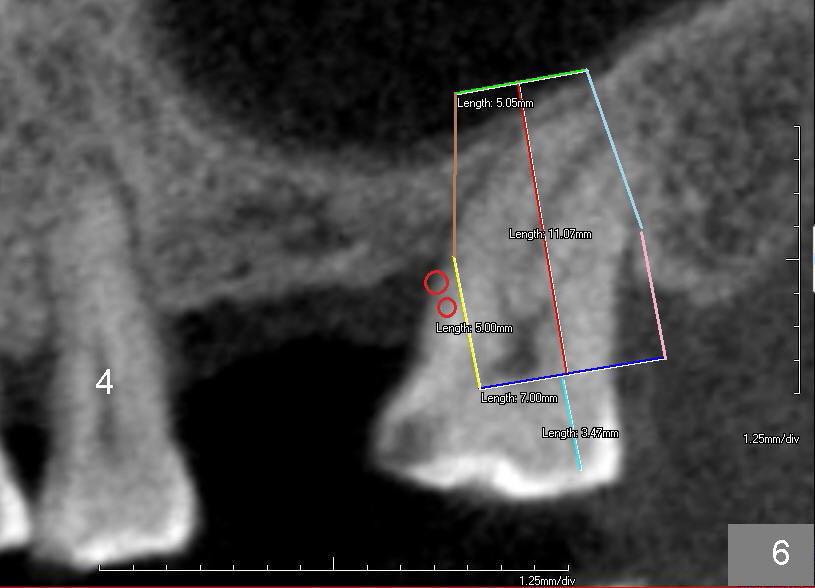
A 61-year-old man has chronic periodontitis and possible bruxism (Fig.1). Two years ago, the tooth #15 had severe bone loss as the tooth #2 has now. It was replaced by a 8x14 mm implant immediately with mesial tilt (Fig.1 red line). There is severe mesial bone loss of the tooth #2 (Fig.2 *) with mesial tilt (Fig.1 red line). Without reference to the big picture, an immediate implant for #2 tends to be placed with mesial inclination; sinus lift will be uneven with tendency of sinus membrane perforation (Fig.3,4).
In other word, the tooth #2 has been mesially tilted (Fig.5). The immediate implant should correct the axis; the apex of the implant evenly lifts the sinus floor (Fig.6). To make it easy, the first step is to place a cemented abutment at the site of #3, which was placed 5 months earlier. The abutment provides reference to parallelism.
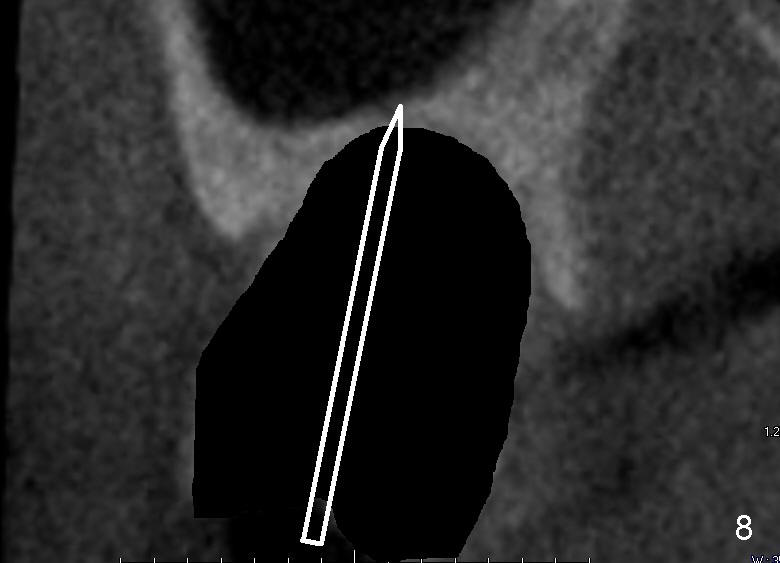
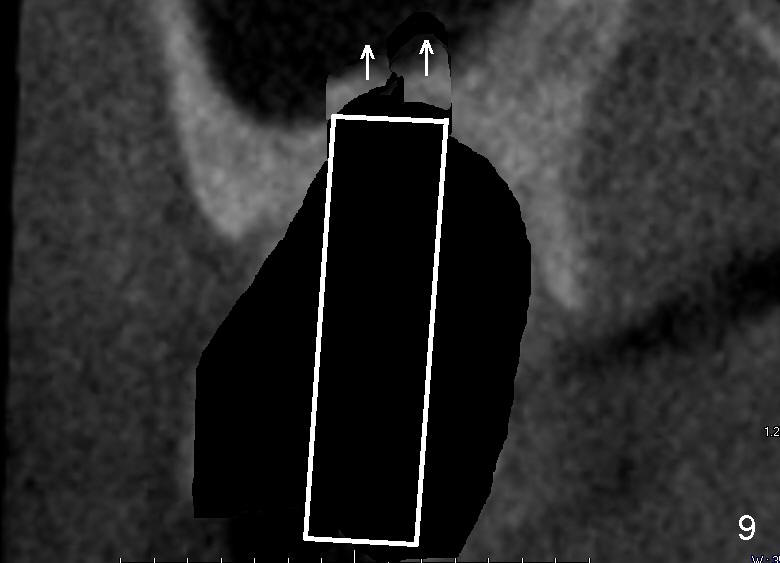
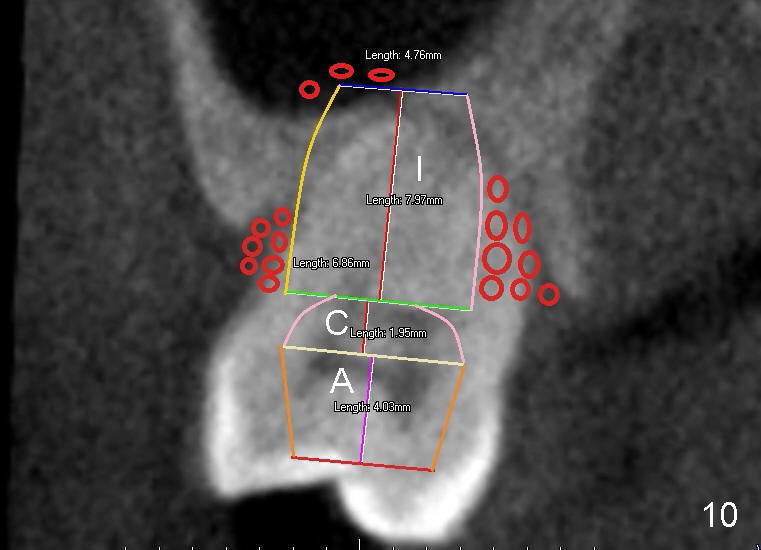
Fig.7 is a coronal section through the mesiobuccal and palatal roots of #2. There is minimal bone where sinus lift will be initiated with a pointed osteotome after extraction (Fig.8). The sinus floor is being gently and slowly lifted by enlarging osteotomes (Fig.9). The implant should be as large as possible to engage more bone buccally and lingually (Fig.10) and as long as possible (Fig.11). My plan is accomplished, but there is a new challenge.
Return to Upper Molar Immediate Implant,
Posterior Immediate Provisional,
Immediate
Implant Complications
Xin Wei, DDS, PhD, MS 1st edition 01/11/2015, last revision 12/20/2015