



|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
Buccolingual (B-L) Trajectory
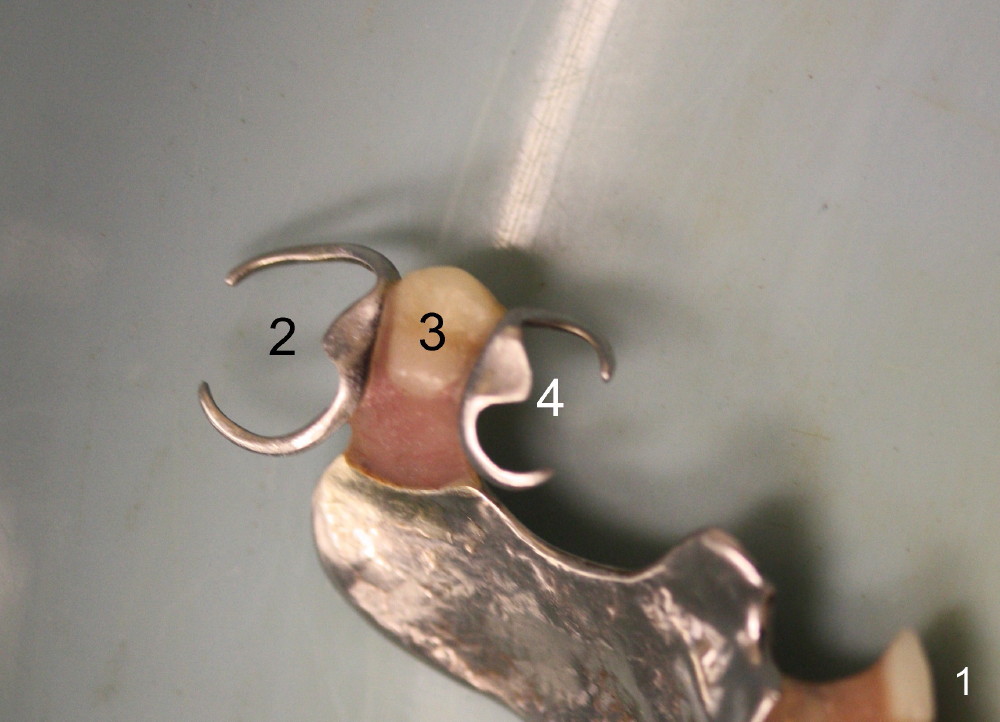
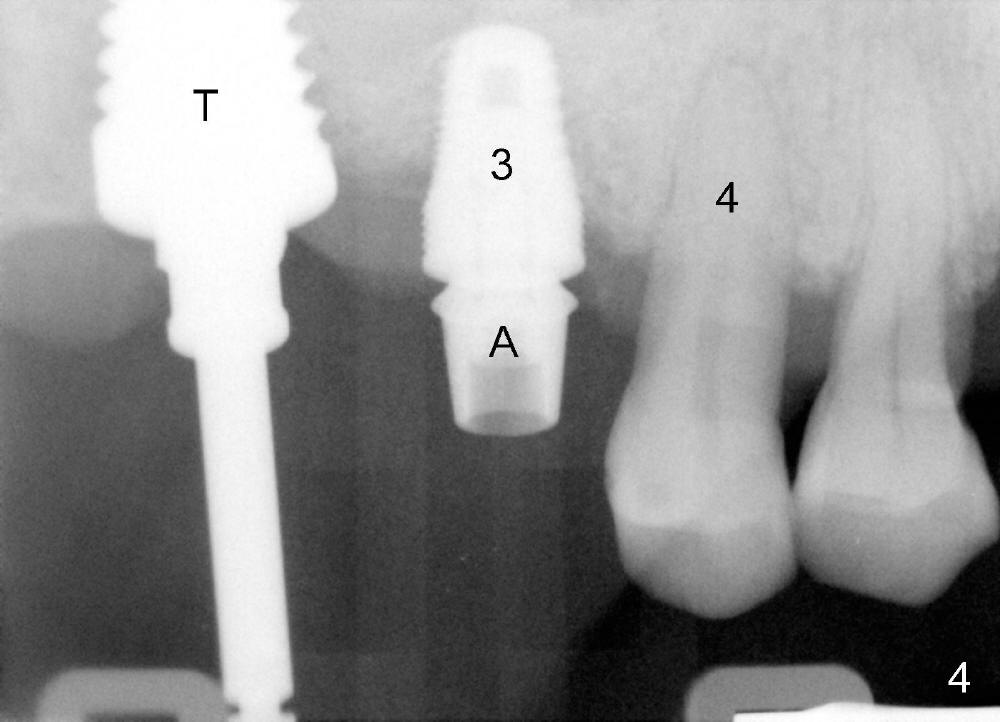
Treatment plan dictates attention paid to the mesiodistal (M-L) trajectory of the tooth #2. In fact after modification of the upper partial denture (Fig.1-3) and extraction, the axis of the 8x17 mm tap (Fig.4,5) and implant (Fig.6,7) at the site of #2 is parallel to those at #3 and 4. But the B-L trajectory is neglected initially and corrected to certain degree as to be shown below. Immediate provisonals at the sites of #2 and 3 are fabricated (splinted) and adapted to the modified partial (Fig.8).
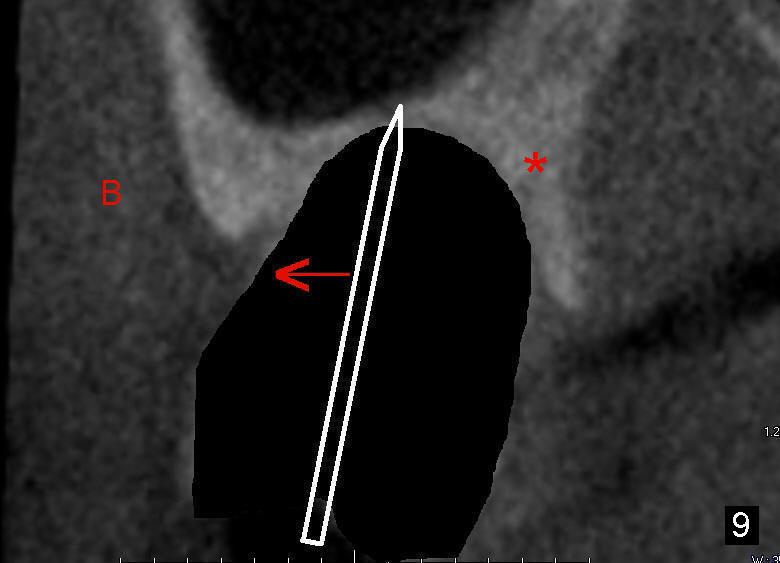
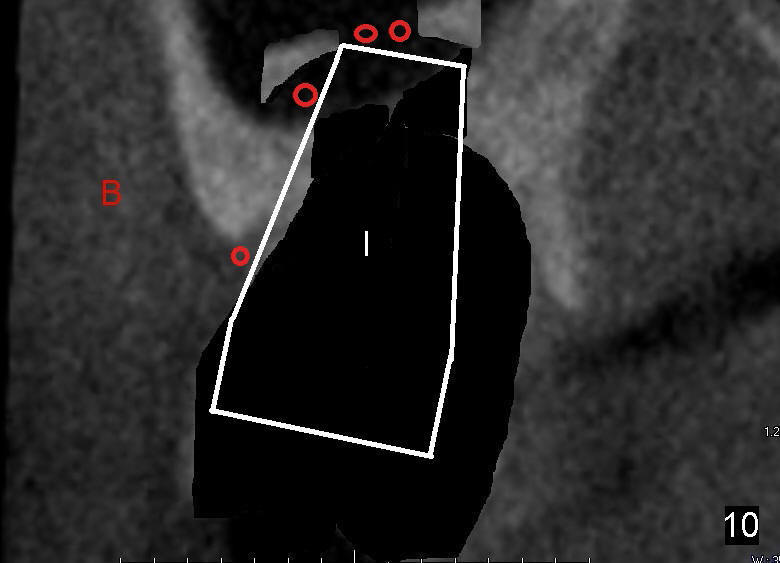
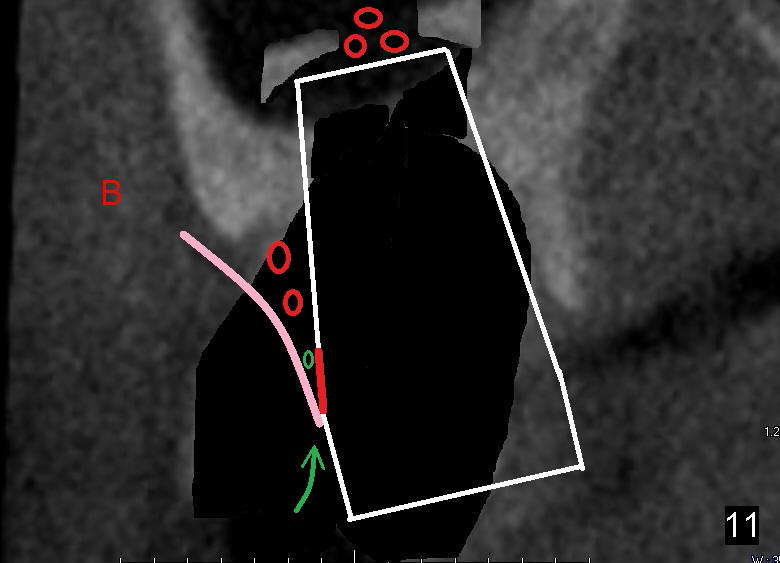
After extraction and curettage, osteotomy is initiated by osteotomes (2-4 mm in diameter). The smallest osteotome tends to slide buccally (Fig.9 CT coronal section of socket). When the implant is being placed, it is inclined buccally excessively (Fig.10 B). It has to be backed up, and redirected (Fig.11). The buccal threads (red line) are barely apical to the gingiva (pink curved line). The space between the gingiva and the implant is so limited that it is difficult to insert (curved green arrow) bone graft (green circle). Red circles represent bone graft placed before implant placement.
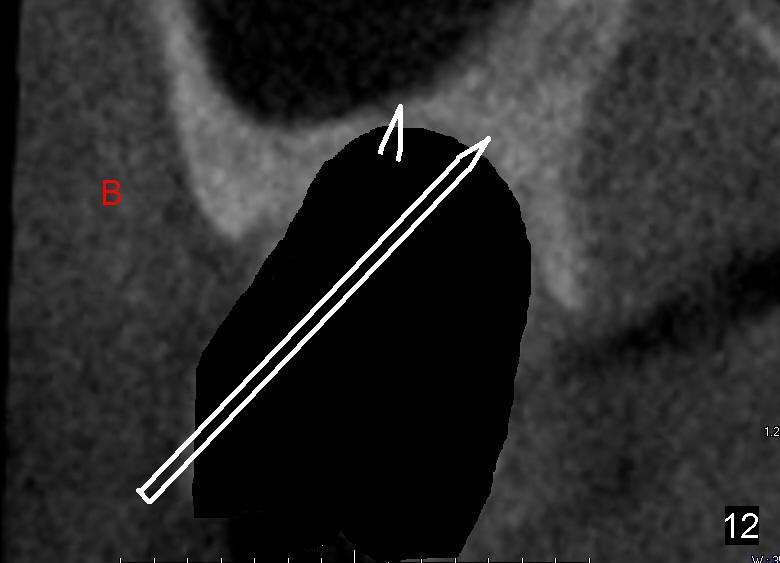
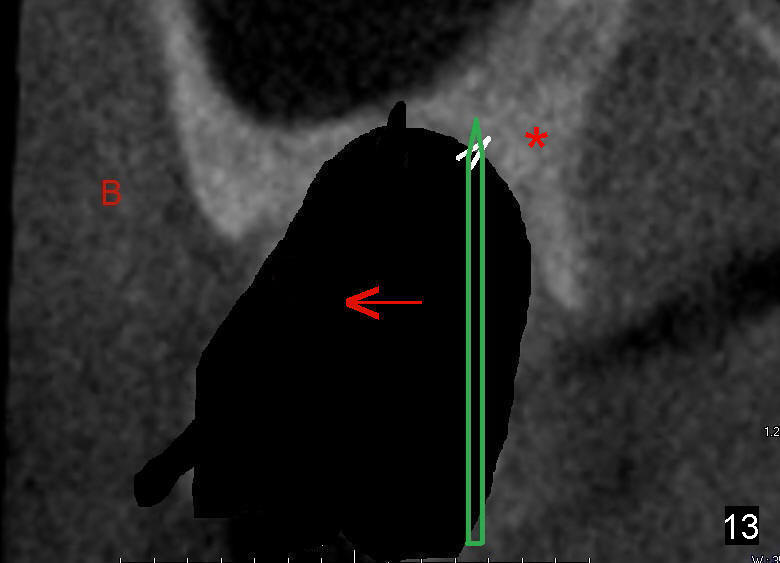
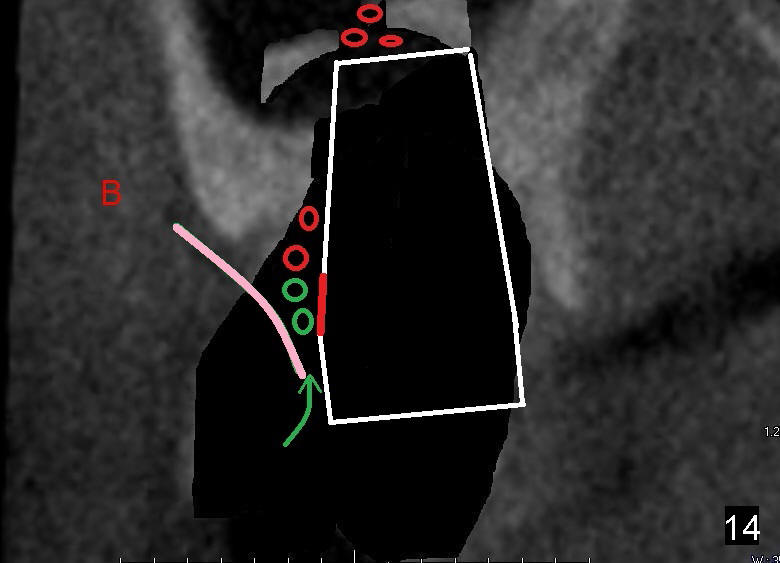
Retrospectively, it is the best to use a sharp pilot drill to start osteotomy, since it is less likely to slide. Furthermore, the initial osteotomy should be as lingual as possible (Fig.12 long arrow, as compared to short one). Once the pilot drill gets its entrance into the bone, the trajectory should be changed (Fig.13 green arrow). As drills or osteotomes increase their diameter, they also tend to move buccally (red arrow) due to dense and thick palatal bone. The implant is most likely placed in a good trajectory and position (Fig.14). The gap between the buccal gingiva and the implant is large enough (green arrow) to supplement bone graft (green circle) after implant placement, if necessary. In other word, the most coronal buccal threads (red line) will be covered by bone graft.
Therefore implant placement is a game of 3 D manipulation. Place an implant as palatal as possible to get engagement into the palatal bone, since it is usually longer, thicker and denser than the buccal bone. Do not use an oversized implant to reduce the chance of buccal thread exposure. In this case, 7 mm is probably better than 8 mm.
In fact, the implant exfoliates 2 months later.
Return to Upper Molar Immediate
Implant,
Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 01/17/2015, last revision 03/29/2015