
_bone%20graft.jpg)


.jpg)
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Possible Buccal Plate Perforation at the Site of #9
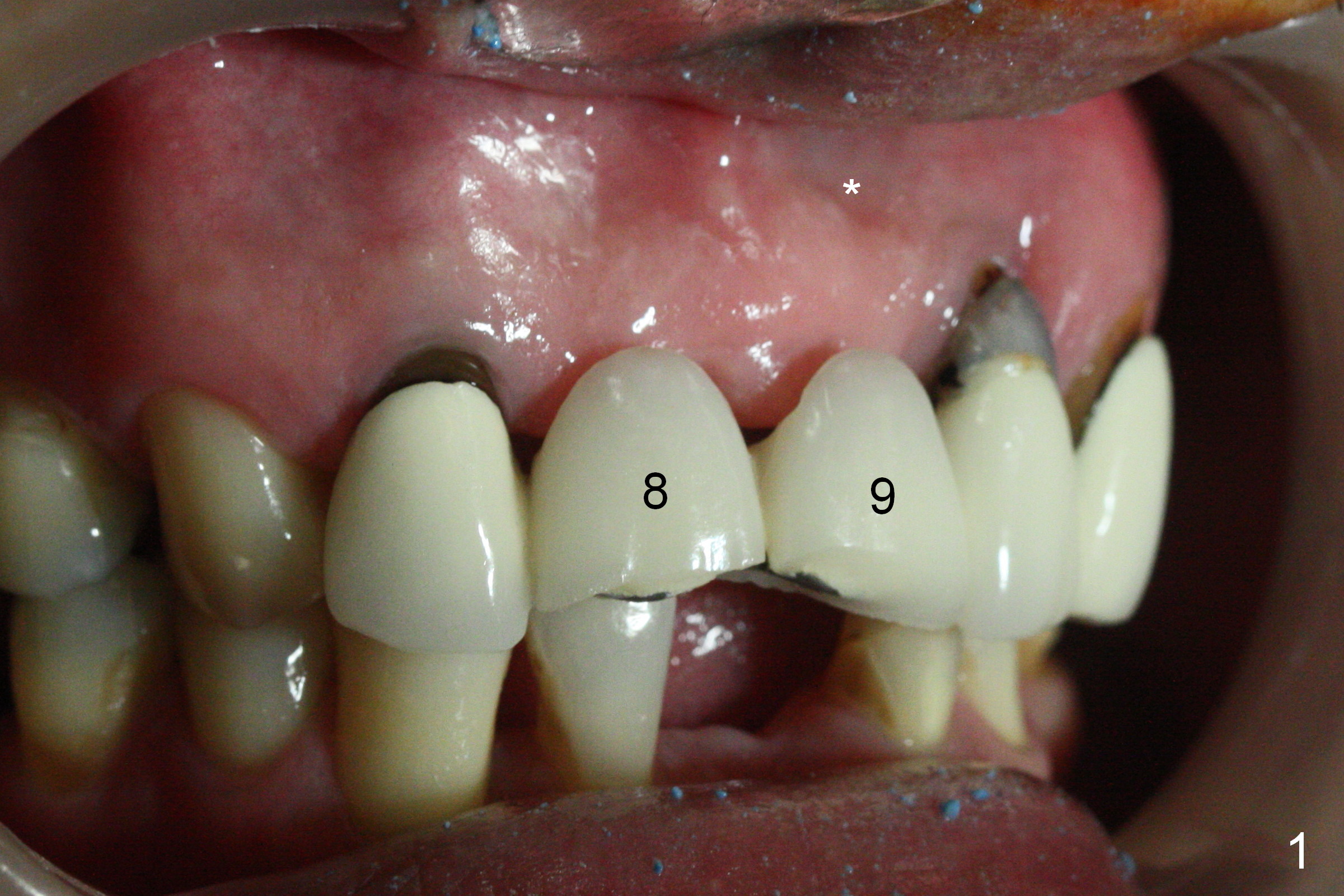
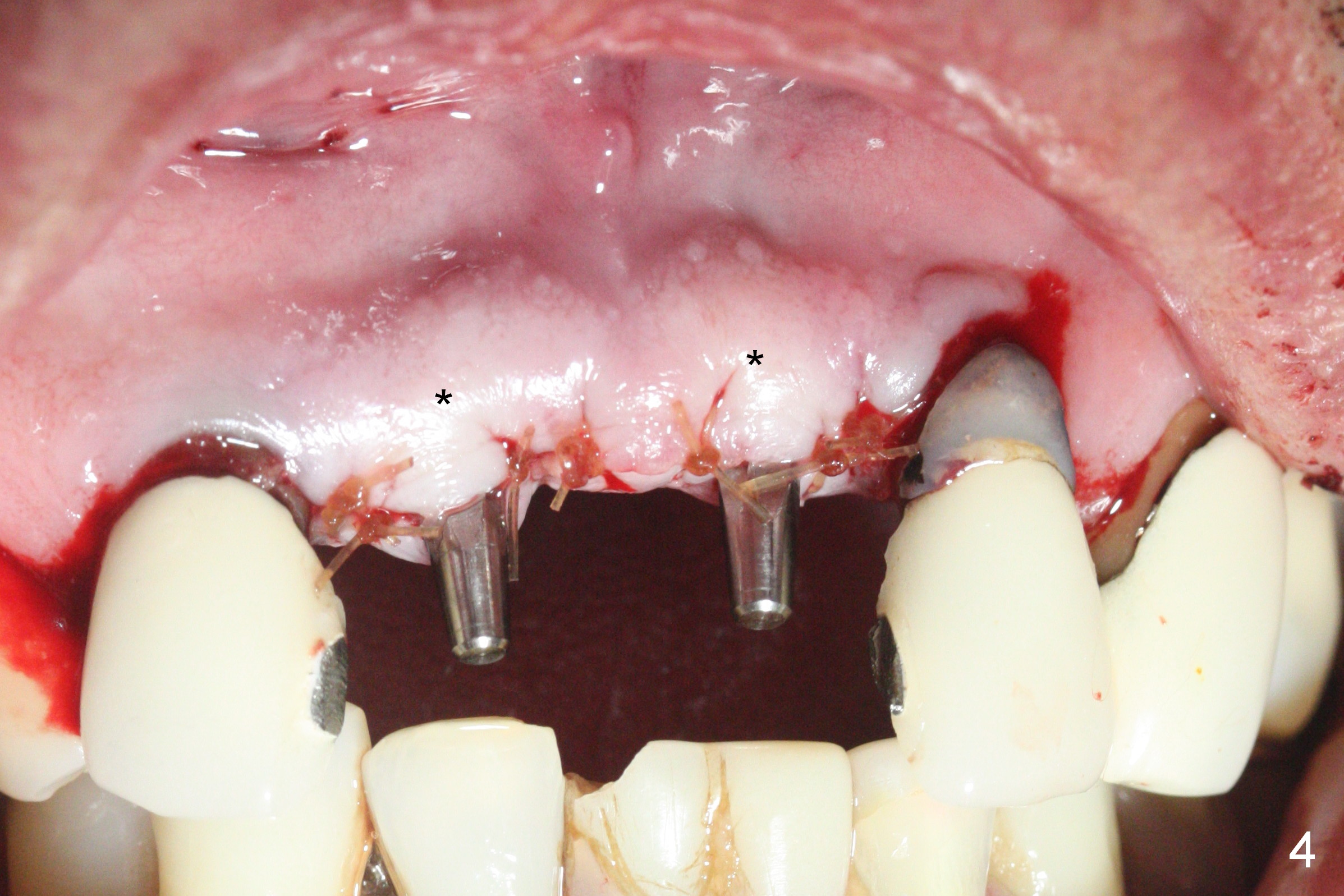
Note the apical buccal concavities at the sites of 8 and 9 (Fig.1 *). The severity of the ridge atrophy is manifested by the buccalized Incisive Papilla (Fig.2 *) after pontic removal. Following incision, the initial osteotomy with 1.2 mm pilot drill appears to perforate the buccal concavity at #9. When the osteotomy is redirected, the buccal plate vibration is undetectable. The insertion torque at #9 is <25 Ncm, while that at #8 is >45 Ncm with the same 1-piece implants (Fig.3,4: 2.5x14(2) mm). The postop buccal plates at #8 and 9 look bulging, probably associated with bone graft and collagen membrane placement (Fig.4 *). The patient returns 2 weeks postop with concern over a palatal swelling, which in fact apparently does not exist. There is palatal perforation of the provisional palatal to #8. The abutment at #8 is adjusted (Fig.5); the provisional is relined and recemented (Fig.6). Gingival recession at the tooth #10 remains in spite of trimming of excessive composite (*, as compared to Fig.1,4). The retainers will be sectioned between #10 and 11 to determine whether the tooth #10 is salvageable or not.
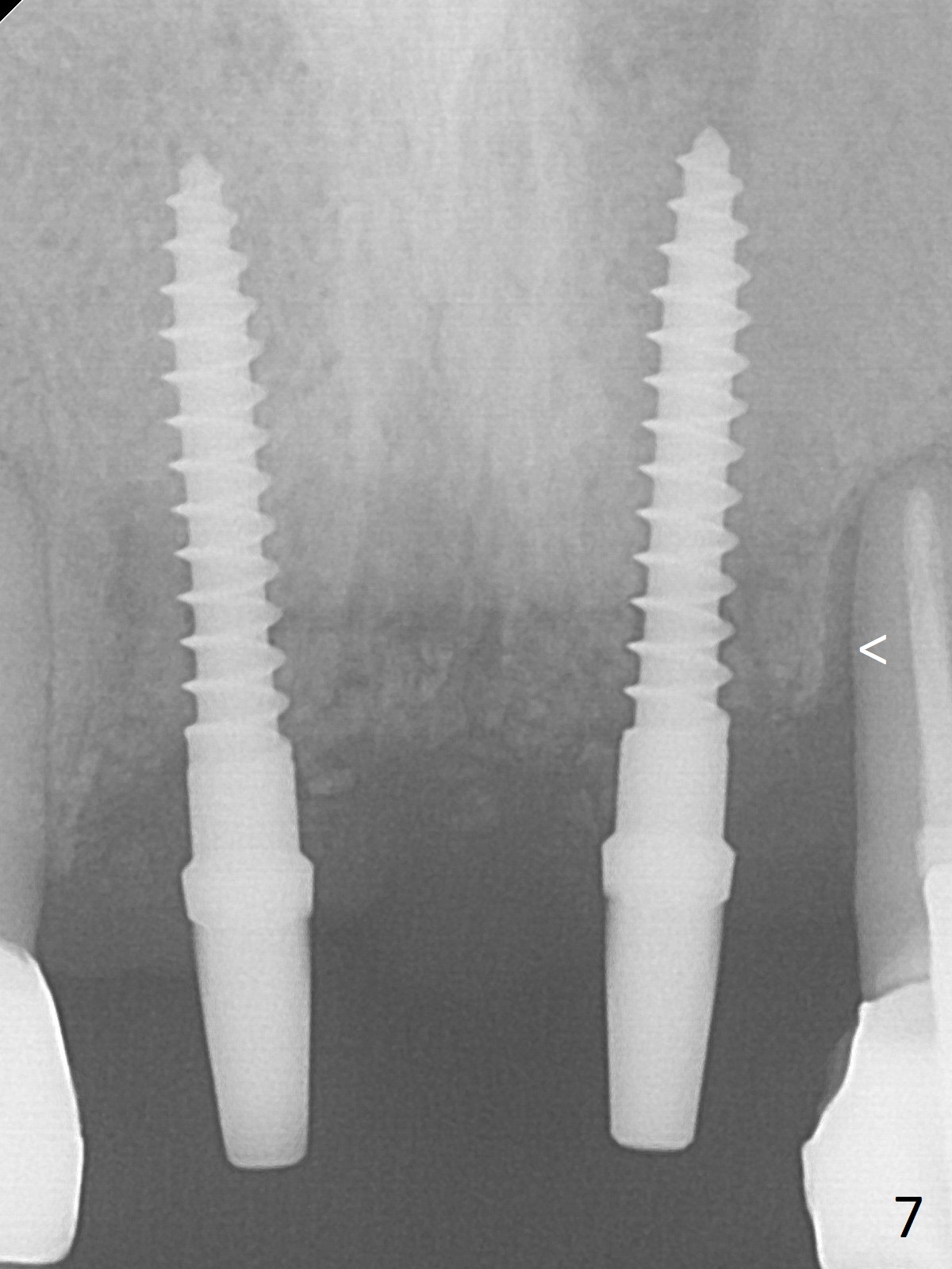
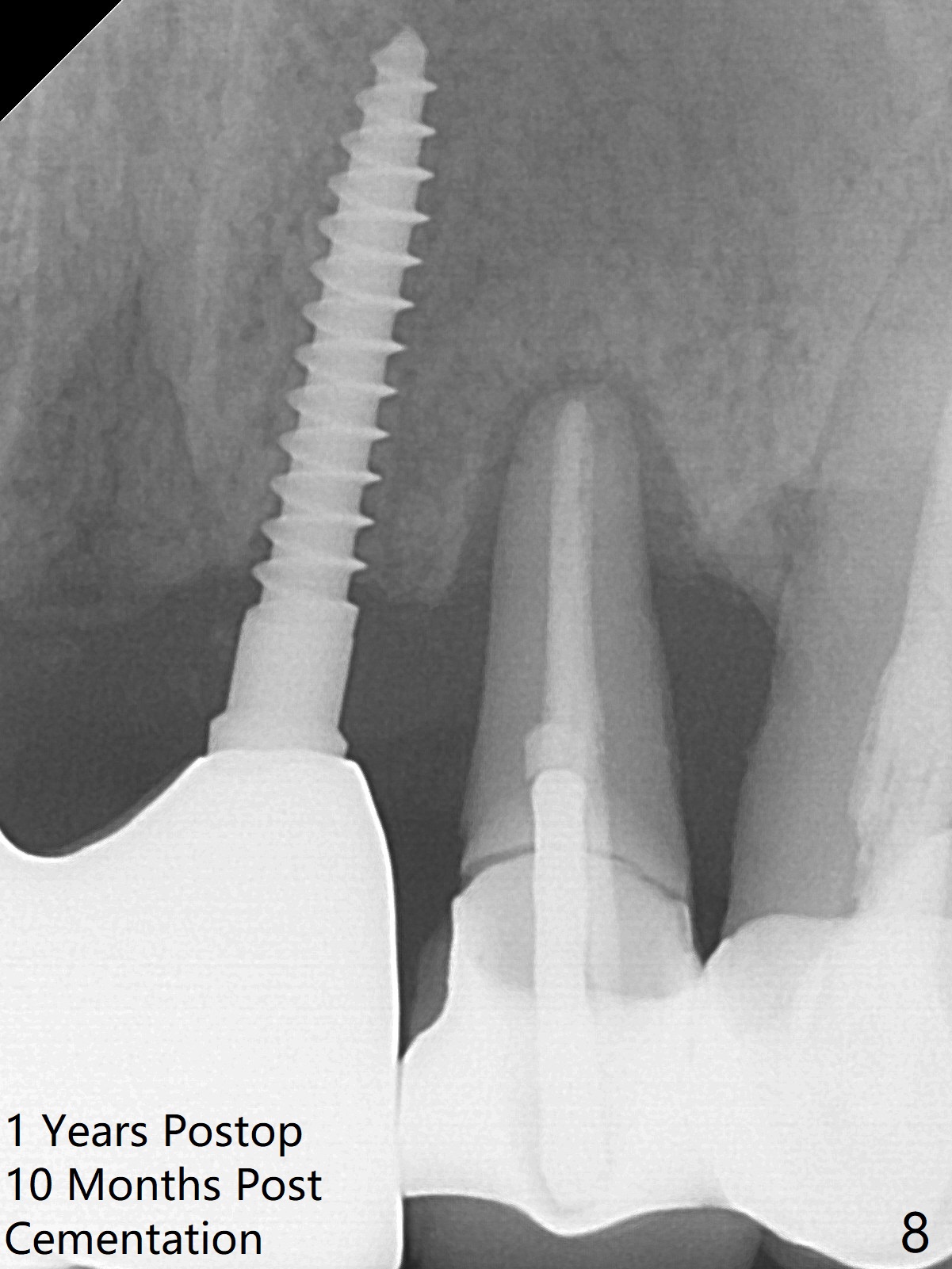
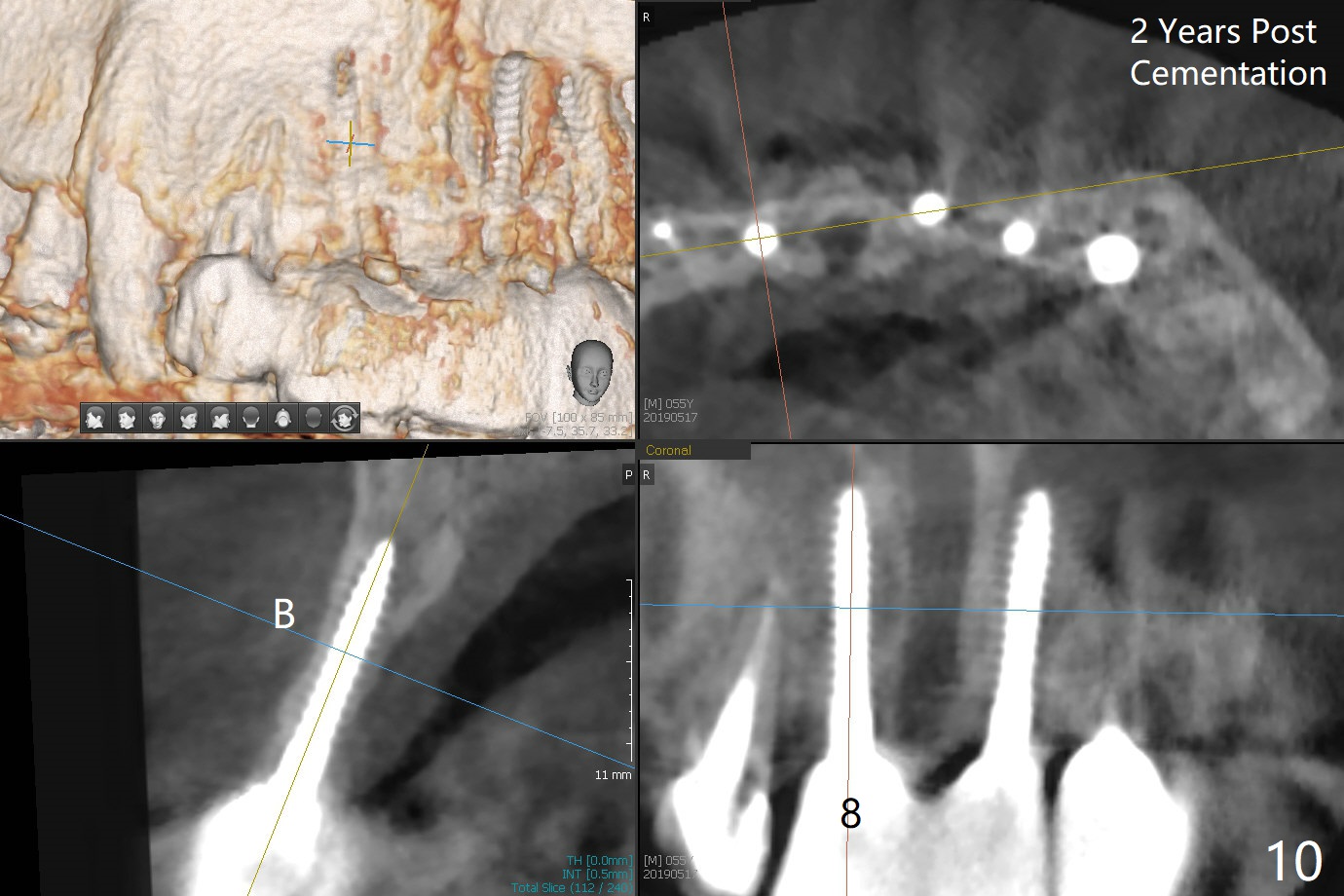
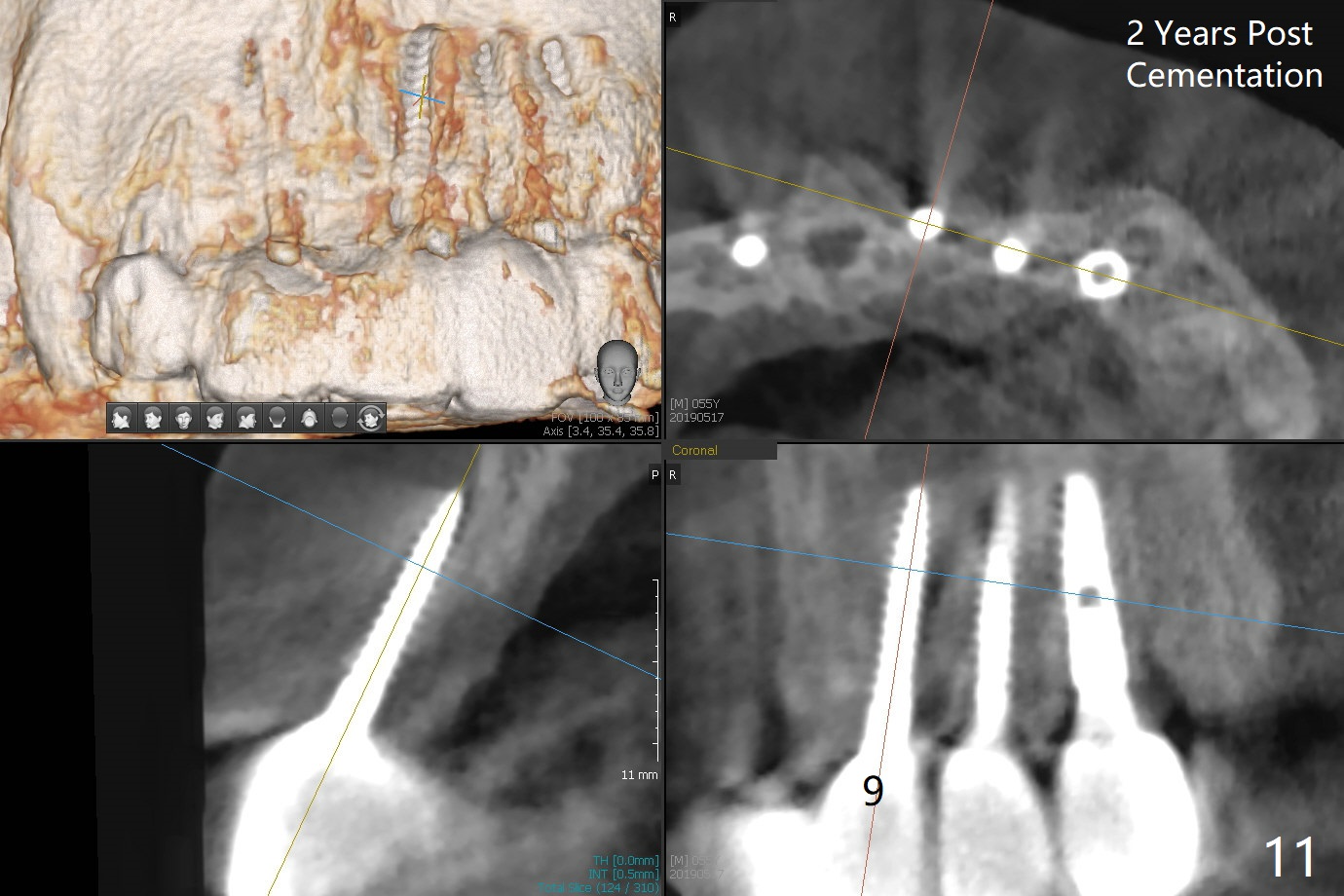
Since the patient is going to travel abroad, he wants to have definitive restoration as soon as possible (Fig.7: 1 month 3 weeks postop). After gingival retraction cords, the implant at #9 is found unstable. Impression is taken for splinted restoration. The tooth #10 has increased periodontal ligament space (<), while the crowns at #14 and 15 have not cemented. Ten months post cementation, the splinted crowns at #8 and 9 remain stable with healthy gingiva; it appears that the tooth #10 needs extraction and implant (Fig.8,9). Take photos preoperatively to show the healthy gingiva around #8 and 9 splinted crowns. CT taken 2 years post cementation shows that the implant at #8 is placed in the middle of the alveolus (Fig.10 (B: buccal)), while the one at #9 is buccal (Fig.11). A smaller (2.0 mm) and shorter (10 or 12 mm) implant may reduce the chance of buccal perforation.
Return to
Upper
Incisor Immediate Implant,
Full Arch Reconstruction,
IBS,
Armaments,
Atrophic Ridge
Xin Wei, DDS, PhD, MS 1st edition 02/17/2017, last revision 05/23/2019